
Translate this page into:
Circulating heat shock protein mRNA profile in gestational hypertension, pre-eclampsia & foetal growth restriction
Reprint requests: Dr Hromadnikova Ilona, Department of Molecular Biology & Cell Pathology, The Third Faculty of Medicine, Charles University, Ruska 87, 100 00 Prague 10, Czech Republic e-mail: ilona.hromadnikova@lf3.cuni.cz
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Heat shock proteins (Hsp) are ubiquitously distributed phylogenetically conserved molecules that regulate cellular homeostasis and maintain the integrity and function of cellular proteins. Increased levels of Hsp in maternal circulation have been shown to be associated with increased risk of pregnancy related complications. The objective of this study was to explore extracellular Hsp mRNA levels in maternal circulation and quantified Hsp27, Hsp60, Hsp70, Hsp90 and Hsp70 binding protein 1 (HspBP1) mRNAs in maternal plasma samples using real-time reverse-transcriptase polymerase chain reaction.
Methods:
Pregnancies with gestational hypertension (GH) (n = 33), pre-eclampsia (PE) with or without foetal growth restriction (FGR) (n = 78) and FGR (n = 25) were involved in the study. Hsp gene expression was analysed in relation to the severity of the disease with respect to the degree of clinical signs, requirements for the delivery and Doppler ultrasound parameters.
Results:
Upregulation of Hsp70 was observed in patients with mild and severe PE (P = 0.004 and P = 0.005, respectively) and in pregnancies complicated with PE delivering before and after 34 wk of gestation regardless of the degree of clinical signs (P = 0.015 and P = 0.009, respectively). No difference in the expression of other Hsp genes among the studied groups was observed. No association between Hsp gene expression and Doppler ultrasonography parameters was found.
Interpretation & conclusions:
These data support that maternal circulation can reflect both maternal and foetal pathologic conditions. Hsp70 represents the sole plasmatic marker, and increased Hsp70 mRNA levels reflect maternal and placental stress response to pregnancy-related complications such as GH and PE, irrespective of the severity of the disease.
Keywords
Foetal growth restriction
gestational hypertension
heat shock protein
maternal circulation
pre-eclampsia

Pre-eclampsia (PE) and foetal growth restriction (FGR) is the major cause of maternal and perinatal morbidity and mortality in 2-10 per cent of pregnant women12. PE is characterized by gestational hypertension (GH) combined with proteinuria after 20 wk of gestation3. FGR is defined as foetal growth less than the 10th percentile for appropriate gestational age. The causes of PE and FGR remain unknown. It is believed that PE results mainly from defective placentation and insufficient maternal spiral artery remodelling that elicit inadequate uteroplacental blood perfusion, ischaemia and finally generalized maternal systemic inflammatory response456. Elevated amounts of pro-inflammatory cytokines, chemokines and adhesion molecules in the maternal circulation have been shown to play a central role in the excessive systemic inflammatory response and in the generalized endothelial dysfunction characteristics of PE7. Moreover, pre-eclamptic patients have been demonstrated to have significantly higher levels of C-reactive protein and particular complement components including terminal complement complex SC5b98.
Heat shock proteins (Hsps) are ubiquitously distributed phylogenetically conserved molecules present in the cells of all living organisms. Under physiological conditions, the stress proteins are expressed in low concentrations as the constitutive proteins, regulating cellular homeostasis and maintaining the integrity and function of other cellular proteins910. Human Hsps are categorized under distinct families based on their functions in the cells, their homologies in the primary structures and their approximate molecular weight, measured in kDa. These families are as follows: a family of small Hsps, Hsp40, Hsp60, Hsp70, Hsp90 and Hsp11011.
Elevated circulating Hsp70 concentrations reflecting systemic inflammation, oxidative stress and hepatocellular injury were found to be associated with an increased risk of several pregnancy-related complications including transient hypertension of pregnancy, PE, haemolysis, elevated liver enzymes, low platelet syndrome and pre-term delivery121314151617. Elevation of circulating Hsp70 levels was also observed in pregnant asthmatic women compared to healthy pregnant women18.
Since most investigators studied Hsp expression at protein level in placental tissues19202122 and maternal circulation (serum or plasma samples)12131415161718, we focused on the examination of Hsp expression at mRNA level. Among differentially expressed proteins, previous studies identified Hsp27 and Hsp70 to be upregulated in placental tissues derived from patients with PE19202122. Several researchers pointed to the fact that the expression of various Hsps might vary in different placental zones. Although the protein levels of total Hsp60 and Hsp90 did not differ in placental and decidual tissues between normal and complicated pregnancies2324, the expression of Hsp27, Hsp60, Hsp70 and Hsp90 was shown to be higher in the thrombus and lower in the infarction than in control samples25. A novel Hsp70 co-chaperone called Hsp70 binding protein 1 (HspBP1) was included in the study since this intracellular protein abundant in tissues, was found to inhibit substantially antiapoptotic function of Hsp7026.
