
Translate this page into:
Boerhaave’s syndrome: A case of spontaneous oesophageal rupture
*For correspondence: 13004396890@163.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 57 yr old male† was admitted to the emergency department of Northern Jiangsu People’s Hospital, Jianglu Province, China, with epigastric pain after an episode of vomiting after he drank a bottle of beer in May 2018. Since he suffered from a peptic ulcer, abdominal computed tomography was carried out and emergency exploratory laparotomy was performed in order to repair gastric perforation. However, there was no sign of gastric perforation was found during the procedure. The occurrence of spontaneous gastro-oesophageal junction rupture, a special type of Boerhaave’s syndrome (Figure A) was then considered. Oesophagogastroscopy was carried out, revealing a lower oesophageal perforation extending up to the epicardia (Figure B). A diagnosis of Boerhaave’s syndrome was made, the patient’s vomiting due to drinking had precipitated gastro-oesophageal junction rupture. Surgical repair of the Oesophageal perforation followed by jejunostomy were done. Postoperatively, the patient was transferred to the intensive care unit for further conservative treatment. He recovered after a 25-day hospital stay. Postoperative follow-up showed that he recovered well.
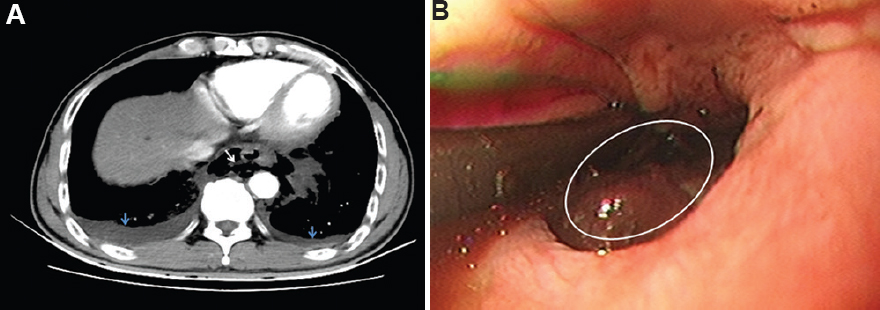
- (A) Oesophageal rupture with air leakage into the mediastinum (white arrow) and bilateral pleural effusion (blue arrow). (B) Oesophagogastroscopy was performed showing a full-thickness rupture of the oesophageal wall (circled area).
Conflicts of Interest: None.




