
Translate this page into:
Declining prevalence of pulmonary paragonimiasis following treatment & community education in a remote tribal population of Arunachal Pradesh, India
Reprint requests: Dr Kanwar Narain, Regional Medical Research Centre, N.E. Region (ICMR), Post Box #105, Dibrugarh 786 001, Assam, India e-mail: kanwar_narain@hotmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
In India, human pulmonary paragonimiasis is an important public health problem in the northeastern (NE) region. In 2005 we reported a hyperendemic focus of paragonimiasis in a remote tribal village in the hills of Changlang district in Arunachal Pradesh. The community was made aware of the disease and all active cases were treated. This study was aimed to assess the decline in the prevelance of paragonimiasis in the same area after a re-survey done in 2011 after a gap of six years.
Methods:
Re-surveys were carried to determine the reduction in the prevalence of paragonimiasis. Community education was given to the villagers to raise their awareness about paragonimiasis. A total of 624 individuals including 301 children (age < 15 yr) were included in the study. Sputum and stool samples were examined for eggs of lung flukes. Serum samples were screened for IgG antibodies against lung fluke antigen by ELISA.
Results:
A significant (P<0.001) decline in the prevalence of paragonimiasis was found. There was decline in both ELISA positivity and egg positivity. Antibody positivity against excretory-secretary (ES) antigen in children (age ≤ 15 yr) fell down from earlier 51.7 to 15.9 per cent and in individuals 16 - 30 yr of age the serological prevalence fell down from 22.4 to 8.2 per cent and in individuals aged ≥ 31 yr, the decline in prevalence was from 15.3 to 3.7 per cent. Gender-wise analysis revealed that the decline in ELISA positivity was similar in both genders and fell down from 33.9 to 11.5 per cent in males and from 29.8 to 10.7 per cent in females. Similarly, there was a significant decline rate in egg positivity also.
Interpretation & conclusions:
The strategy of hotspot targeted active paragonimiasis case detection and treatment of infected cases together with community education appears to be feasible methods to achieve control of paragonimiasis in this region.
Keywords
Community education
paragonimiasis
prevalence
treatment
tribal

Paragonimiasis is an important neglected tropical disease. Among food-borne trematodes, the lung fluke infection costs more in terms of disability adjusted life years (DALYs) than opisthorchiasis, fascioliasis, and intestinal diastome infection combined1. An estimated 293 million people are at risk of paragonimiasis worldwide2 and it has been reported that about 23 million people in 48 countries are infected34. In India, human pulmonary paragonimiasis is emerging as an important public health disease in northeastern (NE) region567891011. The parasite is zoonotic, cycling through wild carnivorous mammals, freshwater snails, crabs or crayfish. Interest in paragonimiasis has increased partly because the symptoms closely mimic those of tuberculosis, frequently leading to inappropriate treatment being administered to smear negative suspected TB cases. Failure of patients to respond to treatment may lead to inflated estimates of the prevalence of multi-drug resistant tuberculosis and may have other far-reaching health implications121314. The distribution of paragonimiasis is highly heterogeneous and a few hotspots of transmission foci can be recognised in NE region. Earlier we reported a hyper-endemic focus of paragonimiasis in a remote tribal area in the hills of Changlang district of Arunachal Pradesh7. During that active survey carried out in 2005 in the community all the infected patients were treated with praziquantel. The villagers were also given awareness about paragonimiasis and various preventive measures. Subsequently, we carried out a re-survey in 2011 with an aim to determine whether household screening and treatment of infected individuals together with imparting community education could decrease the prevalence of paragonimiasis in this highly endemic focus of paragonimiasis after an interval of six years.
Material & Methods
Study area: This study was conducted by the Regional Medical Research Centre (RMRC), Dibrugarh, Assam jointly with community health centre (CHC), Miao, in the five villages of Changlang district of Arunachal Pradesh where paragonimiasis was found to be highly endemic based on cross-sectional surveys conducted earlier by us7. The study area is economically underdeveloped and predominantly hilly with extensive forests and is located at an elevation of 200-4500 m above sea level. Furthermore, these villages are located in remote areas without proper roads and communication. The nearest community health centre is at Miao and can only be approached by foot from the selected study villages. The inhabitants of these villages are predominantly tribal and their primary occupation is subsistence farming.