There is a lack of information on Hsp27, Hsp60, Hsp70, Hsp90 and HspBP1 gene expression in patients affected with PE and/or FGR. We therefore, undertook this study to evaluate Hsp mRNA levels as also Hsp BP1 level in plasma samples from pregnant women with GH.
Material & Methods
This study was designed in a retrospective consecutive manner within the period ranging from January 2011 to January 2014. Samples of maternal peripheral blood from complicated pregnancies were collected at the Institute for the Care of the Mother and Child (Prague, Czech Republic), mostly during the hospital admission. Samples from pregnancies with the normal course of gestation were collected during regular check-up in the 36th wk of gestation in the Clinic of Obstetrics and Gynecology, University Hospital Motol (Prague, Czech Republic). The study included 78 pregnant women with clinically established PE with or without FGR, 25 pregnancies complicated by FGR, 33 with GH and 39 normal pregnancies. Of the 78 patients with PE, 27 had symptoms of mild PE and 51 women were diagnosed with severe PE. Thirty pre-eclamptic women required the delivery before 34 wk of gestation and 48 women delivered after 34 wk of gestation. PE occurred both in previously normotensive patients (56 cases) and in a form superimposed on previous hypertension (22 cases). Seven growth-retarded foetuses were delivered before 34 wk of gestation and 18 after 34 wk of gestation. Oligohydramnios or anhydramnios was present in nine growth-restricted foetuses. The examination of the flow of blood vessels (Doppler ultrasonography) showed an abnormal pulsatility index (PI) in the umbilical artery (abnormal values above the 95th percentile detected in 12 pre-eclamptic and 14 FGR cases) and/or in the middle cerebral artery (abnormal values below the 5th percentile detected in 9 pre-eclamptic and 5 FGR cases). Cerebroplacental ratio (CPR), expressed as a ratio between middle cerebral artery and umbilical artery PI, was below the 5th percentile in 17 cases (8 pre-eclamptic and 9 FGR cases). Absent or reversed end-diastolic velocity waveforms in the umbilical artery occurred in four cases (2 pre-eclamptic and 2 FGR cases).
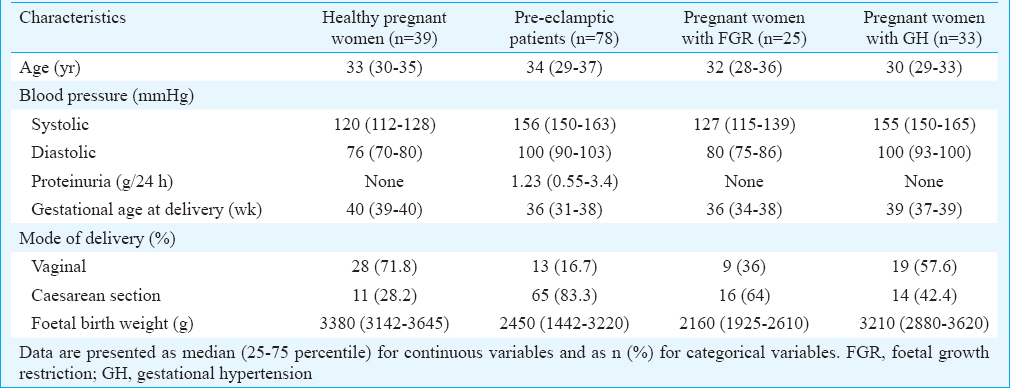
Women with normal pregnancies were defined as those without medical, obstetrical or surgical complications at the time of the study and who subsequently delivered full-term, singleton, healthy infants weighing >2500 g after 37 completed wk of gestation. PE was defined as blood pressure >140/90 mmHg in two determinations four hours apart that was associated with proteinuria >300 mg/24 h after 20 wk of gestation3. Severe PE was diagnosed by the presence of one or more of the following findings: (i) systolic blood pressure >160 mmHg or diastolic blood pressure >110 mmHg, (ii) proteinuria >5 g of protein in a 24 h sample, (iii) very low urine output (<500 ml in 24 h), (iv) signs of respiratory problems (pulmonary oedema or cyanosis), (v) impairment of liver function, (vi) signs of central nervous system problems (severe headache and visual disturbances), (vii) pain in the epigastric area or right upper quadrant, (viii) thrombocytopenia, and (ix) presence of severe FGR3. FGR was diagnosed when the estimated foetal weight, calculated using the Hadlock formula (Astraia Software GmbH), was below the 10th percentile for the evaluated gestational age, adjustments were made for the appropriate population standards of the Czech Republic. The clinical characteristics of the normal and complicated pregnancies are shown in Table I. All patients who participated in this study provided written informed consent. The study was approved by the Ethics Committee of the Third Faculty of Medicine, Charles University in Prague.
