
Translate this page into:
Comprehensive immune profiling in oral cancers
Informed consent from patients with oral gingivobuccal squamous cell carcinoma procured for sample collection.
*For correspondence: drneerajarora@yahoo.co.in
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
This work was performed at the Laboratory Haematology & Histopathology department, Tata Medical Center, Kolkata, India, from May 2017 to October 2019. Recent advancement in the immunotherapy include characterization of immune infiltrates (such as T cells, Tregs, B cells, NK cells, macrophages and dendritic cells) in tumour microenvironment (TME). In this study, immune cell subsets and checkpoint markers in the TME of oral-gingivobuccal squamous cell carcinoma have been analyzed by flow cytometry immunophenotyping (FCI) as well as immunohistochemistry (IHC). The uniqueness of this study is to identify, quantify and correlate immune cells (CD3, CD4 and CD8); inducible costimulatory molecule (CD278); cytolytic (granzyme) and checkpoint (TIM-3 and PD-1) molecules with the clinicopathological status of the disease and genomics using the same set of tumour samples. The novelty of this study is biomarker identification by FCI and detection of immune prognostication scores by IHC to address novel immunotherapeutic targets. The IHC images in Figure A-D depict a representative case of oral gingivobuccal tumour with increased lymphoid infiltrate. These cells show high programmed death ligand-1 (PDL1) expression (Figure E). The FCI image (Figure G and H) shows increased CD3+ lymphocytes with expression of T cell immunoglobulin and mucin domain-containing-3 (TIM-3), PD-1 and CD278. Multiplex image (Figure F) also shows high expression of CD3, CD68, CD15 and granzyme. Evaluating TME will enhance our knowledge of oral cancer in management of patients for a better disease-free survival.
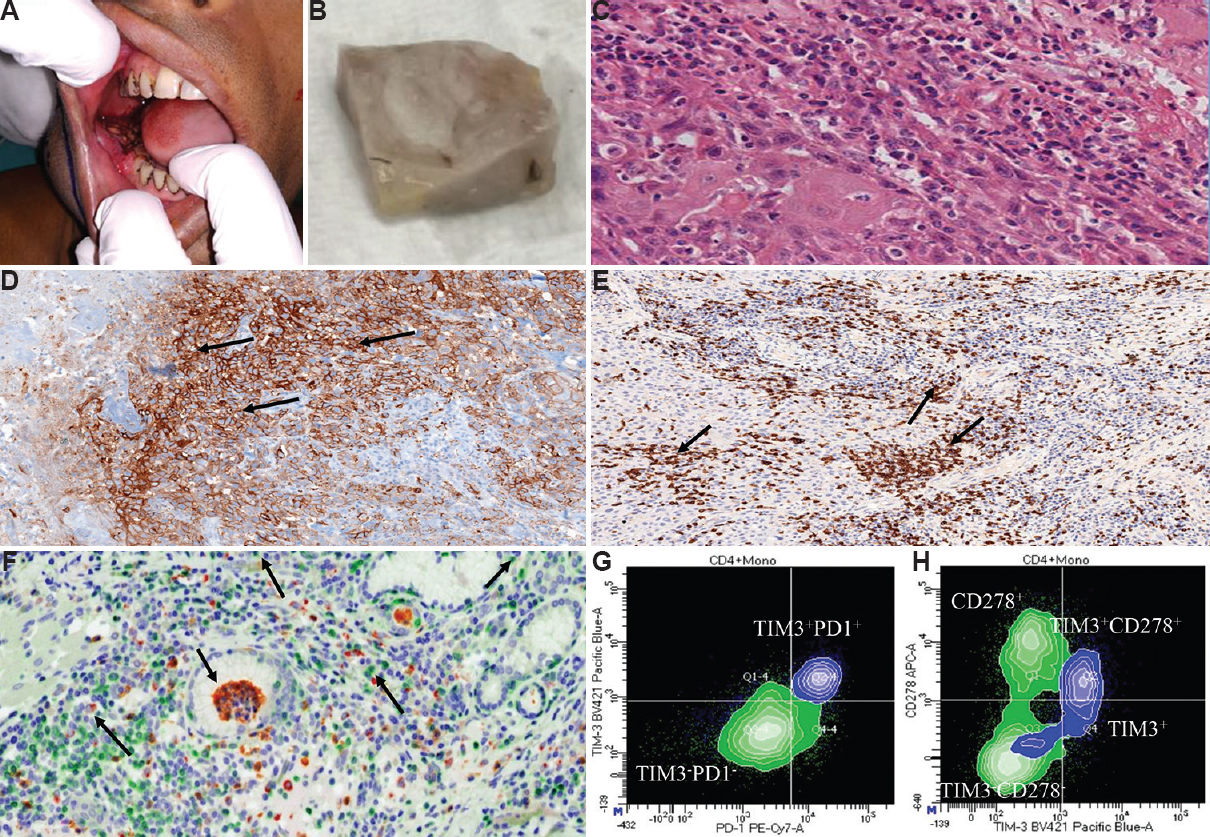
- Immunohistochemistry and flowcytometry images of oral cancer. (A) Irregular growth in lower Gingivobuccal region. (B) Excised tumour from oral cancer patient. (C) Haematoxylin and eosin stain (×40) showing nucleoli islands, each with moderate to abundant cytoplasm, and hyperchromatic nuclei. (D) Scattered brown DAB staining indicates CD3+ lymphocytes (×20). (E) Brown PDL1+ (×20) expressing cells with marginal infiltration. (F) Bright field view (×40) composite CD3, CD15, arginase, granzyme, CD68, nuclei in green, yellow, orange, magenta, red, blue, respectively. (G) TIM3+ PD1+ co-expression in blue monocytes and TIM3-PD1- expressed by green lymphocytes. (H) CD278+ in green lymphocytes & TIM3+CD278+ coexpression in the monocytic population.
Financial support & sponsorship: Authors acknowledge the department of Biotechnology, India, for providing financial support [SyMeC: GIFT study (EC/GOVT/23/17): PI Dr Geetashree Mukherjee].
Conflicts of Interest: None.