Sample size and sampling methodology: The re-surveys were carried out during 2011 in the five villages, of Changlang district following the same strategy as used earlier7. The two study samples were independent. We assumed a null hypothesis of no change in the prevalence of paragonimiasis as assessed in earlier cross-sectional survey7. In order to detect at least 10 per cent decline in the seroprevalence (from 50 to 40%) at 5% level of significance and 90% power, the required sample size was 515 subjects. However, we included a total of 624 individuals including 301 children (age < 15 yr). The households were randomly selected and all individuals in the selected households were included. Information on age, sex, history of cough, crab eating habits was recorded. Written informed consent was obtained from all the persons or their guardians in case of children. The study protocol was approved by the ethics committee of RMRC, Dibrugarh. Blood and stool samples were collected from all the individuals and those with cough also provided the sputum samples. The sputum and stool samples were collected in duplicate and examined for characteristic operculated eggs of lung flukes under light microscope. In addition, the sputum samples were examined for acid fast bacilli (AFB) using Ziehl–Neelsen (Z-N) staining to exclude tuberculosis. IgG antibodies against excretory-secretory (ES) antigen of adult lung flukes were detected using enzyme-linked immunosorbent assay (ELISA) as previously described715. Known positive and negative reference serum samples were included in each ELISA test to monitor quality control. A sample was considered positive if the OD was 0.49 or more.
Statistical Package for Social Sciences (SPSS) version 17 (SPSS Inc., Chicago, Illinois, USA) was used for data entry and analysis. Chi square test was used to compare the prevalence of infection in different age groups and gender.
Community education: Community education was given to the villagers to make them understand the mode of transmission of paragonimiasis. Information regarding the risky food habits which could facilitate transmission of paragonimiasis was also given to the inhabitants of the study villages. Focus group discussions and in-depth interviews were carried out in the study villages during earlier surveys. The participants included the village headman, adult community members (both men and women) and also children. People were also educated about maintaining proper hygiene. Charts and photographs were shown to the villagers to make them understand the life cycle of the lung flukes. The people were also advised to seek medical attention at community health centre (CHC), Miao, if they had persistent cough for more than two weeks with or without haemoptysis.
Clinicians and health care providers of the community health centre of Changlang district at Miao were also informed about the existence of a highly endemic focus of paragonimiasis in their catchment area. All the infected subjects who were sputum or stool egg positive for paragonimiasis were given praziquantel treatment (25mg /kg body weight given orally three times per day for 2 consecutive days)16 at CHC, Miao. All treated subjects were re-examined and their sputum or stool samples were re-tested after 15 days to one month of treatment for confirming the success of treatment.
Results
The results of this study showed that there was a significant (P<0.001) decline in the prevalence of paragonimiasis as revealed by the decline in both ELISA positivity (Fig. 1) and egg positivity (Fig. 2). Antibody positivity against ES antigen in children fell down from earlier 51.7 (n=263) to 15.9 per cent (n=305) and in individuals 16-30 yr of age the serological prevalence fell down from 22.4 (n=196) to 8.2 per cent (n=185) and in individuals aged 31 yr and above, the decline in prevalence was from 15.3 (n=216) to 3.7 per cent (n=134). Gender-wise analysis revealed that the decline in ELISA positivity was similar in both genders and fell down from 33.9 (n=292) to 11.5 per cent (n=275) in males and from 29.8 (n=383) to 10.7 per cent (n=349) in females. In children (age < 15 yr) egg positivity fell down from 20.9 to 3.6 per cent and from 7.1 to 1.6 per cent in individuals 16-30 yr of age. However, there was statistically no difference in the prevalence of egg positivity in individuals 31 yr and above (1.5 vs 2.2%). Gender-wise analysis revealed that there was significant reduction rate in the egg positivity in both male and female subjects (from 10.3 to 3.1% in males and from 11.0 to 2.01% in females). Sputum smear examination revealed that sputum samples from two of the 170 cases examined, were positive for AFB. These cases were referred to the CHC for pulmonary TB treatment.
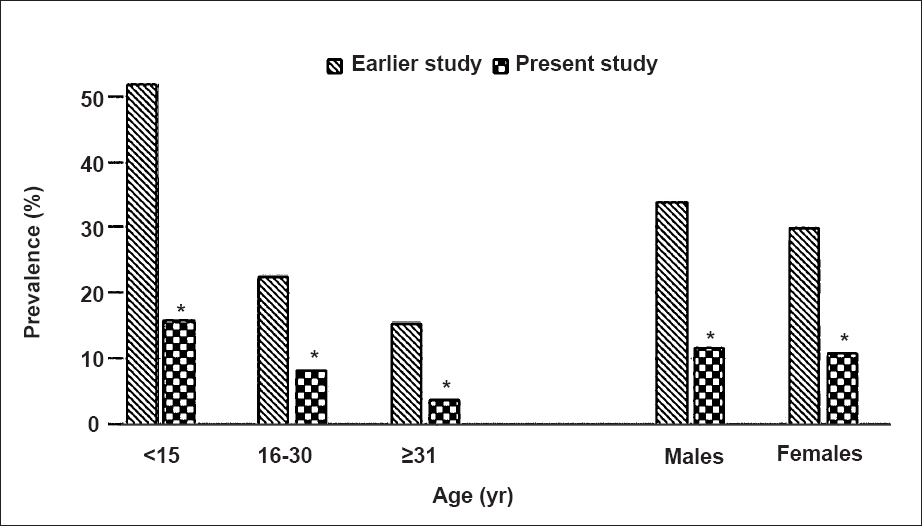
- Bar diagram showing decline in the prevalence of paragonimiasis based on ELISA positivity (age-group and gender-wise comparison of pre- and post-intervention data). (Souce for pre-intervention data: Ref. 7). *P<0.001 compared with earlier study.
