
Translate this page into:
Bilateral acute ophthalmic artery occlusion in a case of giant cell arteritis
* For correspondence: rayrupak@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
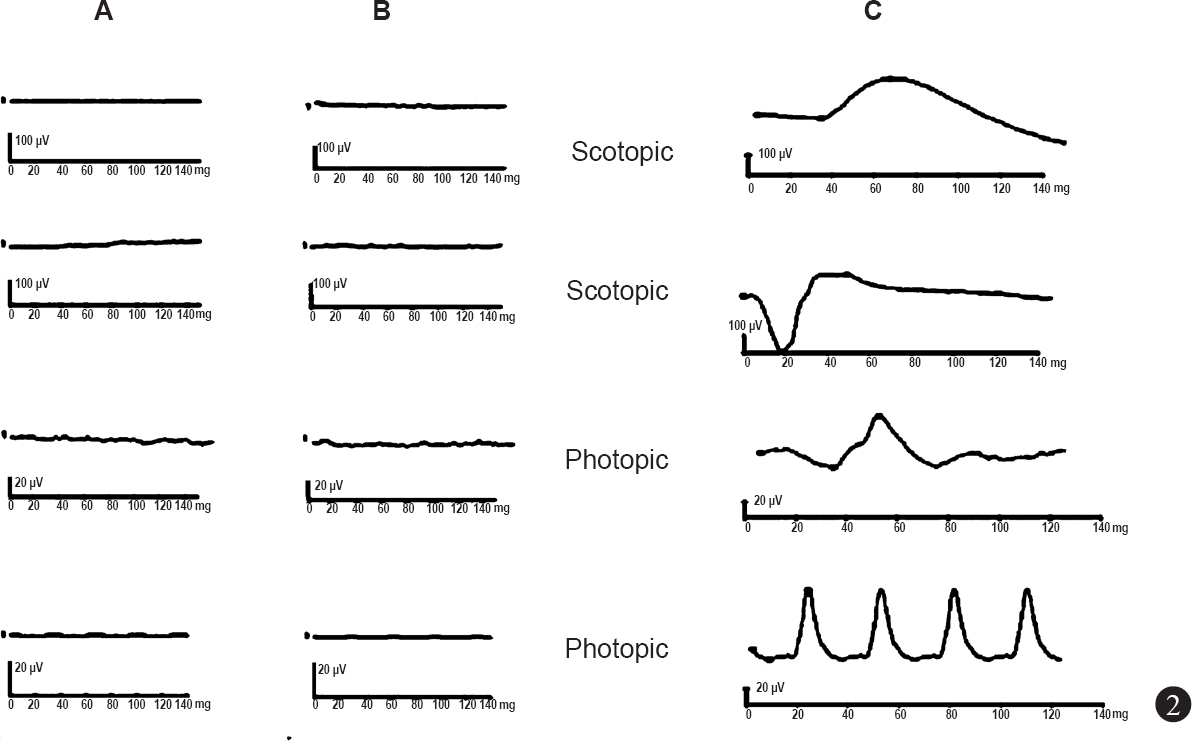
A 52 year old female presented with complaints of sudden, painless loss of vision in both eyes (right eye followed by left eye with in a gap of 3 days) since preceding one week to Aditya Birla Sankara Nethralaya, Kolkata in August 2014. Her visual acuity in both eyes was ‘no perception of light’. She gave a history of fever, weight loss and scalp tenderness one month prior to the visual loss. She had tenderness on temporal artery palpation on right side. Fundus examination showed disc oedema in both eyes along with retinal oedema at the posterior pole and a cherry red spot (Fig. 1A,B). Fundus fluorescein angiography showed no filling of retinal arteries at 30 sec after injection (Fig. 1 C, D). Full field electroretinography showed non-recordable scotopic and photopic responses. (Fig. 2). Erythrocyte sedimentation rate was 140 mm/h by Westergren method and C-reactive protein level was markedly elevated at 96 mg/l. She was diagnosed to be a case of bilateral ophthalmic artery occlusion with anterior ischaemic optic neuropathy secondary to giant cell arteritis (GCA). She was started on three days of pulse methyl prednisolone followed by oral systemic corticosteroids in consultation with her physician. At final follow up after three months there was no improvement in visual acuity. This case highlights the importance of early diagnosis and prompt treatment of giant cell arteritis in order to prevent the blinding complications like ophthalmic artery occlusion, and in case of unilateral involvement, to save the other eye.

-
A, B. Fundus photograph showing disc oedema in both eyes (white arrow), with retinal oedema at the posterior pole along with cherry red spot at the fovea (black arrowhead). (C). Fundus fluorescein angiography of the right eye at 30 sec shows no choroidal filling and no filling of the retinal arteries. (D). Left eye shows no filling of retinal arteries with patchy choroidal filling (white arrow).
-
A, B. Full field electroretinogram (ERG) of right (A) and left (B) eye shows extinguished scotopic and photopic responses. Fig. 2C shows ERG responses in normal eye.