Processing of samples and total RNA isolation: Peripheral blood (9 ml) was collected into ethylenediaminetetraacetic acid tubes and centrifuged twice at 1200 g for 10 min at room temperature. Plasma samples were stored at −80°C until further processing. Total RNA was extracted from one ml of maternal plasma using RNeasy Mini Kit (Qiagen, Hilden, Germany) according to manufacturer's instructions. To minimize DNA contamination, the eluted RNA was treated with five μl of deoxyribonuclease I (DNase I, Fermentas International, Ontario, Canada) for 30 min at 37°C.
Analysis of relative Hsp gene expression using real-time RT (reverse transcriptase)-PCR: All PCR reactions were performed using an ABI PRISM 7500 Sequence Detection System (Applied Biosystems, USA) as previously described27. Human Hsp and β-actin primers and probes were designed using Primer Express version 2.0 (Applied Biosystems, USA). The primer/probe sequences and concentrations used for the amplification of the target and reference genes were as follows (5΄→3΄):
Hsp27, HSPB1: forward primer 5΄-TCCCTGGATGTCAACCACTTC-3΄ (900 nmol/l); reverse primer 5΄-TCTCCACCACGCCATCCT-3΄ (900 nmol/l); probe 5΄-(FAM) CCCCGGACGAGCTGACGGTC (TAMRA)-3΄ (300 nmol/l).
Hsp60, HSPD1: forward primer 5΄-GATGTTGATGGAGAAGCTCTAAGTACA-3΄ (900 nmol/l); reverse primer 5΄-TGCCACAACCTGAAGACCAA-3΄ (900 nmol/l); probe 5΄-(FAM) TCGTCTTGAATAGGCTAAAG (MGB)-3΄ (200 nmol/l).
Hsp70, HSPA1A: forward primer 5΄-ACCAAGCAGACGCAGATCTTC-3΄ (300 nmol/l); reverse primer 5΄- GCCCTCGTACACCTGGATCA-3΄ (300 nmol/l); probe 5΄-(FAM) CCTACTCCGACAACCAACCCGGG (TAMRA)-3΄ (200 nmol/l).
Hsp90α, HSP90AA1: forward primer 5΄-TGCGGTCACTTAGCCAAGATG-3΄ (300 nmol/l); reverse primer 5΄-GAAAGGCGAACGTCTCAACCT-3΄ (300 nmol/l); probe 5΄-(FAM) CCCAGACCCAAGACCAACCGATGG (TAMRA)-3΄ (200 nmol/l).
HspBP1, HSPBP1: forward primer 5΄-TGGCCGACCTGTGTGAGA-3΄ (700 nmol/l); reverse primer 5΄-GCAGGTGCATGCCAGACA-3΄ (700 nmol/l); probe 5΄-(FAM) CATGGACAATGCCG (MGB)-3΄ (200 nmol/l).
B-actin, ACTB: forward primer 5΄-CCTGGCACCCAGCACAAT-3΄ (300 nmol/l for Hsp27, Hsp60, Hsp70, Hsp90α and 200 nmol/l for HspBP1); reverse primer 5΄-GCCGATCCACACGGAGTACT-3΄ (300 nmol/l for Hsp27, Hsp60, Hsp70, Hsp90α and 200 nmol/l for HspBP1); probe 5΄-(VIC) ATCAAGATCATTGCTCCTCCTGAGCGC (TAMRA)-3΄ (200 nmol/l for Hsp27, Hsp60, Hsp70, Hsp90α and 100 nmol/l for HspBP1).
To perform one-step duplex quantitative RT-PCR assay27, the Hsp gene and endogenous control β-actin were amplified in the same tube in a reaction volume of 25 μl consisting of 1× TaqMan One-step RT-PCR Master Mix, TaqMan and/or MGB probes, forward and reverse primers (Hsp and β-actin primers and probe; Applied Biosystems, USA). Ten nanogram of extracted total RNA from maternal plasma was used for the detection of Hsp27, Hsp60, Hsp70, Hsp90 and HspBP1. Each sample was analysed in duplicate. The thermal profile for one-step real-time RT-PCR included reverse transcription at 48°C for 30 min, denaturation at 95°C for 10 min, followed by 50 cycles of PCR with denaturation at 95°C for 15 sec and annealing/extension at 60°C for one minute. For the analysis of relative changes in gene expression, the comparative CT method28 was used to interpret the data. The difference (ΔCT) between the CT values of the Hsp and the endogenous control was calculated for each sample. RNA isolated from a randomly selected placenta derived from gestation of normal course was chosen as the reference for each comparison. The comparative ΔΔCT calculation involved finding the difference between each sample's ΔCT and the reference's ΔCT. Finally, ΔΔCT values were transformed to absolute values using the formula 2−ΔΔCT.
