
Translate this page into:
Association of −330 interleukin-2 gene polymorphism with oral cancer
Reprint requests: Dr Girish Chandra, Department of Anaesthesiology, King George's Medical University, Lucknow 226 003, Uttar Pradesh, India e-mail: girishkgmu123@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Cytokines play an important role in the development of cancer. Several single-nucleotide polymorphisms (SNPs) of cytokine genes have been reported to be associated with the development and severity of inflammatory diseases and cancer predisposition. This study was undertaken to evaluate a possible association of interleukin 2 (IL-2) (− 330A>C) gene polymorphisms with the susceptibility to oral cancer.
Methods:
The SNP in IL-2 (−330A>C) gene was genotyped in 300 oral cancer patients and in similar number of healthy volunteers by polymerase chain reaction (PCR)-restriction fragment length polymorphism and the association of the gene with the disease was evaluated.
Results:
IL-2 (−330A>C) gene polymorphism was significantly associated with oral cancer whereas it was neither associated with clinicopathological status nor with cancer pain. The AC heterozygous genotype was significantly associated with oral cancer patients as compared to controls [odds ratio (OR): 3.0; confidence interval (CI): 2.14-4.20; P<0.001]. The C allele frequency was also significantly associated with oral cancer (OR: 1.80; CI: 1.39-2.33; P<0.001). IL-2 (−330A>C) gene polymorphism was also associated with oral cancer in tobacco smokers and chewers.
Interpretation & conclusions:
Our results showed that oral cancer patients had significantly higher frequency of AA genotype but significantly lower frequency of AC genotype and C allele compared to controls. The IL-2 AC genotype and C allele of IL-2 (−330A>C) gene polymorphisms could be potential protective factors and might reduce the risk of oral cancer in Indian population.
Keywords
Cancer pain
inflammation
interleukin-2
oral cancer
single-nucleotide polymorphism

Oral cancer is the eighth most frequent cancer worldwide1. Of all the annually diagnosed cancer patients, approximately 20-30 per cent suffer from oral cancer. It is one of the most common malignancies among Indian males2. In India, oral cancer is one of the major causes of cancer-related deaths1. Oral cancer includes all malignancies originating in the region of head and neck and has a high incidence, with a poor prognosis34. This may be due to the absence of effective diagnostic and prognostic methods which can guide suitable management at early stages. Oral cancer pain directly affects patients’ quality of life, daily activities, eating, speech and psychological status5. Significant pain has been reported in up to 25 per cent of patients undergoing active treatment and in up to 90 per cent of patients with progressive cancer6. Pain in oral cancer is multifactorial, encompassing a variety of phenotypes. Each phenotype is a result of an underlying oral disease and superimposing environmental factors, such as tobacco chewing, smoking, alcohol consumption and genetic factors7. Cytokines are small glycoproteins released by many different cell types which play a complex role in cancer immunity and carcinogenesis8. Several pro-inflammatory cytokine gene products have been recognized that mediate a critical role in the suppression of apoptosis, proliferation, angiogenesis, invasion and metastasis. Some previous studies have suggested that the common polymorphisms in angiogenesis, thrombosis and inflammation-related genes are associated with increased risk for oral cancer and cancer-related pain9101112.
Interleukin 2 (IL-2), a 15-kDa α-helical cytokine of the Th1 type produced by activated T-cells, promotes the proliferation of lymphocytes, natural killer (NK) cells and macrophages13. IL-2 effectively regulates the immune response and plays important roles in the differentiation of CD41-positive T-cells into Th1 and Th2 effector subsets, while inhibiting T-helper 17 differentiation14. IL-2 is located on chromosome 4q26-q27 and has two single-nucleotide polymorphisms at − 330 and -384 promoter regions, which affect IL-2 expression15. The production of IL-2 protein was greater in CC genotype of IL-2 (−330 A>C) as compared to the AA and AC genotypes in healthy individuals16. Several studies have reported that the IL-2 (−330) gene polymorphism is significantly associated with various cancers, such as peptic ulcer or gastric cancer1718. Cytokines also play an important role in the pathogenesis of cancer-related pain. Cytokines are released by activated glial cells in response to any inflammatory process or tissue damage (as in cancer). These cytokines alter the perception of cancer pain, either by the changed activity of nociceptors or due to hyperexcitability of pain-transmitting neurons12. The present study was carried out to investigate the role of IL-2 (− A330C) genetic polymorphism (rs 2069762) in the pathogenesis of oral cancer in patients attending a tertiary care hospital in north India.
