
Translate this page into:
COVID-19 pandemic from an ophthalmology point of view
For correspondence: Dr Jagat Ram, Department of Ophthalmology, Postgraduate Institute of Medical Education & Research, Chandigarh 160 012, India e-mail: drjagatram@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Coronavirus disease 2019 (COVID-19) is caused by a highly contagious RNA virus termed as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Ophthalmologists are at high-risk due to their proximity and short working distance at the time of slit-lamp examination. Eye care professionals can be caught unaware because conjunctivitis may be one of the first signs of COVID-19 at presentation, even precluding the emergence of additional symptoms such as dry cough and anosmia. Breath and eye shields as well as N95 masks, should be worn while examining patients with fever, breathlessness, or any history of international travel or travel from any hotspot besides maintaining hand hygiene. All elective surgeries need to be deferred. Adults or children with sudden-onset painful or painless visual loss, or sudden-onset squint, or sudden-onset floaters or severe lid oedema need a referral for urgent care. Patients should be told to discontinue contact lens wear if they have any symptoms of COVID-19. Cornea retrieval should be avoided in confirmed cases and suspects, and long-term preservation medium for storage of corneas should be encouraged. Retinal screening is unnecessary for coronavirus patients taking chloroquine or hydroxychloroquine as the probability of toxic damage to the retina is less due to short-duration of drug therapy. Tele-ophthalmology and artificial intelligence should be preferred for increasing doctor-patient interaction.
Keywords
Chloroquine
contact lens
coronavirus
eye donation
eye shields
hydroxychloroquine
ophthalmologist

Introduction
On December 31, 2019, the Government of China sounded the World Health Organization of a group of patients being admitted to hospitals with atypical pneumonia with likely origin due to a virus from the Huanan seafood marketplace in Wuhan city, situated in the province of Hubei in China1. Initially, the virus was thought to have an animal-to-human transmission, but the enormous spread among humans due to the massive human migration on account of the Chinese New Year proved this fact untrue with the evidence of human-to-human transmission234. Coronavirus disease 2019 (COVID-19) is a new infection that can affect both the upper and lower respiratory tracts through aerosols, faeces and contaminated surfaces5678. However, no transmission through breast milk has been documented9. A potentially fatal form of it is known as severe acute respiratory syndrome (SARS)10. It is produced by a highly contagious RNA virus termed as SARS coronavirus 2 (SARS-CoV-2), with the tremendous capability of survival attributed to its rapid mutation rates as compared to DNA viruses11. As of May 20, 2020, SARS-CoV-2 had affected 5,054,252 people in 213 countries/territories and two international conveyances, with 327,938 mortalities located majorly within the USA, Russia, Spain, Brazil, the UK and Italy12. India had 112,028 people affected with 3,434 total deaths, with the maximum being in the State of Maharashtra13. This review highlights the risk ophthalmologists have due to close proximity with patients and suggests ways to prevent this transmission.
Medical personnel at high-risk
Ophthalmologists are at a high-risk due to the following three important reasons: presence of virus in the tear fluid, proximity of encounter and deceiving symptoms.
Presence of virus in the tear fluid
SARS-CoV-2 via its surface spike glycoprotein binds to the angiotensin-converting enzyme 2 (ACE2) receptors. These ACE2 receptors are found distributed in various human organs, including the surface of the cornea and the conjunctiva, and these act as potential entry points1415. Coronavirus was spotted in the conjunctival discharge of COVID-19-positive patients having conjunctivitis16. Loon et al17 have isolated virus from the tears of coronavirus-infected patients by reverse transcription-polymerase chain reaction (RT-PCR). While examining the patient, the risk of tears contaminating the fingers of the examiner as well as the instruments, is fairly high18.
Proximity of encounter
Because of the proximity (20-30 cm) to the patients, examining a patient in the clinic (conjunctival discharge, tears and nasal/oral secretions) can pose a hazard to ophthalmologists192021. The patients visiting ophthalmology clinics are predominantly elderly and they suffer from old age-related diseases such as cataracts, macular degenerations and glaucoma22. Hence, nosocomial infections are an essential concern both for the doctor and the patient23.