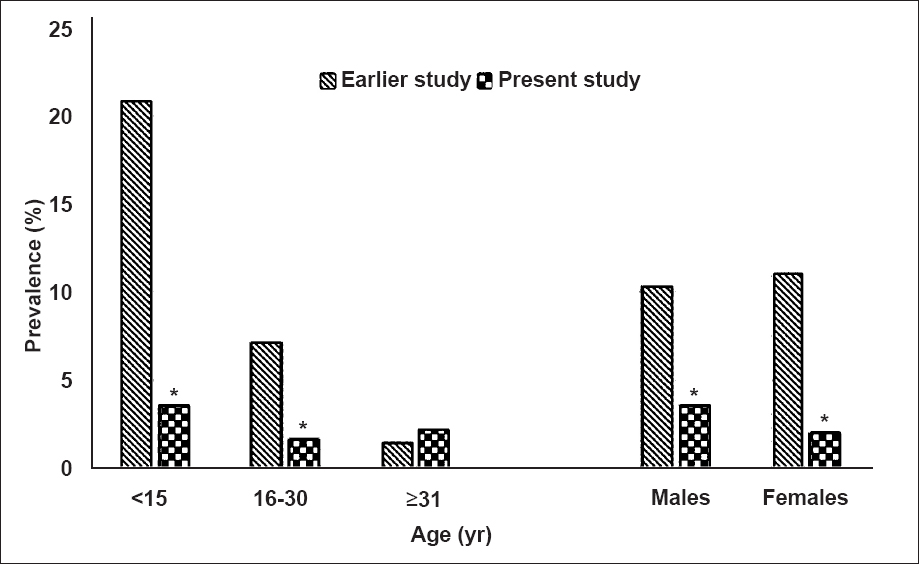
- Bar diagram showing decline in the prevalence of paragonimiasis based on sputum egg positivity (age-group and gender-wise comparison of pre and post-intervention data). (Souce for pre-intervention data: Ref. 7). *P<0.001 compared with earlier study.
Discussion
The present study revealed a significantly different picture of paragonimiasis in Changlang district of Arunachal Pradesh than the one appeared in 20077. The prevalence of paragonimiasis both in terms of seropositivity and egg positivity has declined substantially. The results of this study should be a reason for cautious optimism that pro-active case detection and treatment of paragonimiasis cases together with community education can significantly reduce this food-borne disease in highly endemic and difficult to access foci and ultimately may contribute to the elimination of paragonimiasis in NE region. This strategy of hotspot targeted active case detection and treatment of infected cases together with community education for raising the awareness about paragonimiasis appears to be a feasible method for controlling paragonimiasis in remote and difficult to access foci.
In northeastern India paragonimiasis mostly affects communities who have very limited economic development and reside in the remote hilly and forested areas with poor access to health care facilities6713. Although paragonimiasis is clinically important17, yet it is a neglected food-borne trematode infection in NE region of India. Various factors like lack of education, poverty, remoteness of health care facilities are responsible for high prevalence of lung fluke infections in the endemic areas of Arunachal Pradesh.
Control initiatives from other countries where paragonimiasis is endemic, have revealed that lung fluke infection can be controlled effectively by active detection and treatment of cases and imparting education in a culturally sensitive manner by encouraging good sanitary practices, discouraging risky food habits like consumption of raw or partially cooked crabs or crayfishes17. In countries like China, Korea and Japan paragonimiasis control initiatives have considerably reduced the prevalence of the lung fluke infections1. In South Korea more than one million people were infected in 1950s181920. However, sustained control efforts have dramatically reduced the prevalence of paragonimiasis which ranged earlier from 7.4 to 52.8 per cent1 in different regions to almost negligible levels. In China where paragonimiasis is highly endemic, the surveillance and control measures are actively carried out to reduce prevalence of this disease21222324. Japan has a national programme for controlling paragonimiasis which has resulted in a significant decrease in prevalence of paragonimiasis1. Similarly, paragonimiasis control initiatives have been undertaken in other endemic Western Pacific countries21.
