
Translate this page into:
Combating the wrath of viral hepatitis in India
* For correspondence: rkpsdhiman@hotmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
This editorial is published on the occasion of World Hepatitis Day - July 28, 2016.
The viruses which infect the liver and often lead to inflammation of the liver parenchyma are labelled as hepatitis viruses and can be grouped under hepatitis A, B, C, D and E.
Hepatitis A virus (HAV)
Hepatitis A virus (HAV) is a single stranded non-enveloped virus belonging to the Picornaviridae family. It is classically spread via the faecal-oral route and is closely related to the bad hygienic and sanitary conditions in the community. The clinical spectrum of the infection varies widely and is closely linked to the age of the infected individual. With increasing age over 6 yr to adulthood the probability to develop clinical symptoms relating to hepatitis escalates significantly1. HAV is considered to be endemic in India and most of the population is infected asymptomatically in early childhood leading to a lifelong immunity23. Though HAV infection is depicted to be mild and subclinical in most of the cases, mortality increases if it leads onto liver failure or in the presence of an underlying chronic liver disease. A recent study from Pune depicted the changing seroepidemiology of HAV in India wherein the seroprevalence of HAV was demonstrated to be 50.3 per cent in children aged 6 to 10 yr compared to 30.3 per cent in children aged between 18 months to 6 yr4.
Prevention of HAV infection: As faecal-oral route is implicated in the transmission of HAV, adequate disposal of sewage, supplying safe and pure drinking water and improving the personal hygiene practices help in reducing the spread of HAV (Fig. 1). Since 1992, safe and effective vaccines against HAV have been made available worldwide. The various vaccines developed against HAV are similar in efficacy and are highly immunogenic resulting in induction of antibodies which last at least 15 years5.
- Preventive strategies to control HAV and HEV infection.
Inactivated vaccines are derived from the HM 175/GBM strains and virus is inactivated by formalin. The recommended schedule is to give the vaccine in two separate doses six months apart6. Protective titre of antibodies is seen in almost 100 per cent of individuals after receiving the second dose of vaccine. Immunity achieved is usually lifelong and this can be combined with other childhood vaccines as well. The live attenuated vaccine is derived from the H2 strain of the virus and is now licensed to use in India6. The recommended dose is to give one ml of the vaccine subcutaneously to children aged one to 15 yr. Studies from India have depicted more than 95 per cent seroconversion rates six weeks following a single dose of this vaccine, offering a sustained protection for at least two years7.
Indian Academy of Pediatrics recommends two doses for any of the licensed vaccines which has to be given six months apart to children aged one year or older. In immunocompromised individuals and for post-exposure prophylaxis (PEP), inactivated vaccines are preferred2.
Hepatitis B virus (HBV)
Hepatitis B virus (HBV) is a double stranded DNA virus belonging to the family Hepadnaviridae. HBV is transmitted via permucosal or percutaneous exposure to infected body fluids or blood products and has an incubation period averaging around four months. Transmission is known to occur vertically from an infected mother to child, horizontally (e.g. between children in a houshold), sexually and parenterally (e.g. via blood transfusions, intravenous drug abuse, etc.)8.
India has been grouped among countries with intermediate endemicity (2-7%). The predominant mode of transmission in India is horizontal and the common genotypes reported from this part of the world are A followed by D9. The spectrum of HBV infection varies from acute to chronic depending on the duration of persistence of HBV surface antigen (HBsAg) in the serum. Majority of patients with acute infection would remain asymptomatic and only 30 per cent develop icteric hepatitis. The incidence of developing fulminant hepatic failure remains low (0.1-0.5%). When HBsAg persists in the serum for over six months, the patient is depicted to have chronic HBV infection.
Prevention of HBV infection: Prevention of HBV infection should include vigilant screening of blood and blood products and routine testing of tissue and organ donors. Providing needle exchange programmes and harm reduction advice to those actively involved in intravenous drug use (IVDU) and educating regarding the usage of barrier contraceptives (e.g. condoms), promoting safe sexual practices are imperative in preventing HBV infection10. Mother-to-child transmission can be prevented by routine screening of mothers and providing PEP to all infants born to infected mothers. A PEP regimen consisting of hepatitis B immunoglobulin (HBIg) and vaccination can prevent infection of an infant in more than 90 per cent of cases11.
An effective vaccination programme plays an imperative role in preventing HBV infection and is known to decrease the incidence of chronic liver disease and hepatocellular carcinoma (HCC)12. It was recommended by WHO to all countries to incorporate HBV vaccination in their routine immunization programmes in 199213. Studies in the regions of high endemicity have shown a steady decline in the incidence of HBV infection among children to < 2 per cent with the institution of effective vaccination strategies11. The vaccination is done using a three dose schedule (0,1 and 6 months) and is aimed to achieve a protective anti-HBs titre of >10 mIU/ml.