Deceiving symptoms
Eye care professionals can also be caught unaware because conjunctivitis may be one of the first signs of COVID-19 at presentation, even precluding the emergence of additional symptoms such as dry cough and anosmia24. The American Academy of Ophthalmology (AAO) has released an advisory alerting eye specialists to put on face and eye shields while examining patients with fever, breathlessness or any history of international travel or travel to and from any hotspot25. With these reasons in the background, it is especially important to have practical and useful guidelines, directed at eye care specialists, tailored to the local needs to curtail the incidence of coronavirus infection in both medical personnel and patients.
Guidelines for ophthalmologists to prevent the spread of COVID-19
Ocular involvement in patients with proven SARS-CoV-2 infection
The symptoms of COVID-19 may vary from being completely asymptomatic to having fever, cough, breathlessness, muscle aches, fatigue and loss of smell or taste26. Non-specific symptoms include headache, blood in vomitus or diarrhoea27. A few COVID-19 patients present with conjunctival redness or conjunctivitis21.
In a series of 38 patients from Hubei province in China, those with ophthalmic symptoms were more susceptible to have leucocytosis with increased neutrophil numbers and much higher enzymes such as procalcitonin, C-reactive protein and lactate dehydrogenase than patients with no ophthalmic manifestations. Ocular features were seen in one-third of the involved patients and they demonstrated signs of conjunctivitis, including conjunctival hyperaemia, chemosis or increased tearing. Fundus was not evaluated in any of these patients. However, none of them complained of any decrease in vision. Nearly 91.7 per cent of the patients of the one-third in this study tested positive for SARS-CoV-2 using RT-PCR from nasopharyngeal swabs and of these, 16.7 per cent tested positive from both conjunctival and nasopharyngeal swabs28.
In another study by Guan et al26, among 1,099 patients from mainland China, 0.8 per cent (9 patients) had symptoms of conjunctival congestion. In a case report of a 30 yr old patient of confirmed COVID-19, bilateral follicular conjunctivitis with tearing, redness and moderate and tender preauricular lymphadenopathy was documented on the day 14 of illness with the subsequent resolution on day 19. The fundus picture taken through a non-mydriatic fundus camera as well as macular optical coherence tomography was unremarkable. The virus load in the swabs obtained from the conjunctiva was considerably lesser than that obtained from the nasopharyngeal swabs29.
Ocular symptoms/signs as first indicators of SARS-CoV-2 infection
In a prospective contact tracing study in China, the first symptom of a 22 yr old index patient of COVID-19 was itchy eyes30. In another study which included 534 COVID-19-confirmed patients, 25 patients (4.68%) had conjunctival congestion and of them, three patients had it as the first symptom. The mean duration of the congestion was 4.9±2.6 days. Dry eye (112, 20.97%), blurred vision (68, 12.73%) and foreign body sensation (63, 11.80%) were the most frequently occurring ophthalmic symptoms in these patients. Other symptoms included itching and photophobia. Approximately more than 60 per cent of patients had a history of hand-eye touch31. Other studies also demonstrated conjunctival congestion in 4.76 per cent and 2.78 per cent of the total COVID-19 patients, respectively3233. In a contrary study of 17 patients, tear samples were negative for SARS-CoV-2, even though nasopharyngeal swabs were positive. One of the 17 patients demonstrated eye signs even though SARS-CoV-2 could not be established in tears. This study concluded that viral spread through tears irrespective of the stage of infection is less34.
Other coronaviruses are responsible for causing a wide spectrum of ophthalmic signs and symptoms such as conjunctivitis, uveitis and posterior segment vision-impairing conditions such as retinitis and optic neuritis. However, uveitis and other posterior segment manifestations have not been documented35. An illustrated depiction of all eye-related symptoms is given in Figure 1.
