Translate this page into:
Association of socio-economic status with family history in adult patients with asthma
Reprint requests: Dr Nallur B. Ramachandra, Genomics Laboratory, Department of Studies in Zoology, University of Mysore, Manasagangothri, Mysore 570 006, India e-mail: nallurbr@gmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Socio-economic status is associated with increased morbidity in patients with asthma. The aim of the present study was to assess the association between socio-economic status and family history of asthma in adult asthma patients.
Methods:
The study included 200 adults with asthma and 400 non-asthmatic controls. Socio-economic status was determined based on income. Regression analysis was used to estimate odd ratios in relation to socio-economic class, using age, gender, family history of asthma and smoking habits.
Results:
The highest occurrence of having any family history of asthma was observed in the high class group (88.2%), followed by upper middle class (79.5%), lower middle class (60%) and the lowest in the low class group (34%). Having any family history of asthma was an important risk factor in both univariate and multivariate analyses in lower middle class, upper middle class and high class, but not in the low class group.
Interpretation and conclusions:
The results indicated a positive association between having a family history of asthma and higher socio-economic status. Further studies on a large representative sample need to be conducted to confirm these findings.
Keywords
Asthma
family history
socio-economic status

Asthma is a chronic inflammatory disease of the airways of the lung. Three hundred million people are reported to be affected by asthma worldwide with asthma prevalence increasing globally by 50 per cent every decade1. There are also reports of increasing asthma prevalence in developing countries. Based on a survey conducted in four cities in India, prevalence of asthma was estimated to be 2.38 per cent2. A more recent report, estimated the national burden of asthma at 17.23 million3.
Multiple studies have been carried out to investigate the causes and risk factors of developing asthma. It has been suggested that interactions among multiple genes and environmental factors increase asthma susceptibility4. There are evidences of familial aggregation of asthma and atopy and having a family history of asthma is considered as one of the most important risk factors for developing the disease5. Socio-economic status (SES) of an individual is an environmental factor which has been identified as an important determinant of human health6. Individual-level SES has been associated with worse asthma morbidity in patients with asthma7. In epidemiology, SES may be assessed by using a series of indicators which includes individual level indicators such as education, occupation and income, and area level indicators which are based on residential areas and are drawn from census data. Several studies in different part of the world have made an attempt to investigate the effect of SES on prevalence and severity of asthma8910. While atopy is reported to be more common in higher SES groups11, establishing such association between asthma and SES has been more challenging and the study results are inconsistent. Further, most of such studies have been carried out in developed countries and are mainly on childhood asthma. Studies on adults have revealed both increased1213 and decreased1415 asthma prevalence in higher SES groups, while some studies have found no association between the two16. Association between the SES and asthma inheritance in subjects with adult onset asthma is less clear. The present study was undertaken to assess the association between SES and family history of asthma in adult patients.
Material & Methods
The patients with adult onset asthma were selected from a tertiary care asthma center (Allergy, Asthma and Chest Center), at Mysore, Karnataka, in India during 2009-2010. Assuming history of maternal and paternal asthma of 20 per cent in cases and 10 per cent in controls with a 1:2 case control ratio, a sample size of 195 cases and 390 controls was required to detect the level of significance at 0.05 with a power of 90 per cent. Therefore, 200 cases and 400 controls and their families were selected for a study undertaken to evaluate association of maternal and paternal asthma with the risk of development of adult onset asthma in children. The present study was a sub-study in the same population to assess the association between socio-economic status and having a family history of asthma.
The asthmatics were diagnosed and categorized based on asthma severity into mild persistent, moderate persistent and severe persistent. The diagnosis of asthma and its severity were done according to Global Initiative for Asthma guidelines (GINA).17 Among 200 adults included in the study, 45 were classified as poor or low class (LC), 60 adults were classified as lower middle class (LMC), 78 were classified as upper middle class (UMC) and 17 as high class (HC) according to the guidelines by Agarwal18.
Asthma in the index adult was diagnosed according to GlNA guidelines with reversible airway obstruction of 12 per cent and 200 ml improvement in FEV1 after inhalation of salbutamol. Spirometry was performed according to American Thoracic Society Guidelines19.