Hepatitis D virus (HDV)
Hepatitis D virus (HDV) is an RNA virus which encodes for a hepatitis D antigen (HDAg), which along with the viral RNA requires encapsidation with HBsAg. A replicative HDV infection requires the presence of HBV infection14. HDV is spread via the parenteral route and can be acquired as either a co-infection (simultaneously with HBV) or a super infection (on a pre-existing HBV infection). HDV infection is infrequent in India15 and preventive strategies would include the same as mentioned for HBV.
Hepatitis C virus (HCV)
The HCV is an enveloped, single stranded RNA virus belonging to the family Flaviviridae. It is divided among six major genotypes with genotype 1 being the most prevalent genotype globally (46%), followed by genotype 3 in 22 per cent and genotypes 2 and 4 in 13 per cent each16. The genotypic distribution of HCV in India suggests genotype 3 to be the commonest (61.8%) followed by genotype 1 (31.2%). Genotypes 2, 4, 5, and 6 have been detected in 0.05-4.5 per cent of cases1718.
Globally, HCV is the predominant cause for post-transfusion hepatitis. The seroprevalence of HCV among general population of India has been reported between 0.22-1.8 per cent1920. The prevalence in the high risk group of patients like IVDU has been reported between 60.4-92.5 per cent2122 in different countries and in those undergoing haemodialysis (HD) between 4.3- 42 per cent2324.
HCV is spread via percutaneous or permucosal exposure to infectious blood or blood products. The high risk groups identified for HCV infection are those receiving multiple blood transfusion (e.g. thalassaemics), engaging in unsafe sexual practices, IVDU, patients on HD, health care workers and transplant recipients25.
Prevention of HCV infection: Preventing HCV should follow a multipronged approach which includes educational counselling regarding the modes of spread of HCV directed not only to the high risk groups but to the general population as well, active screening of the high risk groups to detect patients infected with HCV and prompt treatment of those having active HCV infection with direct acting antivirals (DAAs) to decrease the reservoir pool (Fig. 2).
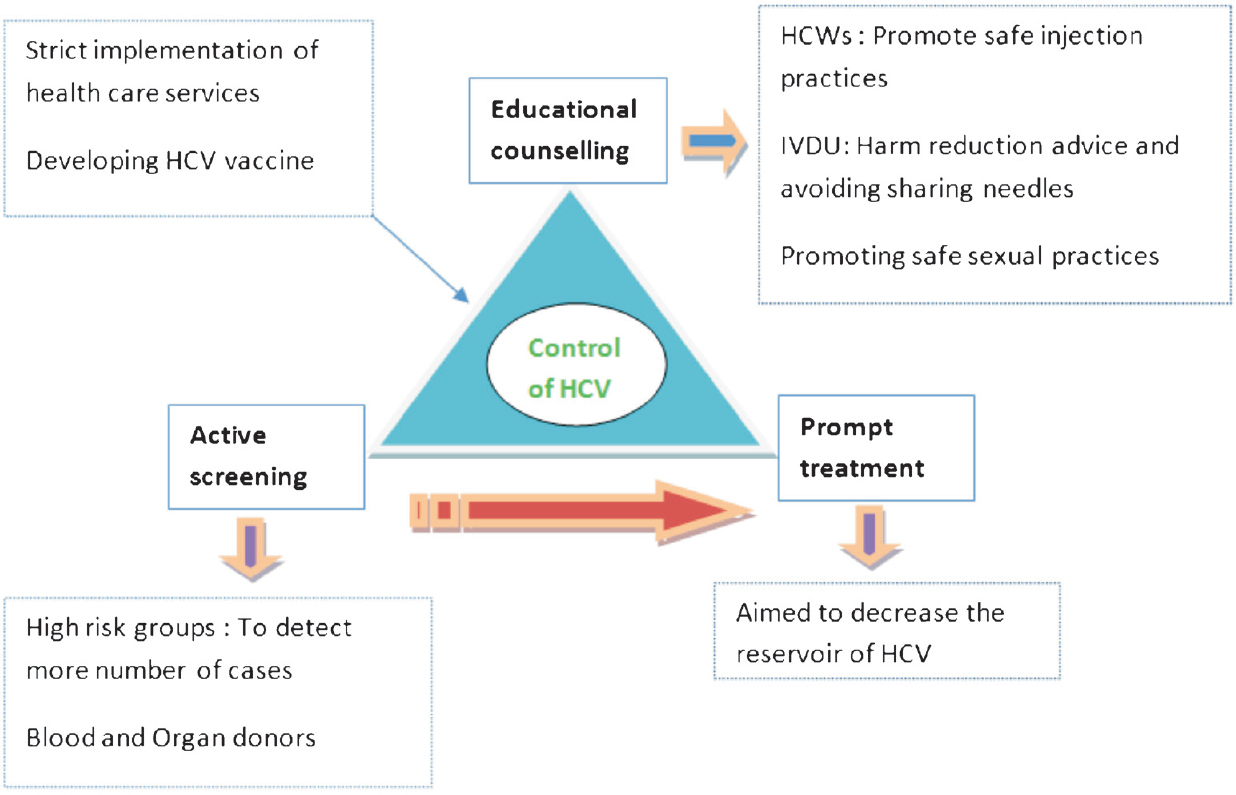
- Preventive strategies to control HCV infection.
