
Translate this page into:
Bubbles in the belly – Cystic mesothelioma
*For correspondence: anuradhachandramohan@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 25 yr old female† first presented to the department of Medicine and subsequently referred to the department of Surgery, Christian Medical College, Vellore, India, in December 2018, with abdominal pain and distension for six months. Investigations revealed high serum ascites albumin gradient (SAAG), low protein massive ascites with negative tests for tuberculosis, Budd-Chiari syndrome and malignant ascites. Ascites persisted despite empirical anti-tuberculosis therapy for nine months.
Computed tomography revealed atypical features of loculated ascites scalloping the liver and mild omental thickening (Fig. 1). Further, magnetic resonance imaging in October 2019 revealed multiloculated cystic lesions filling the peritoneal cavity (Fig. 2), further confirmed by laparoscopy (Fig. 3) suggestive of cystic mesothelioma. Histopathology of the lesional biopsy with calretinin and D2-40 immunohistochemical staining confirmed cystic mesothelioma (Fig. 4). Upon three months follow-up, the patient had persistent ascites and was advised cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC), which she is yet to have.
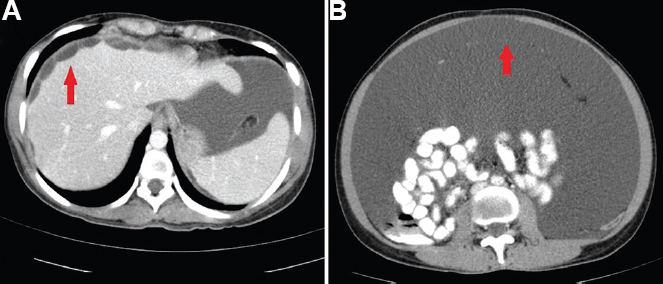
- (A) Contrast-enhanced axial computed tomography images showing loculated ascites with multiple thin septae, scalloping of the liver (arrow) and (B) mild omental thickening (arrow).
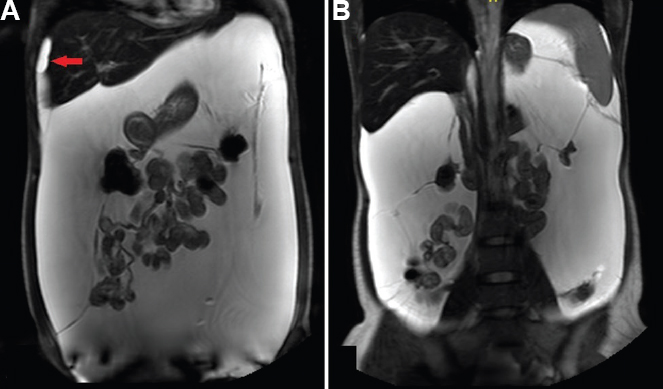
- (A and B) T2-weighted coronal magnetic resonance imaging showing multi-loculated thin-walled cystic lesions filling the peritoneal cavity and scalloping the liver surface (arrow in A).
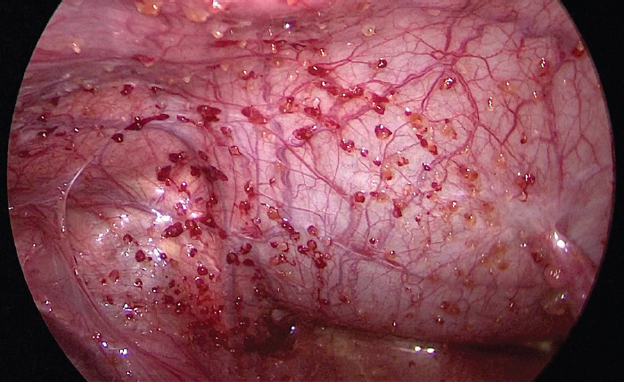
- Intra-operative photograph obtained during diagnostic laparoscopy showing multiple cystic lesions studding the peritoneal cavity.
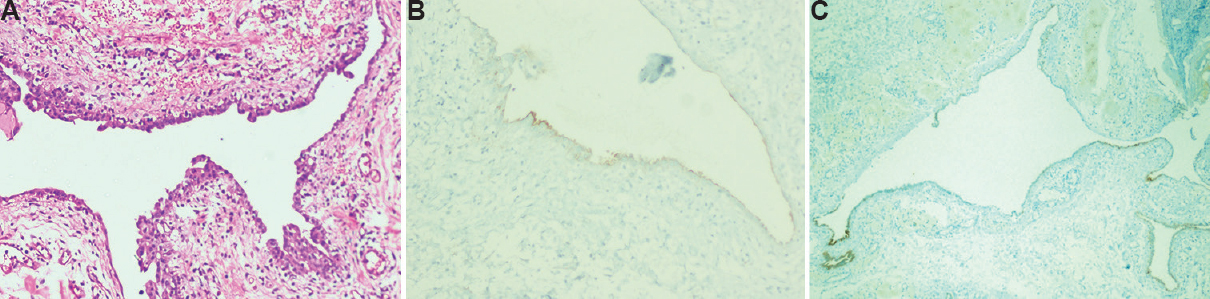
- (A) High-power photomicrograph (H and E, ×100) showing a flat layer of mesothelial cells lying on a loose fibrous stroma. (B) High-power photomicrograph (×100) with D2-40 immunohistochemical staining showing D2-40 expression by the neoplastic cells which outline the shape of the cysts. (C) Low-power photomicrograph (×40) with calretinin immunohistochemical staining showing calretinin expression by the neoplastic cells which outline the shape of the cysts.
Acknowledgment:
Authors acknowledge Dr Rijo Issac, department of Pathology, and Dr Abimanesh, department of Medicine, CMC, Vellore, for working up the patient.
Conflicts of Interest: None.