Measurements of SES: Information on individual SES was derived based on per capita monthly income18. Residence in particular localities of the city, classified according to easily ascertainable characteristics of housing was also taken into account. The income according to the Income Tax returns was utilized to classify the subjects. According to the guidelines, there are six social classes based on per capita monthly income (i) Upper high class with  10000 and above per capita monthly income; (ii) High class with 5000-9999 per capita monthly income; (iii) Upper middle class with 3000-4999 per capita monthly income; (iv) Lower middle class with 1500-2999 per capita monthly income; (v) Poor with 500-1499 per capita monthly income; and (vi) Very poor or below poverty line (BPL) with below 500 per capita monthly income. Four classes, namely low class or poor, lower middle class, upper middle class and high class were included in this study. Since among the index asthmatic cases included in the study, there were no subjects belonging to the very low and very high socio-economic classes, no control cases belonging to these classes were included in the study. Other individual level variables were age, gender, religion and smoking status.
10000 and above per capita monthly income; (ii) High class with 5000-9999 per capita monthly income; (iii) Upper middle class with 3000-4999 per capita monthly income; (iv) Lower middle class with 1500-2999 per capita monthly income; (v) Poor with 500-1499 per capita monthly income; and (vi) Very poor or below poverty line (BPL) with below 500 per capita monthly income. Four classes, namely low class or poor, lower middle class, upper middle class and high class were included in this study. Since among the index asthmatic cases included in the study, there were no subjects belonging to the very low and very high socio-economic classes, no control cases belonging to these classes were included in the study. Other individual level variables were age, gender, religion and smoking status.
Selection of the controls: Controls were selected to match the socio-economically classified adult patients. A total of 400 adults were selected as controls: 90 were selected from poor or low class, 120 from lower middle class, 156 from upper middle class and 34 adults from high class categories. A total of 400 families were thus included. To be considered as a control, the adult individual was asked if he or she has ever been diagnosed as having asthma by a doctor (physician diagnosed asthma). Control group was homogeneous for age, gender and religion. Four wards were randomly selected from the general population of Mysore city and controls were classified as belonging to various socio-economic strata based on per capita monthly income18.
Inclusion and exclusion criteria: Cases: Adults aged > 18 yr; confirmed diagnosis of asthma according to GINA guidelines; and onset of asthma after the age of 18 yr. The asthmatic patients were included only if they had their first respiratory symptoms after the age of 18 yr. The patients who had any chronic respiratory symptoms during childhood were excluded from the study.
Controls: Adults aged >18 yr; no respiratory symptoms suggestive of asthma. Controls belonging to very low and very high socio-economic classes were excluded from the study.
Methodology: A genetic register was designed for the study. The structured questionnaire validated before administering which included data on patient demographics, respiratory symptoms, triggers and medications used. It also included information on the subject's family history of asthma. For an index asthmatic adult, questions were asked regarding the presence of doctor diagnosed asthma in any member of his/her family such as parents, grandparents, aunt/uncles and siblings. In case, the patient had children, it was asked if any of them had doctor diagnosed asthma. In family history “Any” term was used to indicate the presence of asthma in any one or more of the family members of the asthmatic proband.
The study protocol was approved by the Institutional Human Ethical Committee (IHEC) of the University of Mysore, and informed written consents were obtained from all cases and controls.
Statistical analysis: Odds ratio and 95% confidence interval were estimated to assess the association between different SES and family history of asthma. Statistical significance was analyzed by Chi-square test and logistic regression analysis was performed with SPSS version 18 software (IBM, USA) to assess independent association of variables found to be significant in univariate analysis.
Results
The mean age of study subjects was 40 ± 13 yr in cases and 39 ± 13 yr in controls and male-female ratio was 41.5: 58.5. There was no significant age and sex difference between the two groups (Table I). The presence of family history of asthma in subjects stratified according to their SES is presented in Table II.