The various strategies to control HCV26 include:
-
Improving awareness in the community and provider education: This can be achieved by making an educational curriculum incorporating the aspects of prevention, care and treatment which can be used by multiple health care providers.
-
Improving HCV testing, care and management: This can be attained by making standardized recommendations to guide HCV testing and referral to care. Once tested positive for HCV, one must attain proper ongoing care and be provided with prompt treatment services.
-
Strengthening the public based HCV surveillance programmes: To aptly collect data at the community level to help the local and State based programmes to accurately address HCV related health issues.
-
Screening of high risk groups: Active screening of groups which are linked to a very high risk of acquiring HCV infection (e.g. patients on HD, IVDU).
-
Development of HCV vaccine: As HCV genome demonstrates high level of heterogeneity and mutagenicity, generating an effective vaccine against HCV has remained an unsolved matter. Newer vaccine candidates including recombinant protein, peptide and vector based vaccines have shown promise and have lately entered phase I/II clinical trials27.
-
Dual approach: In India, it was shown that prevention of HCV decreased the overall prevalence but it did not impact the short term liver related mortality or development of HCC28. Thus a dual approach of decreasing the incidence of new cases and treatment of old cases would likely play a vital role in bringing down the burden of the disease29.
Hepatitis E virus (HEV)
Hepatitis E virus is a positive stranded RNA virus which is non-enveloped and belongs to the family Hepeviridae. HEV is deemed as the most frequent cause of acute viral hepatitis (AVH) in India3031. HEV is classified into four major genotypes (1-4) of which genotype 1 is the commonest in India8.
HEV is primarily spread via faecal-oral route, but unlike other viruses spread by this route (e.g. HAV), person-to-person transmission rate is quite low with HEV8. Other modes like vertical and parenteral transmission have been documented32 though the clinical implications remain debatable.
HEV is responsible for a significant proportion of acute viral hepatitis in India and several epidemics related to HEV have been reported3133. HEV infection is attributable not only as a common cause of acute liver failure in India but also to worsening liver function in patients with underlying chronic liver disease, an entity termed as acute-on-chronic liver failure (ACLF)34. During an epidemic, women in the late trimester of pregnancy are infected more frequently (12-20%) than non-pregnant women and men (2-4%)35. The frequency to develop ALF is also significantly higher in pregnant women (15-60%) when compared to non-pregnant women, although pregnancy per se has not regarded as a poor prognostic factor once the patient develops ALF36.
Prevention of HEV infection: Provision of safe, clean drinking water, proper sewage disposal and maintaining good personal hygiene (e.g. hand washing) are imperative to control HEV outbreaks (Fig. 1).
Different types of HEV vaccines are being developed resulting in recombinant protein vaccines, DNA vaccines or recombinant HEV virus like particles (rHEV-VLPs). Recombinant HEV ORF2 has been evaluated as a candidate vaccine and a study from Nepal has demonstrated an efficacy of around 88.5 per cent with the only significant adverse effect being injection site pain37. A recent study demonstrated the long term efficacy of HEV vaccine after being administered in a 3-dose schedule (0, 1 and 6 months). A high vaccine efficacy of 86.8 per cent was demonstrated and 87 per cent of the subjects who received three doses of vaccine maintained an effective antibody titre against HEV for at least 4.5 years38.
Conclusions
Viral hepatitis poses a major health care burden in India and strategies to effectively control the problem are needed. Viruses transmitted via the faecal-oral route (HAV and HEV) can be effectively controlled with the institution of proper sanitary conditions and provision of clean and safe drinking water. Preventive strategies for HBV and HCV include active screening of the high risk groups, stringent application of public based surveillance programmes and development of educational curriculum targeting not only the high risk groups but also the general population. Effective vaccines are now being employed in the preventive strategies against viral hepatitis and coupled with other measures can help effectively tackle the burden of viral hepatitis in India.
References
- Hepatitis A vaccine should receive priority in National Immunization Schedule in India. Hum Vaccin Immunother. 2012;8:1132-4.