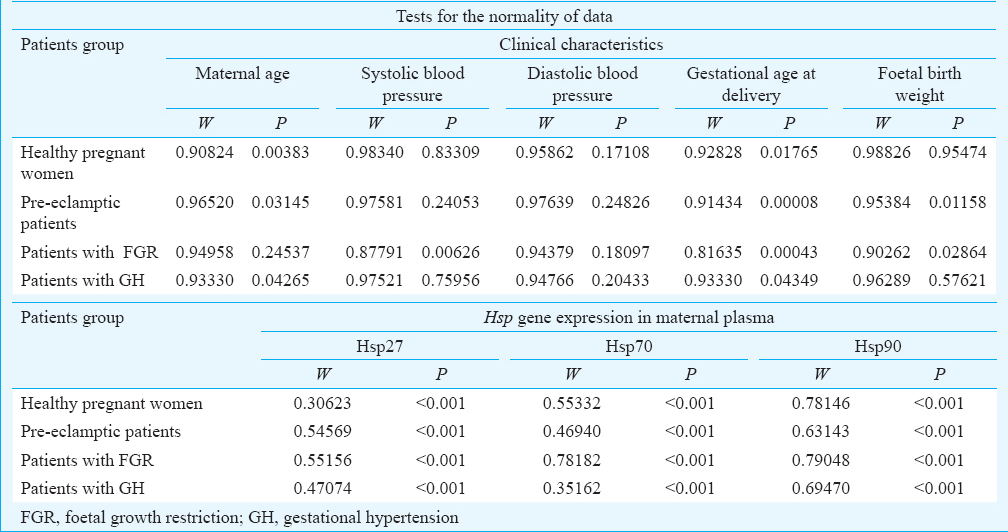
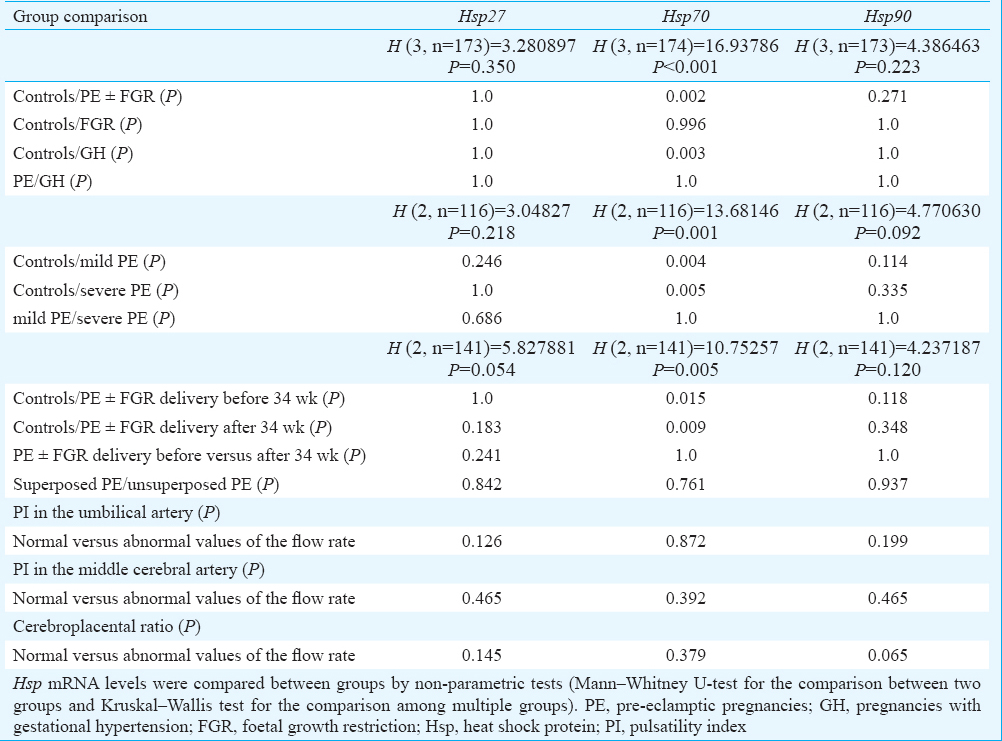
Statistical analysis: Tests of normality of the population distribution of random characteristics (patients’ age, systolic and diastolic blood pressure, gestational age at delivery and foetal birth weight) together with the tests of normality of observed data (Hsp gene expression in maternal plasma samples) were performed using Shapiro–Wilk test. Half of the clinical characteristics in groups of normal and complicated pregnancies did not show a normal distribution. Further, all experimental data did not follow a normal distribution (Table II). Therefore, Hsp mRNA levels were compared between groups by non-parametric tests (Mann–Whitney U-test for the comparison between two groups and Kruskal–Wallis test for the comparison among multiple groups) using Statistica software (version 9.0, StatSoft, Inc., Tulsa, OK, USA). Odds ratio (OR), the likelihood that the outcome occurred in the exposure/intervention group as compared to the control group, was calculated using MedCalc (MedCalc Software bvba, Microsoft Partner, Silver Application Development, Ostend, Belgium).