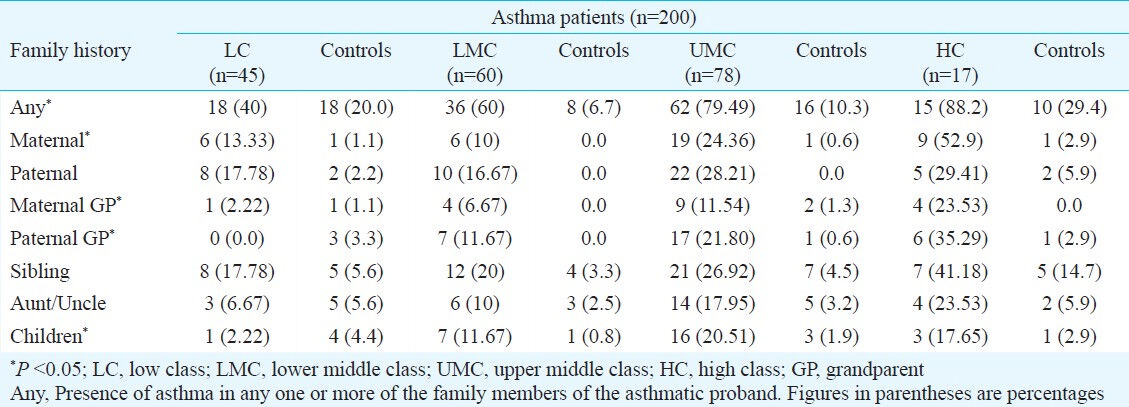
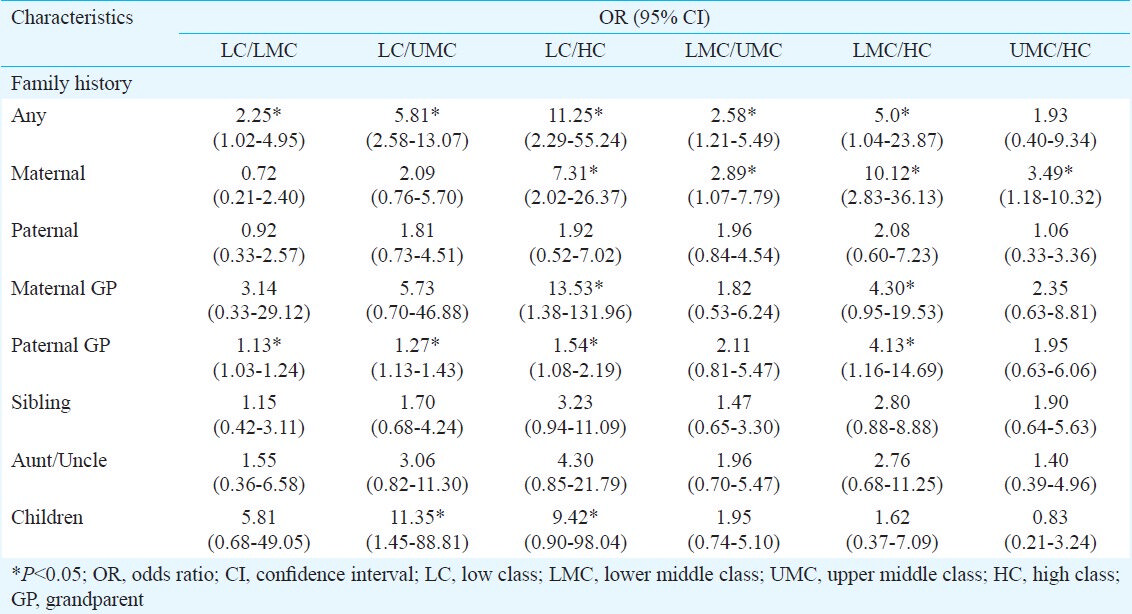
Among the 200 socio-economically classified patients, the highest occurrence of having any family history of asthma was observed in the high class group and this was followed by upper middle class, lower middle class and the lowest in the low class group showing the significant difference between the four groups (Table II). Maternal history of asthma together with maternal and paternal grandparent history of asthma and having asthmatic children showed significant difference between the four groups (Table II). Univariate analysis was carried to compare the presence of having a different family history of asthma between each groups among patients and the odds ratios showing the relative risk for adult onset asthma in the index case were recorded (Table III). Except for upper middle class and high class, all groups showed significant differences in having any family history of asthma. The highest odds ratio was observed between the low class and the high class (OR=11.25, 95% CI=2.29-55.24) (Table III).
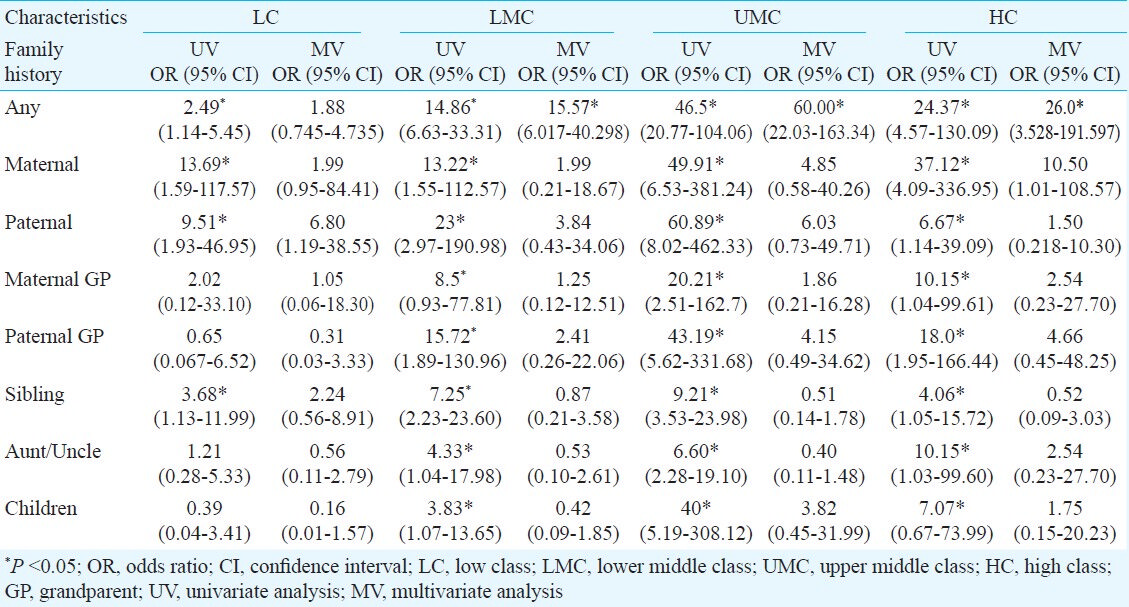
Both univariate and multivariate logistic regressions were used to compare the effect of SES on asthma inheritance among asthmatics and controls. Having any family history of asthma was an important risk factor in both univariate and multivariate analyses in lower middle class, upper middle class and high class, but it is significant only in univariate analysis in the low class group (Table IV).
