
Translate this page into:
Association of ankyrin repeats & kinase domain containing 1 (ANKK1) gene polymorphism with co-morbid alcohol & nicotine dependence: A pilot study from a tertiary care treatment centre in north India
Reprint requests: Dr Rizwana Quraishi, Department of Psychiatry, National Drug Dependence Treatment Centre, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110 029, India e-mail: rizwanaquraishi@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
The frequently encountered co-morbidity of alcohol dependence (AD) with nicotine dependence (ND) increases the risk for various diseases. Ankyrin repeats and kinase domain containing 1 (ANKK1) gene polymorphism is reported to be associated with both ND and AD. This study was undertaken to investigate the possible association of alcohol and tobacco use variables with ANKK1 polymorphism in co-morbid alcohol- and nicotine-dependent treatment seekers visiting a tertiary care centre in north India.
Methods:
Seventy nine male participants (18-65 yr old) fulfilling diagnostic criteria for ND and AD were included in the study. The socio-demographic data, along with alcohol and tobacco use profile, was recorded and ANKK1 profiling was carried out. Both the allele groups, A1 and A2, were compared with respect to demographic and substance dependence profile. Univariate binary logistic regression analysis was performed to determine the risk of high nicotine and alcohol consumption with genotype.
Results:
The A1 carrier group (n=33) reported a significantly higher amount of alcohol and tobacco consumed per day. The scores on parameters of ND were found to be significantly higher in this group. The logistic regression analysis revealed that participants with A1 genotype were 2.5 times more likely to report higher amount of alcohol and nicotine consumption than A2 carriers.
Interpretation & conclusions:
The study provides an indication for the association of ANKK1 polymorphism in the form of higher substance consumption among alcohol dependent smokers, who are A1 carriers and thus may require higher attention of the treatment provider.
Keywords
Alcohol and nicotine dependence
ankyrin repeats and kinase domain containing 1 gene polymorphism
treatment seekers

Alcohol and tobacco misuse is listed among the significant risk factors associated with the global burden of disease by the World Health Organization1. Use of tobacco among alcohol dependent people has a major effect on morbidity2. In India, alcohol is the most common substance of use among people seeking treatment for addiction. In a nationwide survey among treatment seekers, around 44 per cent reported alcohol use3.
The development of co-morbid alcohol and nicotine dependence (AD and ND) is a complex phenomenon which is influenced by several psychosocial, environmental and genetic factors. Studies conducted on twins have reported the genetic contribution of AD and ND with an estimated heritability of 50 per cent4. In a large population-based sample of Dutch twins, alcohol use was found to be correlated (r=0.5-0.6) with smoking. Further, alcohol use in one twin was correlated with smoking in the co-twin, suggesting that familial factors contributing to the association between alcohol and tobacco use. With a bivariate genetic model, it was suggested that alcohol and tobacco use in young adults were associated due to the same genetic risk factors5.
The dopaminergic reward system has long been postulated to be involved in the aetiology of dependence to various psychoactive substances including alcohol and nicotine6. The D2 dopamine receptor gene has been studied widely, focusing on Taq A1 polymorphism in the development of AD and ND. It is actually located in a neighbouring noble gene named ankyrin repeats and kinase domain containing 1 (ANKK1) gene located at exon 8, with two alleles designated as A1 and A27. Individuals with at least one A1 allele appear to have up to 40 per cent fewer striatal dopamine D2 receptor (DRD2) relative to A2/A2 allele carrier individuals8.
An association of Taq A1 polymorphism with ND and AD separately has been shown91011, whereas another study found no association by applying random effect model12. A meta-analysis has shown that ethnicity of the individuals alters the effects of DRD2 Taq A1 polymorphism among alcohol- and nicotine-dependent participants13.
A few studies from north India involving dopamine receptor/ANKK1 reported high risk for AD in the A1 allele carriers1415, while a study from south India reported no association in a severely affected alcoholic population with a young age of onset16. The present study was, therefore, conducted to investigate the association of alcohol and tobacco use variables with ANKK1 gene polymorphism in co-morbid alcohol- and nicotine-dependent treatment seekers visiting a tertiary care centre in north India.