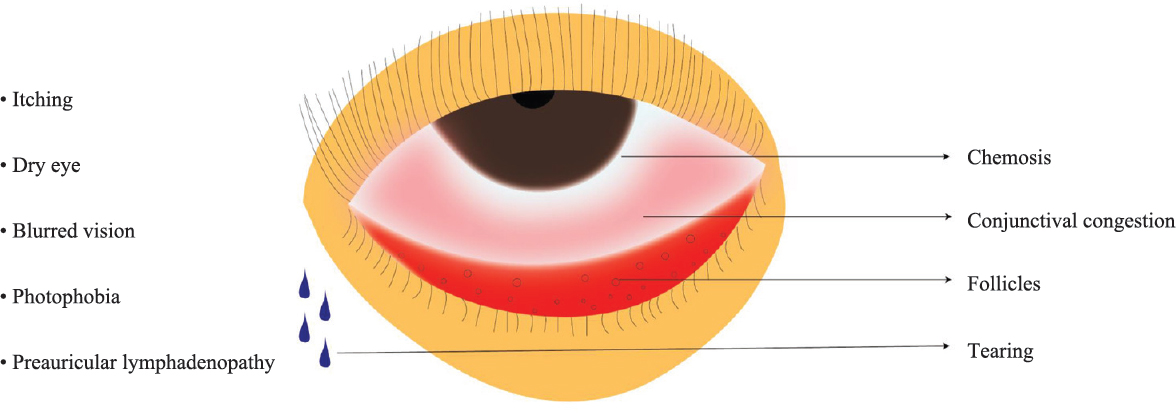
- Ophthalmological signs and symptoms of coronavirus disease 2019. Chemosis, conjunctival congestion, follicles, tearing, itching, dry eye, blurred vision, photophobia and preauricular lymphadenopathy are major signs.
Guidelines at the place of practice
Non-pharmacological interventions, hygiene practices and personal protective equipment (PPE) to limit the virus circulation along with postponement of non-emergency surgeries should be followed in both public and private ophthalmology clinics21. Some of the important points are discussed below:
Opting for tele-ophthalmology: Only e-mails, phone calls, messages and social media platforms should be used to communicate with the patients. Tele-ophthalmology services can be used for patient consults or for patients requiring urgent follow up3637. The governments in different countries have recommended telemedicine in lieu of in-hospital visits. Lives can be saved by social distancing in pandemic areas38. Mode of communication can be audio, video or text.
There are mobile apps for visual acuity and perimetry3940. Home monitoring of intraocular pressure using finger tension and of metamorphopsia using Amsler grid should be done41. Drug dosage modifications can be done during teleconsultation. Informed consent of the patient needs to be taken during tele-consults or video visits. Doctor-patient interaction can also be enhanced through the Internet with the assistance of artificial intelligence4243.
Screening at entrance to hospital: For any patient visiting the eye hospital, at the entry point, a history of travel in the past 14 days from an area in the red zone should be enquired about44. Thermal scanning should be done at the main entrance. The patient and the attendants should be asked to wear a three-ply mask. If the patient has fever or any of the aforementioned symptoms, he/she should be taken to the dedicated COVID-19 hospital454647.
Triaging: Triaging: Initially, telephonic triaging can be practised, and only those patients who require emergent ophthalmic check-up should be called to the hospital. Triaging should be able to segregate the patients into the following three groups: (i) patients who can be seen in the main stream (patients without symptoms and a history of travel to hotspots); (ii) patients who have to be sent to COVID-19 managing hospital; and (iii) indeterminate group. The indeterminate group should be evaluated for the need for urgent eye consultation. If urgent, they would need to be examined in a separate isolation room with PPE.
Emergent conditions: Patients with sudden-onset of painful or painless vision loss, or sudden-onset squint, or sudden-onset floaters or severe lid oedema and children with the aforementioned conditions as well as those with unilateral white reflex should be attended to on an emergent basis21. For patients presenting with conjunctivitis, allergic or toxic conjunctivitis should be ruled out. Circumcorneal congestion can point towards serious ocular conditions such as uveitis or corneal ulcers. The final treatment can be targeted towards the most common causes of conjunctivitis i.e., viral/bacterial, which consists of a topical fluoroquinolone and lubricants. Topical steroids should be avoided as it would require frequent follow up for intraocular pressure monitoring48. The latest guidelines by the All India Ophthalmological Society have given subspecialty-wise classification of procedure on the basis of priority: emergency, urgent and routine procedures46.
Management at outpatient department (OPD): Children <10 yr and elderly >65 yr should be discouraged from visiting the hospital unless they are patients themselves. The waiting areas should be decongested and intercoms or call notifications on phones can be used to call each patient for examination49.