In 2012, the WHO provided a roadmap for combating neglected tropical diseases including paragonimiasis25. It was suggested that by 2015 preventive chemotherapy and morbidity control should also be considered for combatting paragonimiasis and other food-borne trematode (FBT) infections wherever feasible. It was also suggested that by 2020, 75 per cent of population at the risk of FBT should be reached by chemotherapy. However, usefulness of preventive chemotherapy for control of paragonimiasis is yet to be evaluated126. Studies conducted earlier613, including the present study have shown that TB and paragonimiasis are overlapping public health issues in NE region. At present, there is no national level intervention programme targeted towards control of paragonimiasis in India. Integration of paragonimiasis control with the national TB control programme will be an important step towards paragonimiasis elimination in the NE region.
In conclusion, our results showed that active case detection and treatment of infected cases together with community education and awareness programme could be a method to achieve control of paragonimiasis in the endemic areas of NE region of India.
Acknowledgment
Authors acknowledge the Indian Council of Medical Research, New Delhi, for providing financial support.
References
- Trematode infections: liver and lung flukes. Infect Dis Clin North Am. 2012;26:399-419.
- [Google Scholar]
- Global burden of human food-borne trematodiasis: a systematic review and meta-analysis. Lancet Infect Dis. 2012;12:210-21.
- [Google Scholar]
- Paragonimus and paragonimiasis - a new focus in Arunachal Pradesh, India. Curr Sci. 2003;84:985-7.
- [Google Scholar]
- Active detection of tuberculosis and paragonimiasis in the remote areas in North-Eastern India using cough as a simple indicator. Pathog Glob Health. 2013;107:153-6.
- [Google Scholar]
- Pleuropulmonary paragonimiasis due to Paragonimus heterotremus: molecular diagnosis, prevalence of infection and clinicoradiological features in an endemic area of northeastern India. Trans R Soc Trop Med Hyg. 2007;101:786-92.
- [Google Scholar]
- Pulmonary paragonimiasis in childhood--a cause of recurrent haemoptysis and pneumonia. Indian J Chest Dis Allied Sci. 1989;31:211-5.
- [Google Scholar]
- Occurrence of the lung fluke Paragonimus hueit’ungensis in Manipur, India. Zhonghua Yi Xue Za Zhi (Taipei). 2002;65:426-9.
- [Google Scholar]
- Paragonimiasis: an emerging public health problem in India. Indian J Med Res. 2005;121:716-8.
- [Google Scholar]
- Pulmonary paragonimiasis and smear-negative pulmonary tuberculosis: a diagnostic dilemma. Int J Tuberc Lung Dis. 2004;8:621-2.
- [Google Scholar]
- Pleuropulmonary paragonimiasis mimicking pulmonary tuberculosis - a report of three cases. Indian J Med Microbiol. 2005;23:131-4.
- [Google Scholar]
- Development of enzyme-linked immunosorbent assay for serodiagnosis of human paragonimiasis. Indian J Med Res. 2005;121:739-46.
- [Google Scholar]
- Paragonimiasis: diagnosis and the use of praziquantel in treatment. Rev Infect Dis. 1985;7:200-6.
- [Google Scholar]
- Food-borne trematodiases in Southeast Asia epidemiology, pathology, clinical manifestation and control. Adv Parasitol. 2010;72:305-50.
- [Google Scholar]
- Clonorchiasis and paragonimiasis in the Republic of Korea. Report on a prevalence survey using intradermal tests. Bull World Health Organ. 1959;21:721-6.
- [Google Scholar]
- Cerebral and spinal paragonimiasis. A histopathological study. J Neurol Sci. 1969;9:205-36.
- [Google Scholar]
- Large-scale preventive chemotherapy for the control of helminth infection in Western Pacific countries: six years later. PLoS Negl Trop Dis. 2008;2:e278.
- [Google Scholar]
- Paragonimiasis in Yongjia County, Zhejiang Province, China: clinical, parasitological and karyotypic studies on Paragonimus westermani. Southeast Asian J Trop Med Public Health. 2001;32:760-9.
- [Google Scholar]
- Survey on paragonimiasis control in the Lanting People's Commune of Shaoxing County, Zhejiang Province, China. Zhonghua Yu Fang Yi Xue Za Zhi. 1982;16:213-5.
- [Google Scholar]
- Recent progress in studies of Paragonimus and paragonimiasis control in China. Chin Med J (Engl). 1981;94:483-94.
- [Google Scholar]
- World Health Organization (WHO). Accelerating work to overcome the global impact of neglected tropical diseases-a roadmap for implimentation. In: WHO/HTM/NTD 2012. Geneva: WHO; 2012. p. :1.
- [Google Scholar]
- World Health Organization (WHO). Report of the WHO expert consultation on foodborne trematode infections and taeniasis/cysticercosis, Vientiane, Lao People's Democratic Republic, 12-16 October 2009. In: WHO/HTM/NTD/PCT/2011. Geneva: WHO; 2011. p. :3.
- [Google Scholar]