Material & Methods
This was a cross-sectional study, conducted over a period of eight months in 2012 at the National Drug Dependence Treatment Centre, (NDDTC), All India Institute of Medical Sciences (AIIMS), New Delhi, India. The study protocol was approved by the Institutional Ethical Committee. A written informed consent was obtained from all the participants. Individuals were included if they were (i) males, in the age-range of 18-65 yr visiting the outpatient clinic for treatment of alcohol use disorders, (ii) fulfilling Diagnostics and Statistical Manual of Mental Disorder, fourth edition17, criteria for ND and AD, (iii) reporting use of minimum 10 cigarettes per day in the past 12 months (based on the self-report), (iv) belonging to northern India, (v) not current poly-substance user, (vi) reporting no major physical or mental health problem, and (vii) willing to provide informed consent to participate in the study. Participants were purposively selected in the study without any specific bias.
Following inclusion, the socio-demographic profile (including age, sex, marital status, employment and education), medical history, smoking history and current smoking behaviour and medical co-morbidity, were recorded.
Tobacco and Alcohol consumption: Information on the average amount of alcohol and tobacco consumed/day was recorded from all the participants. Alcohol use was recorded on the basis of usual amount and type of beverage consumed in millilitres. To transform into standardized measures, the alcohol content was calculated in grams as reported for the popular beverages available in India18. Tobacco use was recorded as the number of cigarettes/beedi or smokeless tobacco pouches consumed per day. Tobacco content in mg was assessed as per the previously reported estimation of nicotine content from the popular Indian tobacco products19. The severity of ND was assessed by the scores on Heaviness of Smoking Index (HSI) and the Fagerström Test for Nicotine Dependence (FTND)20.
Genetic analysis: From each participant, 5 ml of blood sample was collected. The blood samples were stored at -20°C till analysis. Genomic DNA extraction was carried out using the mini blood DNA extraction kit (Qiagen, Valencia, CA, USA). Taq A1 (rs1800497) genotyping was done using polymerase chain reaction (PCR)-restriction fragment length polymorphism (RFLP) approach following previously published method21. The primers used in the study were F:5’CCTTCCTGAGTGTCATCAAC3’ R:5’ACGGCTCCTTGCCCTCTAG3’21 (purchased from Genei Laboratories Pvt Ltd, Bengaluru). The digested PCR products were resolved on 2-3 per cent agrose gel stained with ethidium bromide. Genotype profiles obtained from this were analyzed along with the clinical data obtained from each participant.
Statistical analysis: The data were recorded into a Microsoft Excel spreadsheet and analysis was performed with SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). The ANKK1 genotyping was classified as the presence or absence of A1 allele (A1A1/A1A2 vs. A2A2). Genotypes were tested for Hardy-Weinberg equilibrium using the Chi-square test for differences in the observed and expected frequencies, with one degree of freedom. Demographic and ND profile were examined using independent sample t tests for continuous variables and Chi-square/Fisher's exact tests for categorical variables to assess the difference in the allele (A1 vs. A2). The wild type (A2A2), heterozygous (A1A2) and mutant (A1A1) genotypes for each individual were dichotomized as the presence and absence of A1 allele. The literature is suggestive of the A1 allele carrier individuals to possess greater likelihood for higher nicotine and alcohol consumption and also increased FTND and HSI score2223. Hence to test this hypothesis binary logistic regression analysis was performed taking each of these four variables as a dependent, one at each time. Independent variable considered was allele form (0; A2; 1; A1) where 0 and 1 referred, respectively to reference and risk allelic form. This provided estimates of parameters in terms of unadjusted risk ratio. Continuation with the same pattern of dependent and independent variables, the adjustment with respect to the duration of use provided adjusted risk ratio.