Discussion
Regression analysis was carried out to study the associations between the SES of the index case with adult onset asthma and the presence of family history of asthma. Comparisons were also made between index asthmatic cases and non-asthmatic controls and the presence of family history of asthma. It was observed that patients with high SES were more likely to have a family history of asthma, independent of age, sex, asthma severity and smoking status.
In this study, information on individual SES was based on per capita monthly income as the main criterion which has also been used by others20. In countries like USA and Canada low income was shown to be associated with increased prevalence of asthma, as well as with increased hospitalization and mortality rates2122. Our study showed that the SES was related to having a family history of asthma which itself is a risk factor in developing the disease. Several mechanisms by which SES may influence asthma include differences in the level of exposure to indoor allergens, cigarette smoking and air pollution. Aeroallergen sensitization, which is a precursor of allergic diseases such as asthma, was affected by area of residence such as urban, semi-urban and rural areas, and could also be a surrogate marker for socio-economic status in young atopic patients23. Also factors such as obesity, diet, exposure to stress and depression may partly explain the differences in asthma prevalence mediated by SES9. Several risk factors that have been investigated in adult asthma include atopy, gender, age, obesity, cigarette smoking, SES and having family history of asthma and/or other allergic diseases. Among these factors, family history of asthma and atopy have been introduced as the strongest risk factors in adult asthma5. In an earlier study conducted in Mysore, India, family history of asthma was reported to be significantly associated with developing asthma in adults24 confirming the genetic background of the disease. There are evidences that heredity and family history of allergic disease modify the response to hygiene related environmental factors25. Both the maternal allergic phenotype and maternal environmental exposures in pregnancy are suggested to critically determine the risk of subsequent infant allergic disease through alterations in DNA and histone methylation, histone acetylation and chromatin structure26. Exposure to cats has been shown to protect against the presence of allergy to cat among adult and children with a family history of allergic illness but not among people without a family history of allergy27. Also, neonatal BCG vaccination was reported to protect against subsequent development of wheeze and airway hyper-responsiveness (AHR) in a cohort of Australian-born children of ethnic Chinese with a family history of allergic disease but not in those without a positive family history28. Such evidences indicate that there are genetic determinants of this protective effect. As most forms of asthma are believed to have their origins in early life,30 it is not clear whether a positive family history and/or maternal environmental exposures during pregnancy are relevant in adult asthma and the related factors need to be ascertained in further studies. Therefore, it is likely that SES is a surrogate marker for various environmental determinants involved in gene-by-environment interactions causing differences in development of asthma among different groups of socio-economic classes.
One of the limitations of this study was that the patients were recruited from the asthma clinic of a single tertiary care centre, which may not be representative of the general population. The control population though identified from the general population was limited to four administrative wards and may not be representative of Mysore. Another limitation was that all the environmental variables that are associated with SES could not be assessed. Further, Agarwal's criteria used in this study may not have represented the socio-economic status completely. The other limitation was information bias if index cases and controls did not have a precise knowledge of their family members having asthma. Despite these limitations, the results of the present study provided an interesting insight about the effect of SES on asthma inheritance in subjects with adult onset asthma.
In conclusion, the present study showed an association between increasing SES and high occurrence of family history of asthma. Further studies on a larger, representative population of adults in India are needed to confirm these findings.
References
- Global Initiative for Asthma (GINA) program. The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy. 2004;59:469-78.