Material & Methods
Study design
Patient selection and clinical evaluation: This population-based case-control study was conducted in the department of Anaesthesiology, King George's Medical University (KGMU), Lucknow, India. The sample size was calculated with 80 per cent of power using the n-Masters 1.0 sample size calculation software developed by Christian Medical College, Vellore, Tamil Nadu, India19. Three hundred oral cancer patients and similar number of healthy volunteers were included in this study, on the basis of well-defined inclusion and exclusion criteria. The histopathologically confirmed oral cancer patients were included in the case group, at the time of baseline treatment from the department of Surgical Oncology of KGMU, Lucknow, between December 2013 and July 2015. The healthy volunteers (controls) comprised those who visited KGMU outdoor clinic as patients to different departments for minor trauma or health check-up, teaching/non-teaching staff and self-willing persons. The participants with a past positive history of any type of cancer or with oral lesions were excluded from the study. Ethical clearance was obtained from the Institutional Ethical Committee. Informed written consent was obtained from all the participants.
Collection of socio-demographic and clinical data: Clinical information, including age, sex, tobacco chewing, smoking, alcohol consumption and disease status, was obtained from patients’ medical records. Oral cancer patients were categorized on the basis of TNM (tumour node metastasis) staging into low risk group (stage I+II, N0 and M0) and high-risk group (stage III+IV, N1+N2 and M1). Clinical data as well as a history of comorbid conditions (heart disease, diabetes, stroke, kidney disease and liver disease) and stage of oral cancer were also extracted from the patients’ records. Self-reported pain ‘during the past week’ was assessed using an 11-point numeric scale (0, ‘no pain’ and 10, ‘worst pain or earlier’-), and a visual analogue scale was used for pain scores20.
Sample collection and molecular analyses: Blood samples (5 ml) were collected in ethylene diamine tetraacetic acid (EDTA) tubes and stored at –80°C until DNA extraction. High molecular weight DNA was extracted using high salting-out method21.
PCR-RFLP analysis of interleukin 2 (−330A>C) gene polymorphism: The final volume of the PCR reaction mixture included 25 μl volume containing 40 ng genomic DNA, 10 pico mole each of forward and reverse primers (F -5’--TAT TCA CAT GTT CAG TGT AGT TCT-3’ and R -5’--CTC TTT GTT ACA TTA GCC CA-3’-) at a concentration of 1×, 1× PCR master mixture (Applied Biosystems, USA). The cycling conditions were as follows: an initial denaturation at 95°C for 4 min, followed by 35 cycles at 95°C for 30 sec, 60°C for 30 sec and 72°C for 40 sec, with a final extension step of 7 min at 72°C in the last cycle. The human β-globin was used as positive control during PCR amplification in genotyping. The PCR products were digested at 37°C with MaeI restriction enzyme to detect the IL-2 alleles and then subjected to three per cent agarose gel electrophoresis (Bio-Rad, USA). Three genotypes were found in our study: genotype A/A, with one fragment, 159 bp; genotype A/C, with two fragments, 159 and 136 bp; and genotype C/C, with one fragments, 136 bp (Figure).
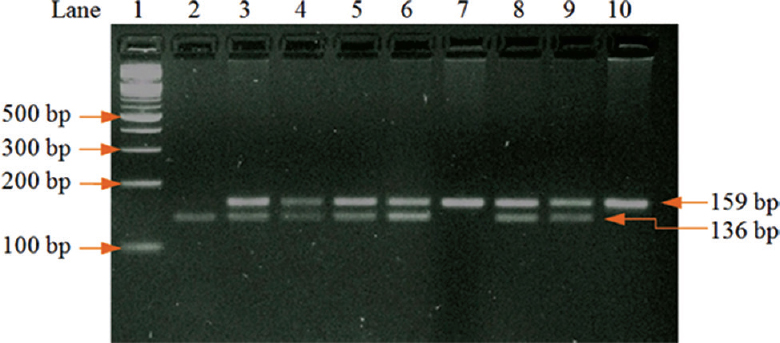
- Gel picture showing the polymerase chain reaction-restriction fragment length polymorphism analysis; after digestion of PCR product with MaeI restriction enzymes (lane 1: 100 bp ladder; lane 2: CC homozygous genotype; lane 3, 4, 5, 6, 8, 9: heterozygous AC genotype; lane 7, 10: homozygous AA genotype.
