
Translate this page into:
Computed tomography chest in COVID-19: When & why?
For correspondence: Dr Mandeep Garg, Department of Radiodiagnosis & Imaging, Postgraduate Institute of Medical Education & Research, Chandigarh 160 012, India e-mail: gargmandeep@hotmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Computed tomography (CT) of the chest plays an important role in the diagnosis and management of coronavirus disease 2019 (COVID-19), but it should not be used indiscriminately. This review provides indications of CT chest in COVID-19 suspect, positive and recovered patients based on the current scientific evidence and our personal experience. CT chest is not indicated as a routine screening modality due to its poor sensitivity and specificity. However, it is useful in a small subset of COVID-19 suspects who test negative on reverse transcription-polymerase chain reaction (RT-PCR) with normal/indeterminate chest X-ray (CXR) but have moderate-to-severe respiratory symptoms and high index of clinical suspicion. CT chest is not indicated in every RT-PCR–positive patient and should be done only in specific clinical scenarios, where it is expected to significantly contribute in the clinical management such as COVID-19 patients showing unexplained clinical deterioration and/or where other concurrent lung pathology or pulmonary thromboembolism needs exclusion. Serial CXR and point-of-care ultrasound are usually sufficient to evaluate the progression of COVID-19 pneumonia. CT chest is also indicated in COVID-19–positive patients with associated co-morbidities (age >65 yr, diabetes, hypertension, obesity, cardiovascular disease, chronic respiratory disease, immune-compromise, etc.) who, despite having mild symptoms and normal/indeterminate CXR, record oxygen saturation of <93 per cent at rest while breathing room air or de-saturate on six-minute walk test. Finally, CT chest plays a crucial role to rule out lung fibrosis in patients recovered from COVID-19 infection who present with hypoxia/impaired lung function on follow up. In conclusion, though CT chest is an indispensable diagnostic tool in COVID-19, it should be used judiciously and only when specifically indicated.
Keywords
Chest
comorbidities
COVID-19
computed tomography scan
RT-PCR
thromboembolism

Introduction
Coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that primarily affects the lungs, and computed tomography (CT) of the chest plays an important role in the evaluation of COVID-19. There have been more than 78 million cases of COVID-19 reported worldwide and >10 million cases of COVID-19 reported in India as on December 24, 20201. Since there is no definite treatment available for COVID-19, the effective control relies on early diagnosis and isolation/quarantine of the infected patients. However, the current reference standard test for confirming the diagnosis of SARS-CoV-2, i.e. reverse transcription-polymerase chain reaction (RT-PCR) on the nasal and pharyngeal swabs, only has a sensitivity of 32-80 per cent23456. Furthermore, the newer rapid antigen and antibody tests have much lower sensitivity as compared to RT-PCR. The inability of these tests to definitively diagnose all cases of COVID-19 has potentially important ramifications pertaining to the spread of infection and clinical management. In absence of a reliable single diagnostic test for COVID-19, the role of chest CT becomes pivotal in the diagnosis, evaluation and management of COVID-19. However, there is conflicting evidence regarding the use of CT chest in COVID-192378910. Despite the consensus statements and guidelines issued by the WHO11, the Fleischner Society9 and various other international radiology associations and chest societies8, appropriate usefulness of chest CT in COVID-19 remains unclear. In addition, the multitude of different clinical scenarios associated with COVID-19 can result in partial or non-compliance with the suggested imaging recommendations. The COVID-19 pandemic mandates practical utilization guidelines for chest CT that are understandable and applicable internationally at all levels of clinical care. The current article addresses this issue and succinctly defines the indications for CT chest in COVID-19, based on the current scientific evidence and our personal experience with COVID-19 in the three tertiary care medical institutes of India having fully dedicated COVID-19 hospital wings.
COVID-19: Routine screening and suspects
The use of chest CT as a routine screening modality in COVID-19 has many limitations and is not recommended. In this regard, 15-50 per cent of patients with COVID-19 will have a normal chest CT, particularly early in the course of the disease512. Consequently, similar to a false-negative RT-PCR, a normal CT chest in patients with COVID-19 could potentially result in inappropriate isolation/quarantine recommendations. Moreover, chest CT abnormalities are not diagnostic of COVID-19 and can be indistinguishable from the manifestations of other viral pneumonia, including influenza, H1N1, adenovirus and rhinovirus101314. An additional limitation is the risk of infection from surface contamination and/or aerosolization, during the process of CT acquisition of a COVID-19 patient. Although sanitization and decontamination of the CT imaging facility and appropriate air exchange can reduce the risk of infection15, it is a time-consuming task and is required to be done after the acquisition of each suspect case. The healthcare workers engaged in CT suite are at an increased risk for catching this infection and should wear appropriate personal protective equipment as per the standard recommendations and guidelines of their local infection control committee. Conversely, CT imaging facility can also act as a source of COVID-19 infection to the other patients coming for CT examination. Because of these limitations of CT imaging, all international radiology organizations and chest societies have unanimously recommended that chest CT should not be used for routine screening in COVID-198916.