- [Google Scholar]
- Prevalence and risk factors for bronchial asthma in Indian adults: a multicentre study. Indian J Chest Dis Allied Sci. 2006;48:13-22.
- [Google Scholar]
- Indian study on epidemiology of asthma, respiratory symptoms and chronic bronchitis in adults (INSEARCH) Int J Tuberc Lung Dis. 2012;16:1270-7.
- [Google Scholar]
- Major gene effect and additive familiar pattern of inheritance of asthma exist among families of probands with sickle cell anemia and asthma. Am J Hum Biol. 2008;20:149-53.
- [Google Scholar]
- The association between family history of asthma and the prevalence of asthma among US adults: National Health and Nutrition Examination Survey, 1999-2004. Genet Med. 2009;1:323-28.
- [Google Scholar]
- Socioeconomic status and health: what we know and what we don’t. Ann N Y Acad Sci. 1999;896:3-15.
- [Google Scholar]
- Individual-level socioeconomic status is associated with worse asthma morbidity in patients with asthma. Respir Res. 2009;10:e125.
- [Google Scholar]
- Association between socioeconomic status and the development of asthma: analysis of income trajectories. Am J Public Health. 2010;100:540-6.
- [Google Scholar]
- Asthma and ethnic minorities: socioeconomic status and beyond. Curr Opin Allergy Clin Immunol. 2009;9:154-60.
- [Google Scholar]
- Low socioeconomic status as a risk factor for asthma, rhinitis and sensitization at 4 years in a birth cohort. Clin Exp Allergy. 2005;35:612-8.
- [Google Scholar]
- Family size, infection and atopy: the first decade of the “hygiene hypothesis”. Thorax. 2000;55:S2-10.
- [Google Scholar]
- Different shapes for different folk: socioeconomic and racial/ethnic disparities in asthma and hay fever among 173, 859 U.S men and women. Environ Health Respect. 2002;110:211-6.
- [Google Scholar]
- Asthma and wheezy bronchitis in adolescents: biosocial correlates. J Asthma. 1988;25:125-9.
- [Google Scholar]
- Socioeconomic and occupational groups and risk of asthma in Sweden. Occup Med (Oxf). 2008;58:161-8.
- [Google Scholar]
- Social class in asthma and allergic rhinitis: a national cohort study over three decades. Eur Respir J. 2005;26:1064-8.
- [Google Scholar]
- The role of socioeconomic status gradients in explaining differences in US adolescents’ health. Am J Public Health. 1999;89:1522-8.
- [Google Scholar]
- Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2008;31:143-78.
- [Google Scholar]
- Social classification: the need to update in the present scenario. Indian J Community Med. 2008;33:50-1.
- [Google Scholar]
- American Thoracic Society. Standardization of spirometry, 1994 update. Am J Respir Crit Care Med. 1995;152:1107-36.
- [Google Scholar]
- The level of unmet need & social correlates: An experience from a district in West Bengal. Int J Med Public Health. 2012;2:29-33.
- [Google Scholar]
- Socioeconomic variation in asthma hospitalization: excess utilization or greater need? Pediatrics. 1999;103:e75.
- [Google Scholar]
- Association between income adequacy and asthma in Canadians. Proceedings of Statistics Canada Symposium- Modelling Survey Data for Social and Economic Research; 2002.
- [Google Scholar]
- Effect of area of residence on patterns of aeroallergen sensitization in atopic patients. Am J Rhinol Allergy. 2010;24:98-103.
- [Google Scholar]
- Inheritance patterns, consanguinity & risk for asthma. Indian J Med Res. 2010;132:48-55.
- [Google Scholar]
- Environmental factors and gene-environment interactions in the aetiology of asthma. Clin Exp Pharmacol Physiol. 2006;33:285-9.
- [Google Scholar]
- Asthma and pregnancy: emerging evidence of epigenetic interactions in utero. Curr Opin Allergy Clin Immunol. 2009;9:417-26.
- [Google Scholar]
- Effect of cat and dog ownership on sensitization and development of asthma among preteenage children. Am J Respir Crit Care Med. 2002;166:696-702.
- [Google Scholar]
- The effect of neonatal BCG vaccination on atopy and asthma at age 7 to 14 years: an historical cohort study in a community with a very low prevalence of tuberculosis infection and a high prevalence of atopic disease. J Allergy Clin Immunol. 2003;111:541-9.
- [Google Scholar]
- Wheezing and bronchial hyper-responsiveness in early childhood as predictors of newly diagnosed asthma in early adulthood: a longitudinal birth-cohort study. Lancet. 2008;372:1058-64.
- [Google Scholar]