Results
Given that HspBP1 was not detectable in maternal plasma samples and Hsp60 showed positive amplification in a limited number of maternal plasma samples, it was decided to exclude them from further analyses. Subsequently, it was determined whether plasma concentrations of Hsp27, Hsp70 and Hsp90 mRNAs were related to pregnancy complications.
Hsp gene expression in maternal plasma samples in patients with pregnancy-related complications: Overall, significantly increased expression was observed only for Hsp70 (P < 0.001) in women with pregnancy-related complications (GH, PE and/or FGR) compared to pregnancies with normal course of gestation. Kruskal–Wallis analysis revealed Hsp70 overexpression in the group of patients with PE with or without FGR (P = 0.002) and GH (P = 0.003), but not in the group of patients with FGR. Plasma levels of Hsp70 mRNA between the groups of patients with PE with or without FGR and GH did not differ (Fig. 1). The odds of having Hsp70 mRNA levels above cut-off (median plus standard deviation of normal pregnancies) was similar between the groups of patients with PE with or without FGR [P < 0.001; OR: 8.31; 95% confidence interval (CI): 2.69-25.62] and GH (P < 0.001; OR: 8.23; 95% CI: 2.38-28.44). The expression of Hsp27 and Hsp90 did not differ between the control group and pregnancies affected with GH, PE with or without FGR and FGR.
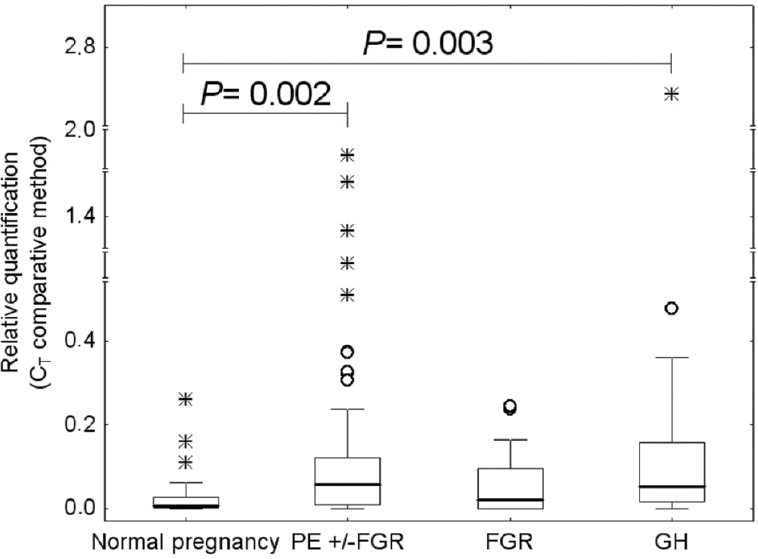
- Heat shock protein 70 (Hsp70) overexpression in maternal plasma samples derived from patients with gestational hypertension (GH) and pre-eclampsia (PE) with or without foetal growth restriction (FGR).
Association of Hsp gene expression in maternal plasma samples and severity of disease with respect to clinical signs, requirements for the delivery and Doppler ultrasonography monitoring: Hsp gene expression was analysed in relation to the severity of the disease with respect to the degree of clinical signs (mild and severe PE) and requirements for the delivery (before and after 34 wk of gestation). When compared to normal pregnancies, significant upregulation of Hsp70 was observed in patients with mild and severe PE (P = 0.004 and P = 0.005, respectively, Fig. 2) and in pregnancies complicated with PE with or without FGR delivering before and after 34 wk of gestation regardless of the degree of clinical signs (P = 0.015 and P = 0.009, respectively, Fig. 3). However, Hsp70 mRNA levels did not differ between the patients with mild and severe PE (Fig. 2) and between those who delivered before and after 34 wk of gestation (Fig. 3). The highest estimated odd ratios of having Hsp70 mRNA levels above cut-off (median plus standard deviation of normal pregnancies) were detected in patients with severe PE (P<0.001; OR: 9.84; 95% CI: 3.05-31.77) and those who delivered before 34 wk of gestation (P < 0.001; OR: 11.44; 95% CI: 3.24-40.4) when compared with the group of patients with mild PE (P = 0.003; OR: 7.0; 95% CI: 1.94-25.25) and those who delivered after 34 wk of gestation (P<0.001; OR: 8.05; 95% CI: 2.47-26.18).