Results
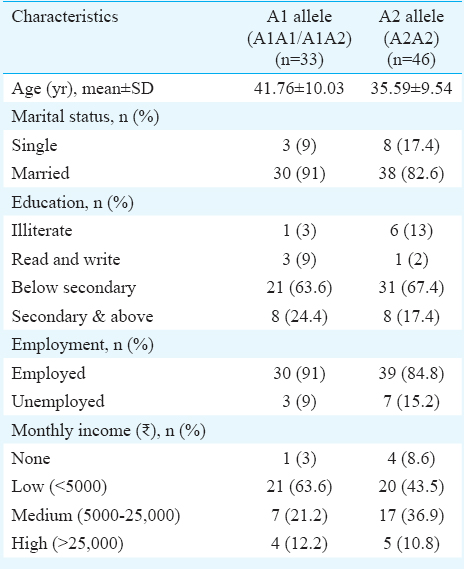
Genotype and demographic profile: A total of 79 alcohol- and nicotine-dependent males were included in the study with mean age of 38.2±10.2 yr (range 20-62 yr). More than one-eighth of the participants were educated below secondary level, married and were employed with income groups varying from low to medium. The Taq A1 genotyping resulted in the presence of A1 allele among 33 (42%) (A1A2=30 and A1A1=3) of the study participants while 46 (58%) had A2A2 genotype. The A1 and A2 allele frequencies were found to be 0.23 and 0.77, respectively. This was found to be in accordance with Hardy-Weinberg equilibrium. The socio-demographic profiling among the two allele type revealed no significant differences (Table I).
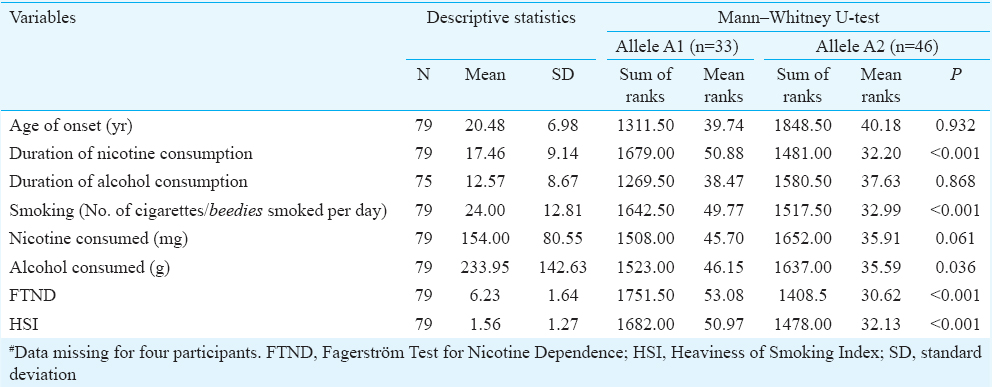
Substance use and dependence measure by ANKK1 genotyping: The alcohol and nicotine use and dependence profile based on the presence or absence of A1 allele is presented in Table II. There was no significant difference in the age of onset of nicotine use, duration of alcohol use from onset till the time of treatment. A significant difference was observed in the smoking duration and number of beedi/cigarettes consumed/day. The mean consumption of cigarette/beedi per day was found to be significantly (P<0.001) higher in an A1 carrier when compared with an A2 group. The mean FTND and HSI scores of the entire sample (n=79) were 6.23 ±1.64 and 1.56 ±1.27, respectively. The HSI score was found to be almost double in the A1 carrier group and was significant (P=0.001). The FTND score was also significantly higher in A1 group (7.2 vs. 5.5; P=0.001).
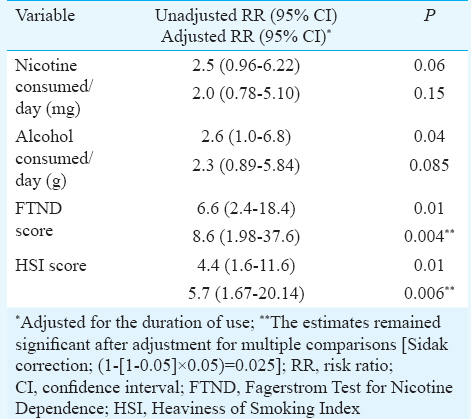
The logistic regression analysis revealed that those with A1 genotype were 2.5 times more likely to report higher amount of alcohol and nicotine consumption than A2 carriers. Further, the analysis identified the A1 carriers to score high on ND scores: FTND and HSI with RR 6.6 (CI 2.4-18.4) and RR 4.4 (CI 1.6-11.6) (Table III).