Statistical analysis: The Chi-square test was used to compare the dichotomous/categorical variables. The unpaired Student's t test was used to compare discrete variables between oral cancer patients and controls. Allele and genotype frequencies were analyzed by Chi-square test and Fisher's exact test. The odds ratios (OR) with 95 per cent confidence interval (CI) were calculated to estimate the strength of association between IL-2 (−330A>C) gene polymorphisms and oral cancer.
Results
The demographic profile included age, gender, body mass index (BMI), relative environmental risk factors and tumour staging. In this study, the age of the participants (47.67±12.67 and 43.03±8.49 yr) was significantly different between oral cancer patients and controls, respectively. However, BMI in the two groups was similar (Table I). The influence of tobacco smoking, chewing and alcohol consumption was also monitored in oral cancer patients and controls, as shown in Table I. The tobacco smoking and chewing were significantly associated with oral cancer. Frequency of smoking was significantly different between oral cancer patients and controls. Alcohol consumption was not significantly different in oral cancer patients and controls. Distribution of oral cancers according to the positions viz. buccal mucosa (44%), tongue (27%), alveolar ridge (13%), lip and gingivobuccal sulcus (5%), hard pallet, retromolar trigone and others (2%) was also observed.
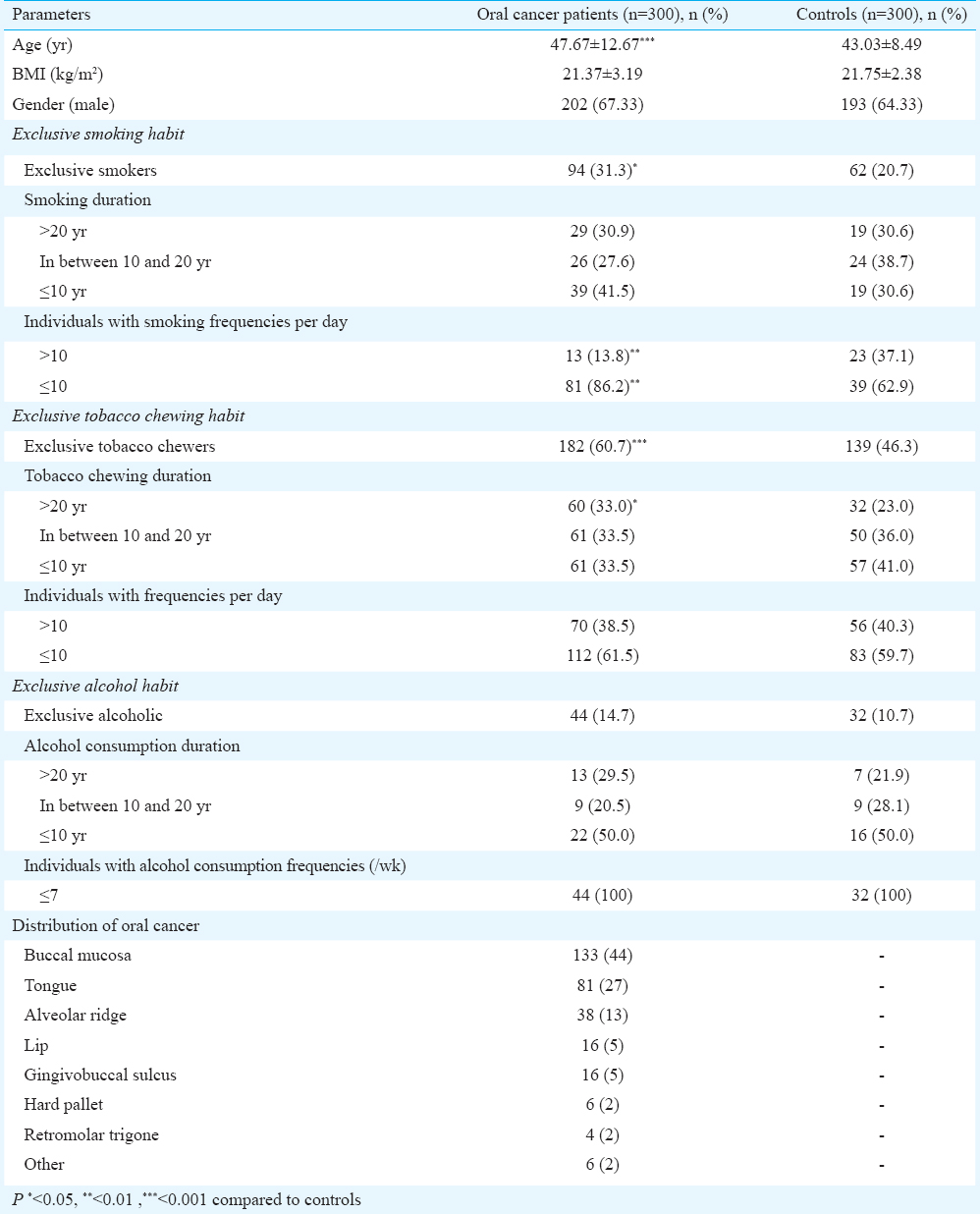