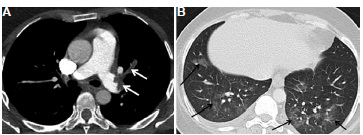
Chest CT may be useful in a few COVID-19 suspects who test negative on RT-PCR with normal/indeterminate chest X-ray (CXR), despite having moderate-to-severe respiratory symptoms9 and a high index of suspicion for COVID-19. In this scenario, a typical CT pattern of COVID-19 with COVID-19 Reporting and Data System (CO-RADS)17 Category 4/5 allows presumptive diagnosis of COVID-19 pneumonia, warranting immediate isolation of such patients. As COVID-19 patients are known to show sudden clinical deterioration, close monitoring of such patients is necessary until the confirmatory diagnosis is established. Various studies have shown that a few patients who initially tested RT-PCR negative on one or more occasions despite having strong clinical suspicion of COVID-19 subsequently were found to be COVID-19 positive on repeat RT-PCR tests231819. CT chest in these patients has shown the classical imaging findings of COVID-19 infection (CO-RADS 4/5) which includes ground-glass opacities, consolidation, septal/bronchovascular bundle thickening, crazy-paving and halo/reversed halo sign (Fig. 1), while lymphadenopathy, centrilobular nodules and pleural effusion, though uncommon, have also been seen in a few patients14.
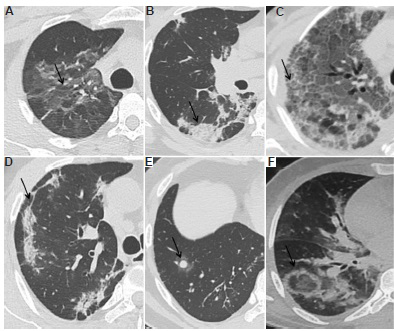
- Common computed tomography (CT) manifestations (indicated by arrows) of COVID-19 pneumonia in different patients: (A) ground-glass opacities, (B) consolidation, (C) crazy-paving, (D) sub-pleural linear opacities and parenchymal bands, (E) halo sign, (F) reverse halo sign.
In concordance with these studies, the role of CT chest is emphasized in those RT-PCR–negative patients who show significant (moderate-to-severe) respiratory symptoms and carry a high index of suspicion for COVID-19 (Fig. 2). To enhance the diagnostic accuracy of chest CT in such patients, CT interpretation should be done in conjunction with blood indices that are more likely to be found altered in COVID-19 pneumonia, viz. lymphopenia, elevated neutrophil-lymphocyte ratio (NLR), serum D-dimer, lactate dehydrogenase (LDH) and inflammatory markers such as C-reactive protein (CRP), interleukin-6, serum-ferritin and fibrinogen520.
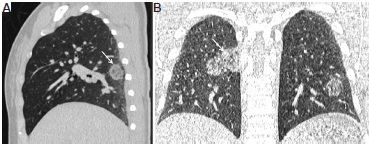
- CT chest of a 45 yr old female who presented with fever and moderate dyspnoea and history of contact with COVID-19 pneumonia patient. Two RT-PCR tests for COVID-19 virus done from oropharyngeal swab samples days on 5 and 7 of symptoms were negative. CT chest was done on the eighth day. (A and B) Sagittal and coronal CT sections in the lung window showed areas of ground-glass opacities (arrow) in the right upper and middle lobes and left lower lobe. Computed tomography was reported COVID-19 Reporting and Data System Category 5 (CO-RADS 5); the patient was isolated and managed as COVID-19 pneumonia. Repeat RT-PCR test was positive for COVID-19 on the ninth day.
RT-PCR–positive COVID-19 patients
Chest CT is clinically useful in RT-PCR–positive patients, but it is not indicated in every positive patient and should be done only in specific clinical situations where it is expected to influence the treatment plan and further management of the patient. CT chest is needed in patients where clinical examination or radiographic findings are suspicious of other concurrent lung pathology (infectious, inflammatory or neoplastic), which may warrant a change in the treatment plan. For example, in tuberculosis (TB)-endemic countries like India, before starting the corticosteroids or immune modulators such as tocilizumab, it is important to be vigilant about the possibility of concurrent/latent pulmonary TB. CT chest in such situations plays a vital role in guiding the treatment plan (Fig. 3). However, it is always desirable to have the tissue/microbial diagnosis of concurrent lung pathology as CT scan alone in many instances may not be able to give the exact diagnosis.