Discussion
The present study was aimed to test the association of dopamine receptor/ANKK1 polymorphism with co-morbid AD and ND in Indian males who were seeking treatment primarily for alcohol use disorders. Nicotine-dependent smokers are at 2.7 times more risk of becoming alcohol dependent compared to nonsmokers24. Similarly, alcohol-dependent patients are at 4.7 times more risk of smoking than non-alcohol dependent persons25. An association of A1 allele with smoking and alcohol consumption has been suggested independently14 and in combination22.
In the present study, more than 80 per cent of the participants were educated below secondary level and employed with low or medium monthly income. Previous studies from treatment settings reported advancing age, illiteracy and lower socio-economic status as the major factors to be associated with smoking26. The distribution of A1 allele in the present study (23%) was in accordance with earlier Indian studies1415 and also from Egypt23 and studies involving Caucasian populations (18-26%)27.
FTND and HSI are frequently used in genetic studies to measure the severity of physical dependence on nicotine and are found to predict nicotine cessation rate28. These scores are reported to be heritable and linked to specific ND linked genetic variants. In the present study A1 genotype was found to be significantly associated with high ND scores (FTND and HSI). Further, the regression analysis identified the A1 carriers to score high on ND scores (FTND and HSI) with RR of 6.6 and 4.4, respectively. These were consistent with the findings of a study, documenting Taq A1 allele to be significantly associated with higher HSI and FTND scores28. We have earlier reported higher scores among adult smokers with increased beedi/cigarette consumption having lower socio-economic status along with co-morbid alcohol use26.
The current study reported higher consumption of alcohol and nicotine among A1 carrier group. The logistic regression analysis revealed A1 carriers to be 2.5 times more likely to report higher amount of alcohol and nicotine consumption than A2 carriers. These results were in concordance with a previous study among treatment-seeking alcoholics who were problem smokers in an Australian population22. The higher scores on measures of substance dependence in the A1 allele carriers can be attributed to the lower availability of dopamine receptor binding sites2223 thereby leading to compensation by increasing consumption in chronic users.
The DRD2 Taq A1 allele, which is implicated in severe substance misuse, is likely to be associated with the reward mechanism1122. This indicates the importance of looking at DRD2 Taq A1 as a general risk for substance misuse rather than for a specific substance. Results of the current study suggest that among A1 carriers, AD with co-morbid ND represents a particularly severe form of the disorder requiring higher attention of the treatment providers.
The present study had certain limitations; the sample size was small as the patients generally do not reveal their tobacco use. The use of tobacco and alcohol consumption was self-reported by the participants and was not verified by any biological marker. Controls were not included. The study included only the treatment seekers at a tertiary care hospital setting and focused on a single gene; hence the findings cannot be generalized.
In conclusion, the study findings showed an association of increased substance consumption along with higher dependence scales with ANKK1 polymorphism in co-morbid alcohol- and nicotine-dependent treatment seekers visiting a tertiary care centre. Owing to the fact that nicotine and alcohol dependence is a complex disorder, future research studies with larger sample size, a variety of behavioural phenotypes and other genes in this population are warranted.
Acknowledgment
Authors acknowledge Prof. R. Ray, Chief, National Drug Dependence Treatment Centre, AIIMS, New Delhi, for his constant support and motivation to carry out this study. The technical support of Shri Ram Kumar is acknowledged.
Conflicts of Interest: None.
References
- Comorbid cigarette and alcohol addiction: Epidemiology and treatment. J Addict Dis. 1998;17:55-66.
- [Google Scholar]
- The extent, pattern and trends of drug abuse in India: National survey. New Delhi: United Nations Office on Drugs and Crimes & Ministry of Social Justice and Empowerment, Government of India; 2004.