Special referral tests such as refraction perimetry, optical coherence tomography, fundus fluorescein angiography, corneal topography, specular microscopy, ultrasound and ultrasound biomicroscopy should be deferred until these are critical for making a diagnosis. Fundus evaluation, if required, can be done using non-mydriatic fundus cameras. Indirect ophthalmoscopy should be preferred in place of the slit lamp for examination as it has a larger working distance. Indirect ophthalmoscopy can also be used for evaluating the central fundus in case of non-availability of non-mydriatic fundus cameras.
Management at operation theatre (OT) level: All elective surgeries should be postponed. Surgeries under general anaesthesia should be avoided as extubation leads to aerosol generation. Since nasal secretions have been shown to contain SARS-CoV-2; procedures which act as nasal simulants such as nasal endoscopy should be avoided34. Topical anaesthesia should be preferred over regional anaesthesia. Pre-operative testing for COVID-19 should be done for all patients46. Full PPE (N95 mask, fog and scratch-resistant goggles/face-shield, disposable waterproof gown, preferably nitrile gloves, and impermeable shoe covers) should be worn by surgeons while operating on COVID-19-confirmed patients. Proper technique of donning and doffing of PPE and their disposal should be followed50. Separate colour-coded bins/bags should be kept as per the Biomedical Waste Rules 2016 and amended by the Central Pollution Control Board51.
Instrument sanitation should be done after seeing every patient. Sanitation of the floor, doorknobs and bed rails should be done using freshly prepared one per cent sodium hypochlorite preferably after every two hours46. The air conditioning should have fresh air exchange and should be fitted with standard filters. Temperature and humidity should be maintained as per guidelines. Negative pressure is preferred in rooms requiring aerosolization procedures such as intubation/extubation, suction and nebulization52. A summary of potential strategies in hygiene practices, personal protective equipment and non-pharmacological interventions is documented in Figure 2.
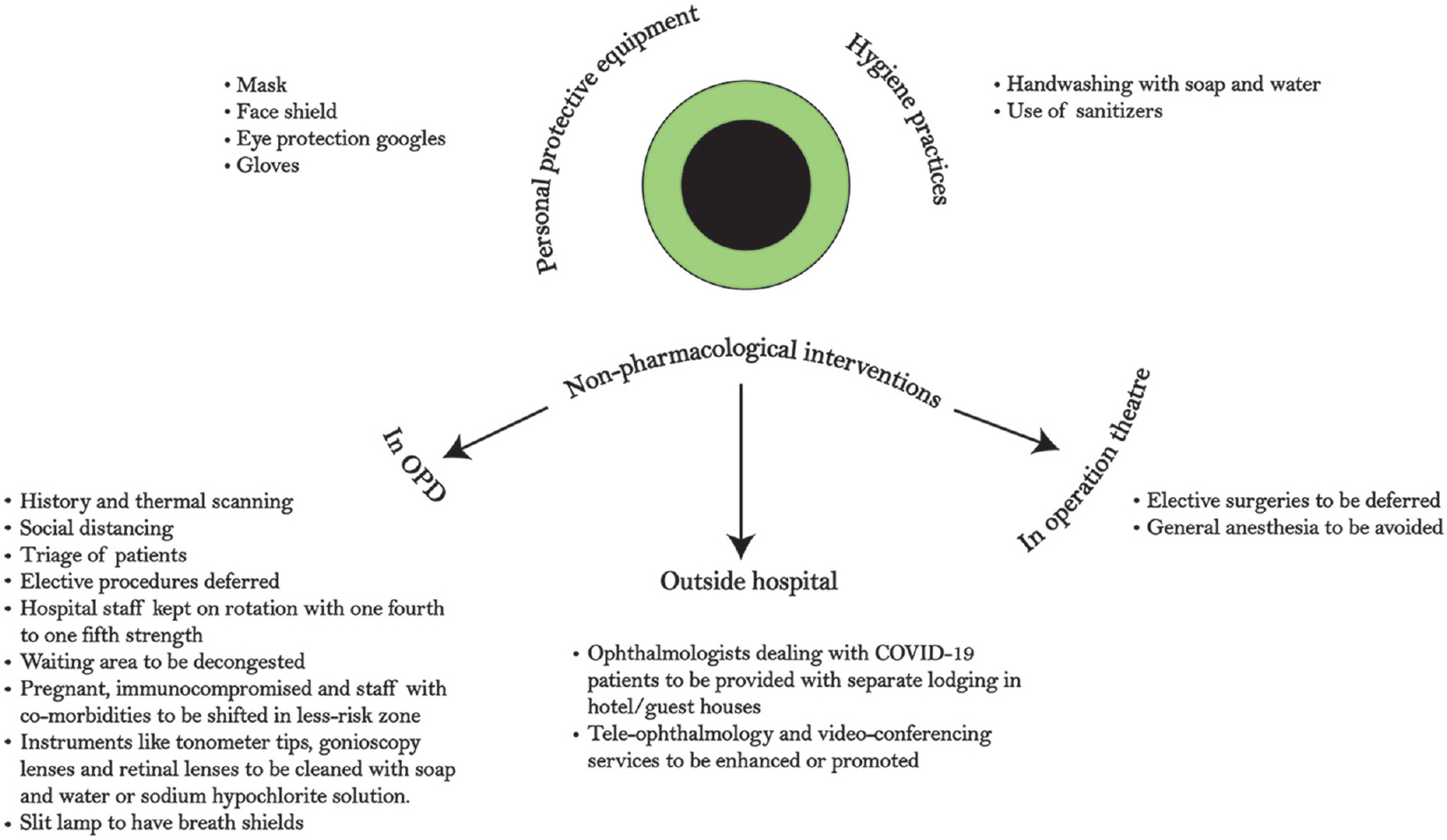
- A summary of potential strategies in hygiene practices, personal protective equipment and non-pharmacological interventions for the prevention of infection among the ophthalmologists and patients visiting ophthalmology clinics.
Special topics of interest in COVID-19 era