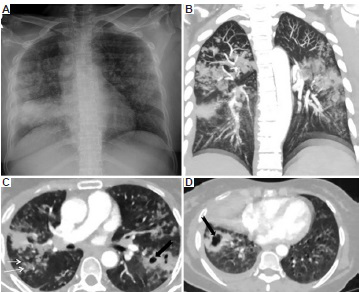
- A 60 yr old female, COVID-19 RT-PCR positive, was planned to start on tocilizumab in view of her rising inflammatory markers and worsening hypoxia. (A) Chest X-ray revealed nodular opacities in both upper and mid zones with dense consolidation in the right lower zone; findings were indeterminate for coronavirus disease pneumonia. (B-D) CT chest showed multiple random and centrilobular nodules (white arrows) and cavitating lesions (black arrows). These features were consistent with pulmonary tuberculosis (confirmed with sputum GeneXpert), so tocilizumab was withheld.
Further, CT chest is particularly useful in those COVID-19 patients who show a sudden and unexplained clinical deterioration or are unresponsive to treatment (Fig. 4). Some of the patients of COVID-19 may also require CT pulmonary angiography in the appropriate clinical setting (Fig. 5) as SARS-CoV-2 can result in the formation of microthrombi in blood vessels and there is an increased prevalence of pulmonary thromboembolism in patients of COVID-192122.
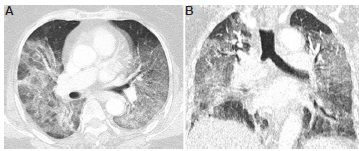
- CT chest of a 70 yr old woman, RT-PCR positive for COVID-19, who presented with unexplained clinical deterioration. (A and B) Lung window (axial and coronal sections) showing bilateral, diffuse areas of ground-glass opacities and patchy consolidation, which demonstrate anteroposterior gradient and predominance in dependent regions of the lungs. CT and clinical features were consistent with acute respiratory distress syndrome. The patient expired the next day.
- A 40 yr old male patient with COVID-19 pneumonia developed sudden onset of breathlessness. CT pulmonary angiography was done. (A) Axial section in the mediastinal window showing hypodense filling defects in the left pulmonary artery and its upper lobar branch, suggestive of pulmonary embolism (white arrows). (B) Axial section in the lung window showing patchy ground-glass opacities in the lower lobes (black arrows), findings consistent with COVID-19 pneumonia.
Chest CT may also be considered in those COVID-19 patients who are at an increased risk for disease progression (age >65 yr and with associated co-morbidities - diabetes, cardiovascular disease, chronic respiratory disease, obesity, hypertension, immune-compromised), have only mild symptoms and a normal/indeterminate CXR, but record arterial oxygen saturation (SpO2) of <93 per cent at rest while breathing normal room air or have an abnormal six-minute walk test (when there is an absolute decrease of >3% in SpO2 after six-minute walk)23. In this subset of patients, chest CT plays a pivotal role in triaging the need for hospitalization and further management as these patients are highly prone to COVID-19–related life-threatening complications and increased mortality.
Recently, the role of serial CT chest in COVID-19 pneumonia has been studied to identify the disease progression by calculating CT involvement/severity scores2425262728. However, its utility in actually changing the patient management in COVID-19 pneumonia remains elusive, which is currently based on the clinical and laboratory parameters of the patient. Moreover, serial CT will also require extra workforce to shift COVID-19 patients to the CT suite and will entail increased risk of infection to the healthcare workers of CT imaging facility. Serial CXR and point-of-care ultrasound usually suffice and remain useful diagnostic tools in most of the cases to look for disease progression in COVID-19 pneumonia, and CT chest in COVID-19–positive patients is indicated only in specific clinical scenarios that have already been described.
COVID-19–recovered patients
CT chest plays a crucial role in the post-COVID-19 phase wherein patients who have recovered from COVID-19 infection present with persistent hypoxia/impaired lung function9. In these patients, a CT scan is useful in differentiating the sequel of COVID-19 infection (post-COVID-19 lung fibrosis) from other treatable causes (Fig. 6).