The occurrence of tumour Stages I, II, III and IV was 8, 56.3, 33.3 and 2.3 per cent, respectively. Lymph node status (N0: 70.7%, N1+N2: 29.3%) and metastasis (M0: 98.7%, M1: 1.3%) were also analyzed. The occurrence of pain according to tumour Stages I, II, III and IV was 37.5, 40.2, 43.0 and 71.4 per cent, respectively. Severity of oral cancer pain according to stage was: Stage I (mild: 50%, moderate: 50% and severe pain: 0%), Stage II (mild: 22.1%, moderate: 73.5% and severe pain: 4.4%), Stage III (mild: 25.6%, moderate: 65.1% and severe pain: 9.3%) and Stage IV (mild: 20%, moderate: 40% and severe pain: 40%).
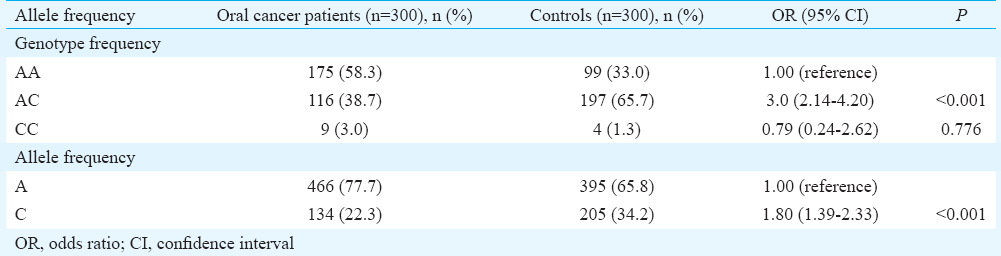
The distribution of genotype and allele at locus was compared between oral cancer patients and controls. The frequencies of the AA, AC and CC genotypes of IL-2 (−330A>C) were 58.3, 38.7 and 3.0 per cent in cases and 33.0, 65.7 and 1.3 per cent in controls, respectively, whereas the allele frequencies of A and C were found to be 77.7 and 22.3 per cent of the study cases and 65.8 and 34.2 per cent in controls, respectively. There were significant differences in the homozygous AA and AC genotype frequencies of the IL-2 (−330A>C) gene polymorphism between oral cancer patients and controls (OR: 3.0; CI: 2.14-4.20; P<0.001), whereas homozygous AA and homozygous CC genotypes did not show any significant difference between the groups. Alleles A and C were also significantly (OR: 1.80; CI: 1.39-2.33; P<0.001) associated with oral cancer (Table II).