Contact lens (CL) practice
A contact lens specialist should keep away from touching his/her face and mucus membrane-covered areas such as nose, mouth and eyes53. CLs should be adequately cleaned, and disposable CLs should not be used longer than what is recommended. Individuals should be told to discontinue CL wear if they have any symptoms of COVID-195455.
Corneal donation guidelines
The Eye Bank Association of America (EBAA): The Eye Bank Association of America has laid down guidelines for eye donation56. According to these, eye banks should avoid corneal donation from donors who in the last 28 days were positive for the novel coronavirus or those who came in contact with a positive case or a suspect or those who had an acute respiratory illness with fever >38°C with any one of the symptoms of COVID-19 or those who had acute respiratory distress syndrome/pneumonia/ground-glass opacities on computed tomography. Cornea from a donor who has tested negative for the disease and has been diagnosed with another aetiology which explains the symptoms or findings can be considered for transplant57.
Global Alliance of Eye Bank Associations (GAEBA): Because there is no evidence till date that coronaviruses can be transmitted by avascular tissue (cornea) transplantation even though it has been proved to be present in tears and conjunctival discharges of patients positive for the novel coronavirus, any efforts to procure tissue are precautionary, hence, the guidelines include that any potential donor with confirmed or suspected coronavirus infection should not donate if the death has occurred less than 14 days since the resolution of symptoms or awaiting test results for suspected coronavirus infection. Moreover, if the donor has been in contact with a confirmed or suspected case of coronavirus infection less than 14 days from the first day of contact, the donation should be avoided57.
Eye Bank Association of India (EBAI): The Eye Bank Association of India57 has given an advisory for the resumption of eye banking activities through the Hospital Cornea Retrieval Programme in the non-containment area of the red zones as demarcated by the government. Because the virus may be present in tears and mucus membranes, it is risky for those healthcare personnel who are deployed for recovery of the donated ocular tissue. They should wear full PPE (cap, gloves, N95 mask, face shield, gown and shoe covers) before enucleating the donor eyeball. Guidelines for cornea and eye banking should be followed58.