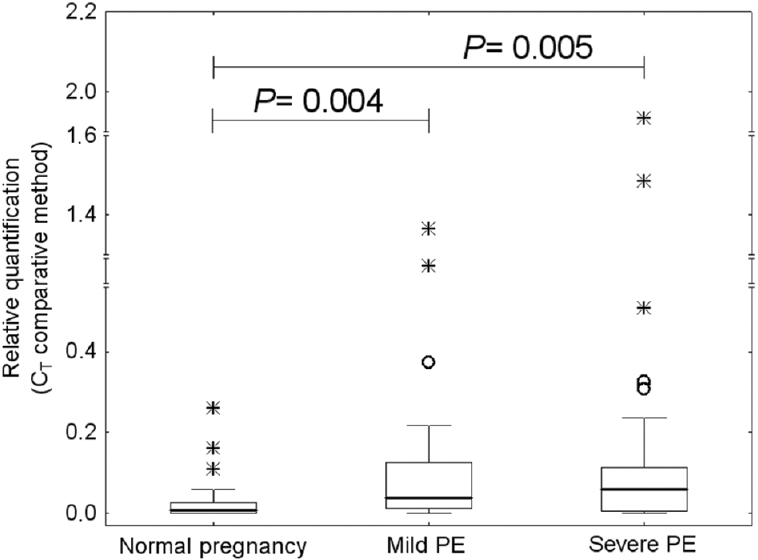
- Increased circulating heat shock protein 70 (Hsp70) mRNA levels in patients with mild and severe pre-eclampsia (PE).
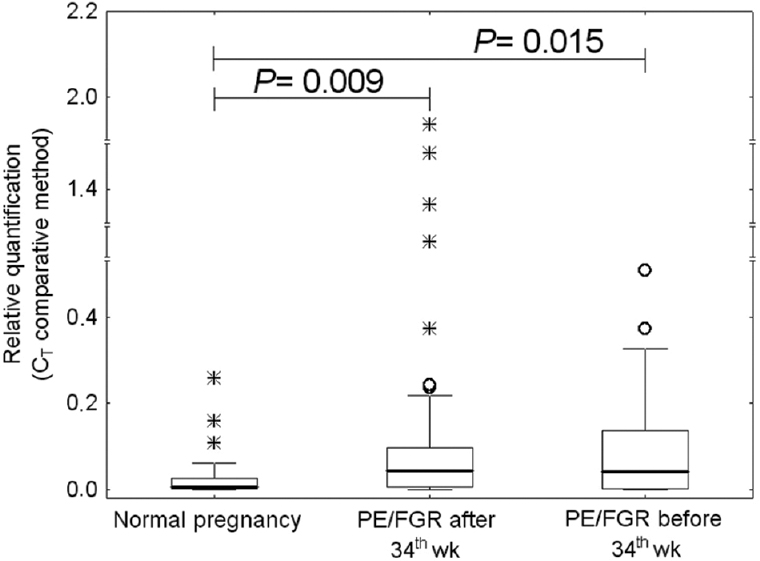
- Increased circulating heat shock protein 70 (Hsp70) mRNA levels in pregnancies complicated with pre-eclampsia (PE) with or without foetal growth restriction (FGR) delivering before and after 34 wk of gestation.
No difference in Hsp gene expression between the groups of patients with mild or severe PE and controls was found. Similarly, Hsp mRNA levels did not differ between pre-eclamptic pregnancies with requirements for the delivery before and after 34 wk of gestation and controls. In addition, the association between Hsp gene expression and the occurrence of previous hypertension in the group of patients with PE was determined. The analyses revealed no difference between the group of PE superposed on chronic hypertension and/or GH and the group of patients with unexpected onset of PE.
The association between Hsp gene expression in maternal plasma and Doppler ultrasonography parameters was analysed in the pregnancies complicated with PE and/or FGR. The difference within the group of complicated pregnancies with normal and abnormal values of flow rates was assessed. The analysis showed no effect of the PI in the umbilical artery, the PI in the middle cerebral artery and the CPR on Hsp mRNA levels in maternal circulation. Summary of data resulting from statistical analyses is shown in Table III.