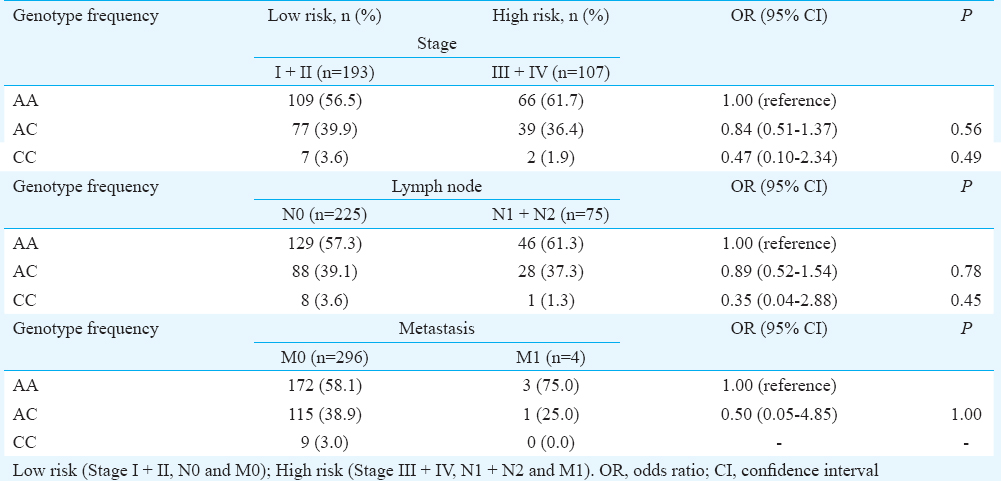
Oral cancer patients were categorized into two groups: low risk and high risk. Low-risk group patients had Stage I+II, N0 and M0 and high-risk group had Stage III+IV, N1+N2 and M1. There was no significant difference between the genotype distribution of the IL-2 (−330A>C) gene polymorphism and tumour stage, lymph node status and metastasis between these two groups (Table III).
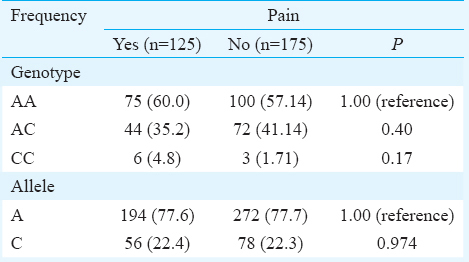
The frequencies of AA, AC and CC genotypes of IL-2 (−330A>C) were 60.0, 35.2 and 4.8 per cent in oral cancer patients with pain and 57.14, 41.14 and 1.72 per cent in oral cancer patients without pain. However, frequencies of A and C alleles were 77.6 and 22.4 per cent in oral cancer patients with pain and 77.7 and 22.3 per cent in oral cancer patients without pain. The frequencies of AA, AC and CC genotypes and A and C alleles of the IL-2 (−330A>C) were not significantly associated with oral cancer pain (Table IV).
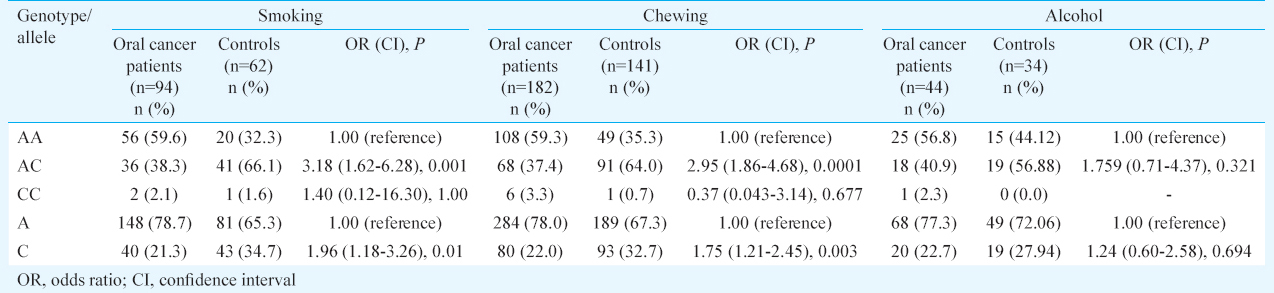
Associations between IL-2 (−330A>C) promoter region genetic variations and exposure to related environmental factors on oral cancer susceptibility are shown in Table V. There were significant differences in the homozygous AA and heterozygous AC genotype frequencies of the IL-2 (−330A>C) gene polymorphism between oral cancer patients and controls, who were known smokers [OR: 3.18 (1.62-6.28); P<0.001] and in tobacco chewers [OR: 2.95 (1.86-4.68); P<0.001]. Allele frequencies of A and C were significantly different in smoking (OR: 1.96; CI: 1.18-3.26; P=0.01) and tobacco chewing individuals (OR:1.75; CI: 1.21-2.45; P=0.003) among oral cancer patients and controls. The frequencies of AA, AC and CC genotypes and A and C alleles of the IL-2 (−330A>C) were not significantly associated with alcohol consumption in oral cancer patients and controls (Table V).