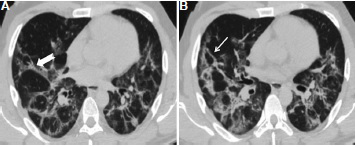
- CT chest of a 55 yr old male patient who had COVID-19 pneumonia a few months back. Symptoms had resolved since then except dyspnoea and hypoxia, which worsened over last few days. RT-PCR test for COVID-19 done on the same day as computed tomography was negative. (A and B) Axial CT sections in lung window showed lung architectural distortion with atelectasis, parenchymal bands (thick arrow), coarse reticulation and irregular interlobular septal thickening (thin white arrow) which was predominant in the lower lobes. The patient gave no history of any occupational exposure or other fibrosing lung disease.
Sometimes, it may be difficult to differentiate post-COVID-19 lung fibrosis from other fibrotic interstitial lung diseases, especially compensated lung fibrosis, which may have remained undiagnosed in the past. The history of occupational exposure and availability of previous imaging (done before the COVID-19 pandemic) for comparison in such cases can be of help as it will not only guide in reaching a quicker and correct diagnosis but will also help in chalking out the appropriate treatment plan.
The sequel of old healed pulmonary TB can be another challenge while interpreting the CT images in patients suspected of post-COVID-19 lung fibrosis. However, the location of abnormalities can help in differentiating post-COVID-19 lung fibrosis from post-tubercular fibrosis. The tubercular fibrotic changes are more commonly seen in the upper lobes (more so in apical regions), while post-COVID-19 lung fibrosis changes are more predominant in the lower lobes and in the peripheral and sub-pleural location29. In addition, the presence of small calcified mediastinal/hilar lymph nodes and pleural thickening points towards changes of sequel of pulmonary TB. In a few instances, post-tubercular lung fibrosis may be indistinguishable from post-COVID-19 fibrosis, and past history of TB and comparison with old imaging (if available) can help in such cases.
The various indications for the use of CT chest in COVID-19 are summarized in the Table.
| COVID-19 screening | CT chest for COVID-19 routine screening is not indicated |
| COVID-19 suspecta | Those who have significant (moderate-to-severe)b respiratory symptoms and a high index of suspicion for COVID-19 but test negative on RT-PCR and have normal/indeterminate CXR |
| COVID-19 positive | Patients who show sudden and/or unexplained clinical deterioration |
| Patients in whom clinical examination or radiographic findings are suspicious of other concurrent lung pathology, which may warrant a change in the treatment plan | |
| Patients with clinical suspicion of pulmonary thromboembolism will require CT pulmonary angiography | |
| Patients who are at an increased risk for disease progression (age >65 yr, associated comorbidities such as diabetes, cardiovascular disease, chronic respiratory disease, obesity, hypertension and immune-compromised), have mildc symptoms with normal/indeterminate CXR, but record SpO2 of <93% at rest while breathing room air or de-saturate on six-minute walk test. CT is useful to triage such patients for need of hospitalization and further management | |
| COVID-19 recovered | Patients who have recovered from COVID-19 infection but on follow up show hypoxia/functional lung impairment. CT chest is needed to differentiate the sequel of COVID-19 infection (lung fibrosis) from other causes |
aDiagnostic accuracy of CT chest in these patients further improves when evaluated in conjunction with other laboratory parameters such as lymphopenia, elevated NLR, D-dimer, CRP, LDH, serum-ferritin and fibrinogen; bModerate-to-severe symptoms: moderate-tosevere dyspnoea and presence of hypoxaemia; cMild symptoms: Fever, cough, sore throat, nasal congestion, malaise, headache, mild or no dyspnoea. RT-PCR, reverse transcription polymerase chain reaction; CXR, chest X-ray; SpO2, arterial oxygen saturation; NLR, neutrophil-lymphocyte ratio; LDH, lactate dehydrogenase; CRP, C-reactive protein
Conclusion
With the continuous surge of COVID-19 cases worldwide, it is imperative for the medical professionals to have knowledge about the appropriate usefulness of CT chest in the diagnosis and management of COVID-19. While routine CT screening for COVID-19 is not recommended, CT chest is an invaluable diagnostic tool in COVID-19 suspects, confirmed and recovered patients in specific clinical scenarios where it is expected to contribute in the disease management and its outcome. Thus, indiscriminate use of CT chest should be discouraged.
Acknowledgment:
Authors thank Dr Jeremy Erasmus (University of Texas, MD Anderson Cancer Centre, USA), Dr Ashish Gupta (The Ottawa Hospital, Ontario, Canada) and Drs Akshay Saxena, Ashish Bhalla and Pankaj Gupta (PGI, Chandigarh) for their invaluable inputs and opinion.
