Translate this page into:
Central pontine myelinolysis
+For correspondence: Shyam Tent House Bus Stand Manoharpur Shahpura Jaipur 303 104, India drkhosya3@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 58-year old man presented to M.B.S Hospital, Government Medical College, Kota, Rajasthan, with non-projectile vomiting and watery diarrhoea for the last three days. On admission, his initial blood tests were within normal range except for severe hyponatremia with a sodium level of 100 mmol/l (normal, 135-145 mmol/l). Normal saline was administered intravenously, and the sodium level began to normalize at 100, 106, 122 and 130 mmol/l on days 2, 3, 5 and 7, respectively. One week later, he had complaints of difficulty in swallowing and speaking accompanied by unsteadiness of gait and eventual inability to walk. Initial magnetic resonance imaging (MRI) (Fig. 1) and computed tomography (CT) of the brain on day 7 showed no abnormality. However, his condition continued to deteriorate, and a repeat MRI on day 14 revealed a well-defined lesion in the pons of low T1 signal intensity (Fig. 2) as well as a lesion of high T2 signal intensity (Fig. 3). A diagnosis of central pontine myelinolysis (CPM) was made.
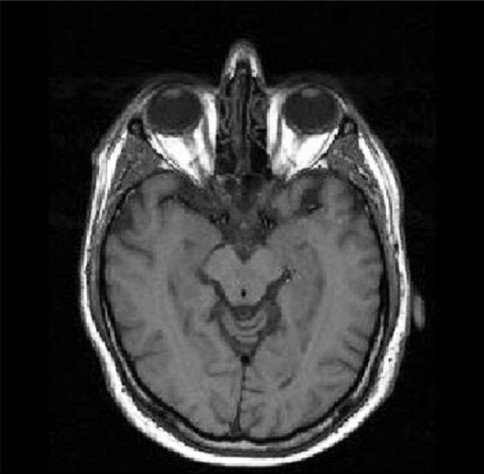
- T1 weighted MR image of the brain
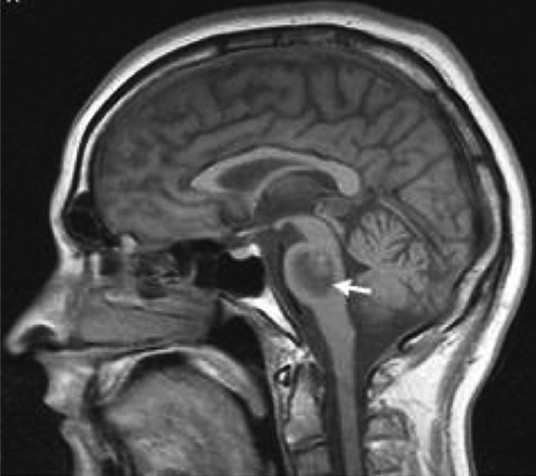
- Brain MRI of the patient showing a low T1 signal intensity lesion (day 14).
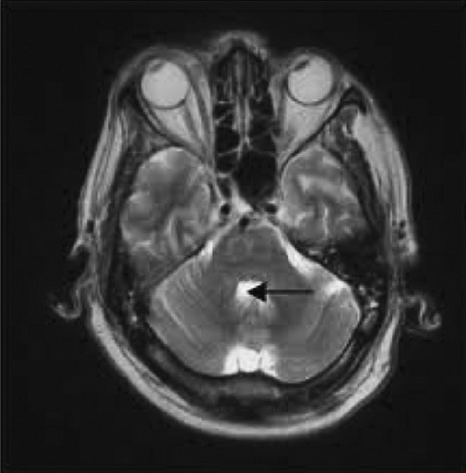
- T2 - weighted image of hyperintensity in the pons (black arrow) consistent with CPM (day 14).
CPM is an subacute demyelinating condition of the brain stem and a recognized complication of the treatment of patients with chronic hyponatremia (>48 h)1. The risk of CPM is believed to be associated with a rapid (>8 mmol/l/day) correction or overcorrection of the serum sodium concentration. However, there is no accepted safe rate of correction2. Conventional imaging findings (MRI and CT) lag behind clinical manifestations, thus limiting the utility of imaging in early diagnosis. Imaging is advocated later to confirm CPM diagnosis3. There are no effective therapeutic methods for CPM treatment and recovery varies ranging from none to substantial improvement4. Although the use of plasmapheresis (PP) and immunoglobulins (IVIg) has been reported in analogous situations, support for their use in the liver transplant population is limited but, there is no clear evidence as to why PP and IVIG may help reverse the neurologic sequelae of CPM. However, it has been suggested that the initial osmotic stress results in the release of myelinotoxic products that can lead to demyelination567.
References
- Neurologic complications after solid organ transplantation. Transpl Int. 2009;22:269-78.
- [Google Scholar]
- Outcome of central pontine and extrapontine myelinolysis (n = 44) J Neurol. 1999;246:700-5.
- [Google Scholar]
- Treatment of central pontine myelinolysis with therapeutic plasmapheresis. Lancet. 1999;353:1155.
- [Google Scholar]
- Immunoglobulins are effective in pontine myelinolysis. Clin Neuropharmacol. 2000;23:110-3.
- [Google Scholar]
- Treatment of central pontine myelinolysis with plasmapheresis and immunoglobulins in liver transplant patient. Transpl Int. 2008;21:390-1.
- [Google Scholar]