Retinal screening before starting chloroquine therapy
Chloroquine (CQ) and hydroxychloroquine (HCQ) have been demonstrated to have considerable efficacy against the SARS-CoV-259. CQ and HCQ have been used by the physicians since long for diseases such as systemic lupus erythematosus (SLE) as well as rheumatic disorders60. Retinal toxicity is rarely seen before 10 or more years of use at a dose of <5 mg/kg real weight as advocated by the AAO guidelines61. Rheumatologists have been routinely using HCQ as a part of the therapeutic regimen for SLE, myeloma and small-cell carcinoma of the lung. These regimens extend from a few weeks to months. Visual loss has not been documented in any of the studies except in two patients who showed subtle alterations in the parafoveal ellipsoid zone on optical coherence tomography626364.
Marmor60 has concluded that ophthalmic retinal screening is unnecessary for coronavirus patients taking CQ or HCQ as antiviral drug therapy for a time period less than two weeks, as the probability of toxic damage to the retina is extremely less even on using large dosages. Other drugs such as remdesivir, CQ, oseltamivir, interferon 1β, tocilizumab and convalescent serum, as well as anti-mRNA vaccines, are under trial47.
Conclusion
SARS-CoV-2 infection has evolved as a global health emergency in the present era. The risk of infection to the healthcare workers is very real, however, all healthcare professionals do not have the same risk. An ophthalmologist treating a presumably non-COVID-19 patient, especially with good triaging and exclusion of most of the potentially COVID-19-positive patients, is not exposed the same level of risk. Hence, ophthalmologists should work in tandem with infectious disease specialists for risk stratification and infection control measures as well as for the use of PPE. Till the time a cure is developed, artificial intelligence-based platforms, as well as tele-ophthalmology, should be encouraged.
Financial support & sponsorship: None.
Conflicts of Interest: None.
References
- Pneumonia of unknown cause - China. Available from: http://wwwwhoint/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en/">http://wwwwhoint/csr/don/05-january-2020-pneumonia-of-unkown-cause-china/en/
- China confirms new coronavirus spreads from humans to humans. Available from: https://wwwnytimescom/2020/01/20/world/asia/coronavirus-china-symptomshtml">https://wwwnytimescom/2020/01/20/world/asia/coronavirus-china-symptomshtml
- Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet. 2020;395:507-13.
- [Google Scholar]
- China will rack up three billion trips during world's biggest human migration. Available from: https://wwwbloombergcom/news/articles/2020-01-20/china-readies-for-world-s-biggest-human-migration-quicktake">https://wwwbloombergcom/news/articles/2020-01-20/china-readies-for-world-s-biggest-human-migration-quicktake
- The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;109:102433.
- [Google Scholar]
- Molecular and serological investigation of 2019-nCoV infected patients: Implication of multiple shedding routes. Emerg Microbes Infect. 2020;9:386-9.
- [Google Scholar]
- The different clinical characteristics of corona virus disease cases between children and their families in China - the character of children with COVID-19. Emerg Microbes Infect. 2020;9:707-13.
- [Google Scholar]
- WHO Director-General's remarks at the media briefing on 2019-nCoV on 11 February 2020. Available from: https://wwwwhoint/dg/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020">https://wwwwhoint/dg/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020
- Uncertainties about the transmission routes of 2019 novel coronavirus Influ Other Respir Viruses 2020 101111/irv12735
- Insights into the recent 2019 novel coronavirus (SARS-CoV-2) in light of past human coronavirus outbreaks. Pathogens. 2020;9:186.
- [Google Scholar]
- Coronavirus Update (Live): 2,250,689 cases and 154,256 deaths from COVID-19 virus pandemic - Worldometer. Available from: https://www.worldometers.info/coronavirus/
- org Coronavirus (COVID-19) updates worldwide & India with state wise status. Available from: https://covidindiaorg/">https://covidindiaorg/
- Receptor recognition by the novel coronavirus from Wuhan: An analysis based on decade-long structural studies of SARS coronavirus. J Virol. 2020;94:e00127-20.
- [Google Scholar]
- Expression of SARS coronavirus S protein functional receptor ACE2 in human and rabbit cornea and conjunctiva. Rec Adv Ophthalmol. 2004;24:332-6.
- [Google Scholar]
- The severe acute respiratory syndrome coronavirus in tears. Br J Ophthalmol. 2004;88:861-3.
- [Google Scholar]
- Revisiting the dangers of the coronavirus in the ophthalmology practice. Eye (Lond) 2020:1-3.