- Association between alcohol use and smoking in adolescent and young adult twins: A bivariate genetic analysis. Alcohol Clin Exp Res. 1997;21:537-46.
- [Google Scholar]
- New directions in the genetic mechanisms underlying nicotine addiction. Addict Biol. 2001;6:109-17.
- [Google Scholar]
- Identification and characterization of ANKK1: A novel kinase gene closely linked to DRD2 on chromosome band 11q23.1. Hum Mutat. 2004;23:540-5.
- [Google Scholar]
- Allelic association of the D2 dopamine receptor gene with receptor-binding characteristics in alcoholism. Arch Gen Psychiatry. 1991;48:648-54.
- [Google Scholar]
- Meta-analysis of the association of the Taq1A polymorphism with the risk of alcohol dependency: A HuGE gene-disease association review. Am J Epidemiol. 2008;167:125-38.
- [Google Scholar]
- The taqI DRD2 A1 allele is associated with alcohol-dependence although its effect size is small. Alcohol Alcohol. 2006;41:479-85.
- [Google Scholar]
- Genetic polymorphism and smoking behavior: A systemic review and meta analysis. Nicotine Tob Res. 2004;6:583-97.
- [Google Scholar]
- Family-based study of the association of the dopamine D2 receptor gene (DRD2) with habitual smoking. Am J Med Genet. 2000;90:299-302.
- [Google Scholar]
- Association between dopamine receptor 2 TaqIA polymorphisms and smoking behavior with an influence of ethnicity: A systematic review and meta-analysis update. Nicotine Tob Res. 2013;15:633-42.
- [Google Scholar]
- Dopamine D2 receptor polymorphisms and susceptibility to alcohol dependence in Indian males: A preliminary study. BMC Med Genet. 2010;11:24.
- [Google Scholar]
- DRD2 and ANKK1 gene polymorphisms and alcohol dependence: A case-control study among a Mendelian population of East Asian ancestry. Alcohol Alcohol. 2013;48:409-14.
- [Google Scholar]
- Polymorphisms at the DRD2 locus in early-onset alcohol dependence in the Indian population. Addict Biol. 2001;6:331-5.
- [Google Scholar]
- American Psychiatry Association. In: Diagnostics and statistical manual of mental disorders. Washington, DC: American Psychiatry Press; 1994. p. :4.
- [Google Scholar]
- Country profile on alcohol in India. In: Riley L, Marshall M, eds. Alcohol and public health in 8 developing countries. Geneva: World Health Organization; 1999. p. :37-60.
- [Google Scholar]
- Estimation of nicotine content in popular Indian brands of smoking and chewing tobacco products. Indian J Dent Res. 2008;19:88-91.
- [Google Scholar]
- The Fagerström test for nicotine dependence: A revision of the Fagerström tolerance questionnaire. Br J Addict. 1991;86:1119-27.
- [Google Scholar]
- Heavy nicotine and alcohol use in alcohol dependence is associated with D2 dopamine receptor (DRD2) polymorphism. Addict Behav. 2007;32:310-9.
- [Google Scholar]
- DRD2/ANKK1 TaqI polymorphism and smoking behavior of Egyptian male cigarette smokers. Nicotine Tob Res. 2007;9:1325-9.
- [Google Scholar]
- Psychiatric comorbidity of smoking and nicotine dependence. Behav Genet. 1995;25:95-101.
- [Google Scholar]
- Profile of nicotine use among alcohol dependent patients visiting a tertiary care center in North India. Indian J Psychol Med. 2014;36:174-8.
- [Google Scholar]
- Dopamine receptor DRD2 genotype and smoking cessation outcome following treatment with bupropion SR. Pharmacogenomics J. 2005;5:21-9.
- [Google Scholar]
- Significant association of ANKK1 and detection of a functional polymorphism with nicotine dependence in an African-American sample. Neuropsychopharmacology. 2009;34:319-30.
- [Google Scholar]