- [Google Scholar]
- Seroepidemiology of hepatitis A virus infection among school children in Delhi and north Indian patients with chronic liver disease: implications for HAV vaccination. J Gastroenterol Hepatol. 2003;18:822-7.
- [Google Scholar]
- Changing epidemiology of hepatitis A virus in Indian children. Vaccine Development Therapy. 2014;4:7-13.
- [Google Scholar]
- Indian Academy of Pediatrics (IAP) recommended immunization schedule for children aged 0 through 18 years--India, 2014 and updates on immunization. Indian Pediatr. 2014;51:785-800.
- [Google Scholar]
- Immunogenicity and safety of live attenuated hepatitis A vaccine: a multicentric study. Indian Pediatr. 2009;46:29-34.
- [Google Scholar]
- Hepatitis B virus genotype A is more often associated with severe liver disease in northern India than is genotype D. Indian J Gastroenterol. 2005;24:19-22.
- [Google Scholar]
- Tackling the hepatitis B disease burden in India. J Clin Exp Hepatol. 2014;4:312-9.
- [Google Scholar]
- Toward elimination and eradication of hepatitis B. J Gastroenterol Hepatol. 2010;25:19-25.
- [Google Scholar]
- Prevention of hepatocellular carcinoma in hepatitis B virus infection. J Gastroenterol Hepatol. 2009;24:1352-7.
- [Google Scholar]
- Global programme for control of hepatitis B infection. Vaccine. 1995;13(Suppl 1):S47-9.
- [Google Scholar]
- Latest discoveries on the infection and coinfection with hepatitis D virus. Am Clin Lab. 2002;21:25-7.
- [Google Scholar]
- Prevalence of delta virus infection in high risk population and hepatitis B virus related liver diseases. Indian J Gastroenterol. 1992;11:11-2.
- [Google Scholar]
- Global epidemiology and genotype distribution of the hepatitis C virus infection. J Hepatol. 2014;61(Suppl 1):S45-57.
- [Google Scholar]
- Geographical distribution of hepatitis C virus genotypes in India. Indian J Pathol Microbiol. 2002;45:323-8.
- [Google Scholar]
- Prevalence and geographic distribution of hepatitis C virus genotypes in Indian patient cohort. Infect Genet Evol. 2009;9:643-5.
- [Google Scholar]
- The current seroprevalence of hepatitis C virus in a tertiary care centre in Vellore, Tamil Nadu. Indian J Community Med. 2012;37:137.
- [Google Scholar]
- Prevalence of anti-HCV antibodies in central India. Indian J Med Res. 1996;104:177-81.
- [Google Scholar]
- High hepatitis C virus prevalence and incidence among Canadian intravenous drug users. Int J STD AIDS. 2007;18:23-7.
- [Google Scholar]
- Infection with hepatitis C virus among intravenous-drug users: prevalence, genotypes and risk-factor-associated behaviour patterns in Thailand. Ann Trop Med Parasitol. 2002;96:615-25.
- [Google Scholar]
- Hepatitis B virus and hepatitis C virus co-infection in hemodialysis patients: A retrospective study from a tertiary care hospital of North India. J Nat Sci Biol Med. 2016;7:72-4.
- [Google Scholar]
- Hepatitis C virus infection during haemodialysis in India. J Assoc Physicians India. 1999;47:1139-43.
- [Google Scholar]
- Hepatitis C virus prevention, care, and treatment: from policy to practice. Clin Infect Dis. 2012;55(Suppl 1):S58-63.
- [Google Scholar]
- Future of therapy for Hepatitis C in India: A matter of accessibility and affordability? J Clin Exp Hepatol. 2014;4:85-6.
- [Google Scholar]
- 2014. Disease Burden of Chronic Hepatitis C Virus (HCV) Infection in India. 65th Annual Meeting of the American Association for the Study of Liver Diseases. Available from http://www.centerforda.com/Posters/India%20AASLD%20140930a%20-%20small.pdf
- Common aetiological agent for epidemic and sporadic non-A, non-B hepatitis. Lancet. 1992;339:1509-10.
- [Google Scholar]
- Contribution of hepatitis E virus in acute sporadic hepatitis in north western India. Indian J Med Res. 2012;136:477-82.
- [Google Scholar]
- Sero-epidemiology of hepatitis E virus (HEV) in urban and rural children of North India. Indian Pediatr. 2001;38:461-75.
- [Google Scholar]
- Hepatitis E and acute liver failure in pregnancy. J Clin Exp Hepatol. 2013;3:213-24.
- [Google Scholar]
- A 20-year single-center experience with acute liver failure during pregnancy: is the prognosis really worse? Hepatology. 2008;48:1577-85.
- [Google Scholar]
- Safety and efficacy of a recombinant hepatitis E vaccine. N Engl J Med. 2007;356:895-903.
- [Google Scholar]