Financial support & sponsorship: None.
Conflicts of Interest: None.
References
- Coronavirus update (Live): 79,331,141 cases and 1,743,079 deaths from COVID-19 virus pandemic. Available from: https://www.worldometers.info/coronavirus/
- Correlation of chest CT and RT-PCR testing for coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology. 2020;296:E32-40.
- [Google Scholar]
- Sensitivity of chest CT for COVID-19: Comparison to RT-PCR. Radiology. 2020;296:E115-7.
- [Google Scholar]
- Diagnostic performance of CT and reverse transcriptase polymerase chain reaction for coronavirus disease 2019: A meta-analysis. Radiology. 2020;296:E145-55.
- [Google Scholar]
- Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): A review. JAMA. 2020;324:782-93.
- [Google Scholar]
- Patients with RT-PCR-confirmed COVID-19 and normal chest CT. Radiology. 2020;295:E3.
- [Google Scholar]
- ACR recommendations for the use of chest radiography and computed tomography (CT) for suspected COVID-19 infection. Available from: https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recommendations-for-Chest-Radiography-and-CTfor-Suspected-COVID19-Infection
- The role of chest imaging in patient management during the COVID-19 pandemic: A Multinational Consensus Statement from the Fleischner Society. Radiology. 2020;296:172-80.
- [Google Scholar]
- Performance of radiologists in differentiating COVID-19 from viral pneumonia on chest CT. Radiology. 2020;296:E46-54.
- [Google Scholar]
- Use of chest imaging in COVID-19: A rapid advice guide; June 11, 2020. Available from: https://apps.who.int/iris/handle/10665/332336
- Chest CT findings in coronavirus disease-19 (COVID-19): Relationship to duration of infection. Radiology. 2020;295:200463.
- [Google Scholar]
- Spectrum of imaging findings in pulmonary infections. Part 1: Bacterial and viral. Pol J Radiol. 2019;84:e205-13.
- [Google Scholar]
- Coronavirus disease 2019 (COVID-19): Role of chest CT in diagnosis and management. AJR Am J Roentgenol. 2020;214:1280-6.
- [Google Scholar]
- Guidelines on Imaging of COVID Patients June 2020 - Under Aegis of ICRI Chest Radiology Sub-Specialty Group. Available from: https://iria.org.in/guidelines-on-imaging-of-Covid-patientsversion-june-2020
- CO-RADS - A categorical CT assessment scheme for patients with suspected COVID-19: Definition and evaluation. Radiology. 2020;296:E97-104.
- [Google Scholar]
- Clinical diagnostic value of CT imaging in COVID-19 with multiple negative RT-PCR testing. Travel Med Infect Dis. 2020;34:101627.
- [Google Scholar]
- A case report of COVID-19 with false negative RT-PCR test: Necessity of chest CT. Jpn J Radiol. 2020;38:409-10.
- [Google Scholar]
- Unraveling the mystery of COVID-19 cytokine storm: From skin to organ systems. Dermatologic Ther 2020:e13859.
- [Google Scholar]
- COVID-19: Coagulopathy, risk of thrombosis, and the rationale for anticoagulation. Clin Appl Thromb Hemost. 2020;26:1076029620938149.
- [Google Scholar]
- Pulmonary embolism in hospitalised patients with COVID-19. Thromb Res. 2020;195:95-9.
- [Google Scholar]
- Proposed modifications in the 6-minute walk test for potential application in patients with mild COVID-19: A Step to optimize triage guidelines. Anesth Analg. 2020;131:398-402.
- [Google Scholar]
- The performance of chest CT in evaluating the clinical severity of COVID-19 pneumonia: Identifying critical cases based on CT characteristics. Invest Radiol. 2020;55:412-21.
- [Google Scholar]
- Relation between chest CT findings and clinical conditions of coronavirus disease (COVID-19) pneumonia: A multicenter study. AJR Am J Roentgenol. 2020;214:1072-7.
- [Google Scholar]
- CT quantitative analysis and its relationship with clinical features for assessing the severity of patients with COVID-19. Korean J Radiol. 2020;21:859-68.
- [Google Scholar]
- Chest CT findings in patients with coronavirus disease 2019 and its relationship with clinical features. Invest Radiol. 2020;55:257-61.
- [Google Scholar]
- CT manifestations of coronavirus disease-2019: A retrospective analysis of 73 cases by disease severity. Eur J Radiol. 2020;126:108941.
- [Google Scholar]
- Thoracic sequelae and complications of tuberculosis. Radiographics. 2001;21:839-58.
- [Google Scholar]