Discussion
Pro-inflammatory cytokines play a significant role in the pathogenesis of a tumour15. Genetic modification also plays a significant role in the inflammatory response, which may be a contributory factor in the risk of oral cancer15. IL-2 is an immune regulatory cytokine with biological functions of pro- and anti-inflammation. It has been demonstrated that IL-2 influences the T-cell proliferation, differentiation and survival of effectors22. An increasing number of evidences indicate that IL-2 may affect the development and the destructive biological nature of different tumors23.
In the current study, we investigated the role of IL-2 (−330A>C) polymorphisms in susceptibility to oral cancer in Indian population and observed that the IL-2 (−330A>C) gene polymorphism could be an anti-tumour factor for oral cancer.
Our results showed that oral cancer patients had a significantly higher frequency of AA genotype, as compared to control group. On the other hand, the frequencies of C allele and heterozygous AC genotype of IL-2 (−330A>C) were significantly lower in oral cancer patients as compared to controls. A previous study has reported that tumour growth is associated with a downregulation of Th1-type activity and upregulation of Th2-type activity. IL-2 is an important inflammatory cytokine which is produced by helper T-cells and activated natural killer (NK) cells and cytotoxic T-cells23. Furthermore, IL-2 also influences the role of cytotoxic T-cells, induced by IL-2 receptor expression, endorsing cell migration, improving the interaction between the cells and inducing cytokine secretion23. Pei et al24 demonstrated that the abnormal level of IL-2 was significantly associated with tumour. Other groups2325 found that the IL-2 (−330) promoter region gene polymorphism was a risk factor and a prognostic marker for cancer development. Some studies have reported the IL-2 gene polymorphism to be associated with decreased expression of IL-2 gene1726. Shin et al27 did not find any significant association between IL-2 genetic polymorphism and gastric cancer. In our study also no association was found between IL-2 (−330A>C) gene polymorphism and progression of oral cancer. Similarly, Savage et al18 also showed no significant association of IL-2 gene polymorphism with the progression of gastric cancer.
The actual molecular mechanism, by which cytokines influence pain, has not yet been established. In our study, the genotype of IL-2 was not significantly associated with oral cancer pain; however, some studies suggested that cytokines released during tissue damage or inflammation change the activity of nociceptors, contributing to pain hypersensitivity28. IL-2 levels have been implicated in pain response28 and in complex regional pain syndrome29. Our study also showed that the oral cancer pain severity increased with increasing tumour stages. There was a strong association of AC genotype and C allele of IL-2 (−330A>C) with oral cancer and tobacco use (smoking and chewing) in our study. Seyedroudbari and Khan30 have also reported that the smokeless tobacco upregulates pro-inflammatory cytokines.
In conclusion, the AC genotype and C allele of IL-2 (−330A>C) gene polymorphisms were significantly different among oral cancer patients and controls. The AC genotype and C allele of IL-2 (−330A>C) might be protective factors against the promotion of oral cancer. Our results did not show any significant association between IL-2 (−330A>C) gene polymorphisms with progression of oral cancer or its associated pain. Further studies with large sample sizes will be necessary to confirm our findings.
Acknowledgment
This work was financially supported by a grant from the Indian Council of Medical Research, New Delhi, India (No: 3/2/2/131/2012/NCD-III).
Conflicts of Interest: None.
References
- Strengthening the prevention of oral cancer: The WHO perspective. Community Dent Oral Epidemiol. 2005;33:397-9.