Discussion
Circulating nucleic acids such as DNA, mRNA and microRNAs present in maternal plasma or serum samples are increasingly being used as biomarkers for monitoring of pregnancy-related complications. Extracellular nucleic acids present in maternal circulation are predominantly haematopoietic in origin29. Placental insufficiency-related pregnancy complications have been shown to be associated with an excessive placental trophoblast apoptosis and shedding of placenta debris45. The Redman hypothesis proposes that release of a continuous stream of placental debris into the maternal circulation provokes a systemic inflammatory response in all women, which is exaggerated, if the burden of the debris is abnormally high (when the placenta is oxidatively stressed secondary to spiral artery disease) or if the woman responds excessively to the process45. PE usually appears when the inflammatory responses begin to decompensate. The problem with the placenta is generally considered to be an inadequate uteroplacental circulation leading to placental hypoxia, oxidative stress and, in the most severe cases, infarction. Two abnormalities, affecting the spiral arteries, are known to predispose to PE: the arteries may be either too small because of deficient placentation, or obstructed because of acute atherosis or both45.
We hypothesize that maternal circulation can reflect both maternal and placental pathologic conditions through the mediation of diverse Hsp gene expression profiles. Since Hsp60 and HspBP1 mRNA are not detectable in maternal plasma samples and Hsp27 and Hsp90 mRNA show comparable levels regardless of the course of gestation, Hsp70 represents the sole plasmatic marker. Increased Hsp70 mRNA levels reflect maternal and placental stress response to pregnancy-related complications such as GH and PE. Our data supported the finding of other investigators who reported significantly higher protein levels of total Hsp70, constitutive and induced forms of Hsp70 in PE along with oxidative stress in placental tissues202122. Our finding was in compliance with the results of other studies demonstrating elevated circulating Hsp70 concentrations in pregnancy-related complications including transient hypertension of pregnancy and PE121314151617. Hsp70 represents an antioxidative stress marker. The overexpression of Hsp70 and the heat shock transcription factor (Hsf1) seen in the pre-eclamptic endothelial cells suggests its possible protective role as stress-specific natural adaptive response against the generated stress30. As proposed by Molvarec et al15, we hypothesise that haemodynamic stress, oxidative stress (placental or systemic), placental ischaemia, ischaemia of other organs as well as maternal systemic inflammatory response may contribute to the overexpression of Hsp70, resulting in elevated circulating Hsp70 levels. The possible cause of Hsp70 mRNA overexpression in the maternal circulation of women with PE may be a compilation of several events: the activation of circulating maternal leucocytes, mainly monocytes, as a response to placental hypoxia and excessive amount of placental debris in maternal circulation. Both activated maternal leucocytes and placental debris released into maternal circulation may be a source of high circulating Hsp70 mRNA levels.
Former studies evaluating the relationship between PE or intrauterine growth restriction and expression of total Hsp60 and Hsp90 revealed that a stress response in placental and decidual tissues, as determined by immunohistochemical and immunofluorescence analyses, was not associated with pregnancy outcome2324. Most likely, there will be very low levels of Hsp60 mRNA inside placental debris released into maternal circulation throughout gestation. Our unpublished data also revealed very low levels of Hsp60 mRNA in maternal whole peripheral blood samples derived from women with normal and complicated pregnancies. That could be the reason for rarely detectable circulating Hsp60 mRNA in maternal plasma samples.
We presumed that very low (hardly detectable) HspBP1 mRNA circulating levels were closely related to the high Hsp70 mRNA extracellular levels. Hsp70 directly inhibits apoptosis. HspBP1 binds to the ATPase domain of Hsp70 and inhibits its ability to refold denatured proteins26. Molar ratio of HspBP1 to Hsp70 in cells is an important determinant of the function of the resulting complex. The excess of HspBP1 enhances the proapoptotic effect in all cells and vice versa, the lack of HspBP1 enables Hsp70 to carry out cytoprotective properties through its antiapoptotic function.
In conclusion, our findings support that women with pregnancy-related complications may benefit from the exploration of extracellular Hsp70 mRNA levels in maternal circulation.
Acknowledgment
This work was supported by the Charles University research programme PRVOUK P32, Czech Republic.
Conflicts of Interest: None.
References
- Geographic variation in the incidence of hypertension in pregnancy. World Health Organization International collaborative study of hypertensive disorders of pregnancy. Am J Obstet Gynecol. 1988;158:80-3.
- [Google Scholar]
- ACOG Committee on Practice Bulletins – Obstetrics. ACOG practice bulletin. Diagnosis and management of preeclampsia and eclampsia. Number 33, January 2002. Obstet Gynecol. 2002;99:159-67.