- [Google Scholar]
- Is novel coronavirus disease (COVID-19) transmitted through conjunctiva. J Med Virol 2020 101002/jmv25753
- [Google Scholar]
- Novel coronavirus disease 2019 (COVID-19): The importance of recognising possible early ocular manifestation and using protective eyewear. Br J Ophthalmol. 2020;104:297-8.
- [Google Scholar]
- Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323:1061-9.
- [Google Scholar]
- COVID-19: A novel coronavirus and a novel challenge for critical care. Intensive Care Med. 2020;46:833-6.
- [Google Scholar]
- 2019-nCoV transmission through the ocular surface must not be ignored. Lancet. 2020;395:E39.
- [Google Scholar]
- Important coronavirus updates for ophthalmologists. Available from: https://wwwaaoorg/headline/alert-important-coronavirus-context,">https://wwwaaoorg/headline/alert-important-coronavirus-context
- Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382:1708-20.
- [Google Scholar]
- Characteristics of ocular findings of patients with coronavirus disease 2019 (COVID-19) in Hubei province, China. JAMA Ophthalmol. 2020;138:575-8.
- [Google Scholar]
- Ocular manifestations of a hospitalised patient with confirmed 2019 novel coronavirus disease. Br J Ophthalmol. 2020;104:748-51.
- [Google Scholar]
- Rapid asymptomatic transmission of COVID-19 during the incubation period demonstrating strong infectivity in a cluster of youngsters aged 16-23 years outside Wuhan and characteristics of young patients with COVID-19: A prospective contact-tracing study. J Infect. 2020;80:e1-13.
- [Google Scholar]
- Ocular manifestations and clinical characteristics of 534 cases of COVID-19 in China: A cross-sectional study. medRxiv 2020 doi: 101101/2020031220034678
- [Google Scholar]
- Ophthalmologic evidence against the interpersonal transmission of 2019 novel coronavirus through conjunctiva medRxiv 2020 doi: 101101/2020021120021956
- The infection evidence of SARS-COV-2 in ocular surface: A single-center cross-sectional study. medRxiv 2020 doi: 101101/2020022620027938
- [Google Scholar]
- Assessing viral shedding and infectivity of tears in coronavirus disease 2019 (COVID-19) patients. Ophthalmology 2020 pii: S0161-6420(20)30311-0
- [Google Scholar]
- Can the coronavirus disease 2019 (COVID-19) affect the eyes? A review of coronaviruses and ocular implications in humans and animals. Ocul Immunol Inflamm. 2020;28:391-5.
- [Google Scholar]
- Telemedicine practice guidelines; March 25, 2020. Available from: https://wwwmohfwgovin/pdf/Telemedicinepdf">https://wwwmohfwgovin/pdf/Telemedicinepdf
- AIOS telemedicine practice guidelines. Available from: https://aiosorg/pdf/AIOS-Telemedicine-Practice-Guidelinespdf">https://aiosorg/pdf/AIOS-Telemedicine-Practice-Guidelinespdf
- 2020. Clinical care guidance for healthcare professionals about coronavirus (COVID-19). Atlanta: CDC; Available from: https://wwwcdcgov/coronavirus/2019-ncov/hcp/clinical-carehtml">https://wwwcdcgov/coronavirus/2019-ncov/hcp/clinical-carehtml
- Virtual ophthalmology: Telemedicine in a Covid-19. Era Am J Ophthalmol 2020 pii: S0002-9394(20)30214-2
- [Google Scholar]
- Comparison of Peristat online perimetry with the Humphrey perimetry in a clinic-based setting. Transl Vis Sci Technol. 2016;5:4.
- [Google Scholar]
- Detecting possible glaucoma with only limited equipment: A crucial first step. Community Eye Health. 2012;25:48-9.
- [Google Scholar]
- Promising artificial intelligence-machine learning-deep learning algorithms in ophthalmology. Asia Pac J Ophthalmol (Phila). 2019;8:264-72.
- [Google Scholar]
- Artificial intelligence in ophthalmology: Accuracy, challenges, and clinical application. Asia Pac J Ophthalmol (Phila). 2019;8:197-9.