- [Google Scholar]
- Fas receptor (CD95) & Fas ligand (CD178) expression in patients with tobacco-related intraoral squamous cell carcinoma. Indian J Med Res. 2011;134:54-60.
- [Google Scholar]
- Second primary tumors in head and neck cancer. Acta Otorrinolaringol Esp. 2006;57:462-6.
- [Google Scholar]
- Interleukin-18: Biology and role in the immunotherapy of cancer. Curr Med Chem. 2010;17:3353-7.
- [Google Scholar]
- Pain and its treatment in outpatients with metastatic cancer. N Engl J Med. 1994;330:592-6.
- [Google Scholar]
- Smoking, alcohol, and betel quid and oral cancer: A prospective cohort study. J Oncol. 2011;2011:525976.
- [Google Scholar]
- Cancer mortality in India: A nationally representative survey. Lancet. 2012;379:1807-16.
- [Google Scholar]
- Targeting the interleukin-6/Jak/stat pathway in human malignancies. J Clin Oncol. 2012;30:1005-14.
- [Google Scholar]
- Genetic and nongenetic covariates of pain severity in patients with adenocarcinoma of the pancreas: Assessing the influence of cytokine genes. J Pain Symptom Manage. 2009;38:894-902.
- [Google Scholar]
- Th1 and Th2 cytokine profiles in recurrent aborters with successful pregnancy and with subsequent abortions. Hum Reprod. 2001;16:2219-26.
- [Google Scholar]
- Interleukin-2 signaling via STAT5 constrains T helper 17 cell generation. Immunity. 2007;26:371-81.
- [Google Scholar]
- Two novel biallelic polymorphisms in the IL-2 gene. Eur J Immunogenet. 1998;25:419-20.
- [Google Scholar]
- Association of cytokine polymorphic inheritance and in vitro cytokine production in anti-CD3/CD28-stimulated peripheral blood lymphocytes. Transplantation. 2001;72:1444-50.
- [Google Scholar]
- Promoter polymorphisms of IL2, IL4, and risk of gastric cancer in a high-risk Chinese population. Mol Carcinog. 2009;48:626-32.
- [Google Scholar]
- Polymorphisms in interleukin -2, -6, and -10 are not associated with gastric cardia or esophageal cancer in a high-risk Chinese population. Cancer Epidemiol Biomarkers Prev. 2004;13:1547-9.
- [Google Scholar]
- Methods of determining sample sizes in clinical trials. Indian Pediatr. 1989;26:115-21.
- [Google Scholar]
- A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 1988;16:1215.
- [Google Scholar]
- The association of −330 interleukin-2 gene polymorphism with its plasma concentration in Iranian multiple sclerosis patients. Scientifica (Cairo). 2014;2014:724653.
- [Google Scholar]
- Interleukin-2 gene polymorphisms and prognosis of breast cancer. Genet Test Mol Biomarkers. 2013;17:453-7.
- [Google Scholar]
- A variant in interleukin-2 gene is associated with repeated spontaneous abortion in Ningxia Han people. Open J Obstet Gynecol. 2013;3:32-6.
- [Google Scholar]
- IL-2 gene C/T polymorphism is associated with prostate cancer. J Clin Lab Anal. 2006;20:245-9.
- [Google Scholar]
- Effects of the multiple sclerosis associated −330 promoter polymorphism in IL2 allelic expression. J Neuroimmunol. 2004;148:212-7.
- [Google Scholar]
- Polymorphisms of interleukin-1 and interleukin-2 genes in patients with gastric cancer in Korea. J Gastroenterol Hepatol. 2008;23:1567-73.
- [Google Scholar]
- Expression of interleukin 8 and its receptors in human colon carcinoma cells with different metastatic potentials. Clin Cancer Res. 2001;7:3298-304.
- [Google Scholar]
- Differential expression patterns of cytokines in complex regional pain syndrome. Pain. 2007;132:195-205.
- [Google Scholar]
- In vitro effects of smokeless tobacco extract on tumor necrosis factor-alpha (TNF-alpha) and interleukin-1beta (IL-1beta) production, and on lymphocyte proliferation. Toxicon. 1998;36:631-7.
- [Google Scholar]