- [Google Scholar]
- Preeclampsia: an excessive maternal inflammatory response to pregnancy. Am J Obstet Gynecol. 1999;180(2 Pt 1):499-506.
- [Google Scholar]
- Preeclampsia and the systemic inflammatory response. Semin Nephrol. 2004;24:565-70.
- [Google Scholar]
- Inadequate maternal vascular response to placentation in pregnancies complicated by pre-eclampsia and by small-for-gestational age infants. Br J Obstet Gynaecol. 1986;93:1049-59.
- [Google Scholar]
- Circulating cytokines, chemokines and adhesion molecules in normal pregnancy and preeclampsia determined by multiplex suspension array. BMC Immunol. 2010;11:59.
- [Google Scholar]
- Activation of the complement system in normal pregnancy and preeclampsia. Mol Immunol. 2010;47:1500-6.
- [Google Scholar]
- Heat shock response of eukaryotic cells. Berlin: Springer-Verlag; 1984. p. :7-10.
- The stress response, function of the proteins, and perspectives. In: Stress Proteins in Biology and Medicine. New York: Cold Spring Harbor Laboratory Press; 1990. p. :1-37.
- [Google Scholar]
- Guidelines for the nomenclature of human heat shock proteins. Cell Stress Chaperones. 2009;14:105-11.
- [Google Scholar]
- Serum levels of heat shock protein 70 in patients with preeclampsia: a pilot-study. Wien Klin Wochenschr. 2002;114:730-2.
- [Google Scholar]
- Association of elevated serum heat-shock protein 70 concentration with transient hypertension of pregnancy, preeclampsia and superimposed preeclampsia: a case-control study. J Hum Hypertens. 2006;20:780-6.
- [Google Scholar]
- Association of increased serum heat shock protein 70 and C-reactive protein concentrations and decreased serum alpha(2)-HS glycoprotein concentration with the syndrome of hemolysis, elevated liver enzymes, and low platelet count. J Reprod Immunol. 2007;73:172-9.
- [Google Scholar]
- Increased serum heat-shock protein 70 levels reflect systemic inflammation, oxidative stress and hepatocellular injury in preeclampsia. Cell Stress Chaperones. 2009;14:151-9.
- [Google Scholar]
- High levels of heat shock protein 70 are associated with pro-inflammatory cytokines and may differentiate early- from late-onset preeclampsia. J Reprod Immunol. 2013;100:129-34.
- [Google Scholar]
- Elevated serum 70 kDa heat shock protein level reflects tissue damage and disease severity in the syndrome of hemolysis, elevated liver enzymes, and low platelet count. Eur J Obstet Gynecol Reprod Biol. 2008;139:133-8.
- [Google Scholar]
- Increased circulating heat shock protein 70 levels in pregnant asthmatics. Cell Stress Chaperones. 2010;15:295-300.
- [Google Scholar]
- Heat shock protein 27 in the placentas of women with and without severe preeclampsia. Clin Exp Obstet Gynecol. 2004;31:12-4.
- [Google Scholar]
- Placental heat shock protein 70 overexpression confers resistance against oxidative stress in preeclampsia. Turk J Med Sci. 2008;38:27-34.
- [Google Scholar]
- Expression of heat shock protein 70 and endothelial nitric oxide synthase in placental tissue of preeclamptic and intrauterine growth-restricted pregnancies. Pathol Res Pract. 2010;206:651-6.
- [Google Scholar]
- Effect of HSP70 and 90 in modulation of JNK, ERK expression in preeclamptic placental endothelial cell. Cell Biochem Biophys. 2012;64:187-95.
- [Google Scholar]
- Placental heat shock proteins: No immunohistochemical evidence for a differential stress response in preterm labour. Gynecol Obstet Invest. 1995;40:236-43.
- [Google Scholar]
- Heat shock proteins and heat shock protein-antibody complexes in placental tissues. Infect Dis Obstet Gynecol. 1999;7:180-5.
- [Google Scholar]
- Changed expression of heat shock proteins in various pathological findings in placentas with intrauterine fetal growth restriction. Med Electron Microsc. 2004;37:170-6.
- [Google Scholar]
- Inhibition of Hsp70 ATPase activity and protein renaturation by a novel Hsp70-binding protein. J Biol Chem. 1998;273:32883-8.
- [Google Scholar]
- Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) method. Methods. 2001;25:402-8.
- [Google Scholar]
- Nonhematopoietically derived DNA is shorter than hematopoietically derived DNA in plasma: a transplantation model. Clin Chem. 2012;58:549-58.
- [Google Scholar]
- Over expression of HSP70 and HSF1 in endothelial cells during preeclamptic placental stress. Aust N Z J Obstet Gynaecol. 2011;51:47-52.
- [Google Scholar]