- [Google Scholar]
- 2020. Coronavirus disease 2019 (COVID-19). Atlanta: CDC; Available from: https://wwwcdcgov/coronavirus/2019-ncov/indexhtml">https://wwwcdcgov/coronavirus/2019-ncov/indexhtml
- Guidelines for the use of non-pharmaceutical measures to delay and mitigate the impact of 2019-nCoV. Available from: https://wwwecdceuropaeu/en/publications-data/guidelines-use-non-pharmaceutical-measures-delay-and-mitigate-impact-2019-ncov">https://wwwecdceuropaeu/en/publications-data/guidelines-use-non-pharmaceutical-measures-delay-and-mitigate-impact-2019-ncov
- All India Ophthalmological Society - Indian Journal of Ophthalmology consensus statement on preferred practices during the COVID-19 pandemic. Indian J Ophthalmol. 2020;68:711-24.
- [Google Scholar]
- All eyes on Coronavirus-What do we need to know as ophthalmologists. Indian J Ophthalmol. 2020;68:549-53.
- [Google Scholar]
- What ophthalmologists should know about conjunctivitis in the COVID-19 pandemic? Indian J Ophthalmol. 2020;68:683-7.
- [Google Scholar]
- Preparedness among ophthalmologists: During and beyond the COVID-19 pandemic. Ophthalmology. 2020;127:569-72.
- [Google Scholar]
- Novel coronavirus disease 2019 (COVID-19): Guidelines on rational use of personal protective equipment. Available from: https://wwwmohfwgovin/pdf/Guidelinesonrationaluseof PersonalProtectiveEquipmentpdf">https://wwwmohfwgovin/pdf/Guidelinesonrationaluseof PersonalProtectiveEquipmentpdf
- 2020. Guidelines for handling, treatment, disposal of waste generated during treatment/ diagnosis/ quarantine of COVID-19 patients. New Delhi: Ministry of Environment, Forest & Climate Change, Government of India; Available from: https://wwwmohfwgovin/pdf/63948609501585568987wastesguidelinespdf">https://wwwmohfwgovin/pdf/63948609501585568987wastesguidelinespdf
- ISHRAE COVID-19 guidance document for air conditioning and ventilation. New Delhi: ISHRAE; 2020.
- Infection control guidelines for optometrists 2016. Clin Exp Optom. 2017;100:341-56.
- [Google Scholar]
- Contact lens practice in the time of COVID-19. Cont Lens Anterior Eye. 2020;43:193-5.
- [Google Scholar]
- Stepping up infection control measures in ophthalmology during the novel coronavirus outbreak: An experience from Hong Kong. Graefes Arch Clin Exp Ophthalmol. 2020;258:1049-55.
- [Google Scholar]
- COVID-19 updates. Available from: https://restoresightorg/covid-19-updates/">https://restoresightorg/covid-19-updates/
- ALERT UP-DATE: Coronavirus (COVID-2019) and ocular tissue donation. Available from: http://wwwgaebaorg/2020/alert-coronavirus-2019-ncov-and-ocular-tissue-donation/">http://wwwgaebaorg/2020/alert-coronavirus-2019-ncov-and-ocular-tissue-donation/
- New insights on the antiviral effects of chloroquine against coronavirus: What to expect for COVID-19? Int J Antimicrob Agents. 2020;55:105938.
- [Google Scholar]
- COVID-19 and chloroquine/hydroxychloroquine: Is there ophthalmological concern? Am J Ophthalmol. 2020;213:A3-4.
- [Google Scholar]
- Recommendations on screening for chloroquine and hydroxychloroquine retinopathy (2016 Revision) Ophthalmology. 2016;123:1386-94.
- [Google Scholar]
- Dose-loading with hydroxychloroquine improves the rate of response in early, active rheumatoid arthritis: A randomized, double-blind six-week trial with eighteen-week extension. Arthritis Rheum. 1999;42:357-65.
- [Google Scholar]
- Combined autophagy and proteasome inhibition: A phase 1 trial of hydroxychloroquine and bortezomib in patients with relapsed/refractory myeloma. Autophagy. 2014;10:1380-90.
- [Google Scholar]
- Rapid onset of retinal toxicity from high-dose hydroxychloroquine given for cancer therapy. Am J Ophthalmol. 2015;160:799-805.
- [Google Scholar]




