
Translate this page into:
Association between anthropometry, cardiometabolic risk factors, & early life factors & adult measures of endothelial function: Results from the New Delhi Birth Cohort
Reprint requests: Dr Mark D. Huffman, Department of Preventive Medicine, Northwestern University Feinberg School of Medicine, 680 N. Lake Shore Drive, Suite 1400, Chicago, IL 60660, USA e-mail: m-huffman@northwestern.edu
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Abnormal endothelial function represents a preclinical marker of atherosclerosis. This study was conducted to evaluate associations between anthropometry, cardiometabolic risk factors, and early life factors and adult measures of endothelial function in a young urban Indian cohort free of clinical cardiovascular disease.
Methods:
Absolute changes in brachial artery diameter following cuff inflation and sublingual nitroglycerin (400 µg) were recorded to evaluate endothelium-dependent and -independent measures of endothelial function in 600 participants (362 men; 238 women) from the New Delhi Birth Cohort (2006-2009). Data on anthropometry, cardiometabolic risk factors, medical history, socio-economic position, and lifestyle habits were collected. Height and weight were recorded at birth, two and 11 yr of age. Age- and sex-adjusted linear regression models were developed to evaluate these associations.
Results:
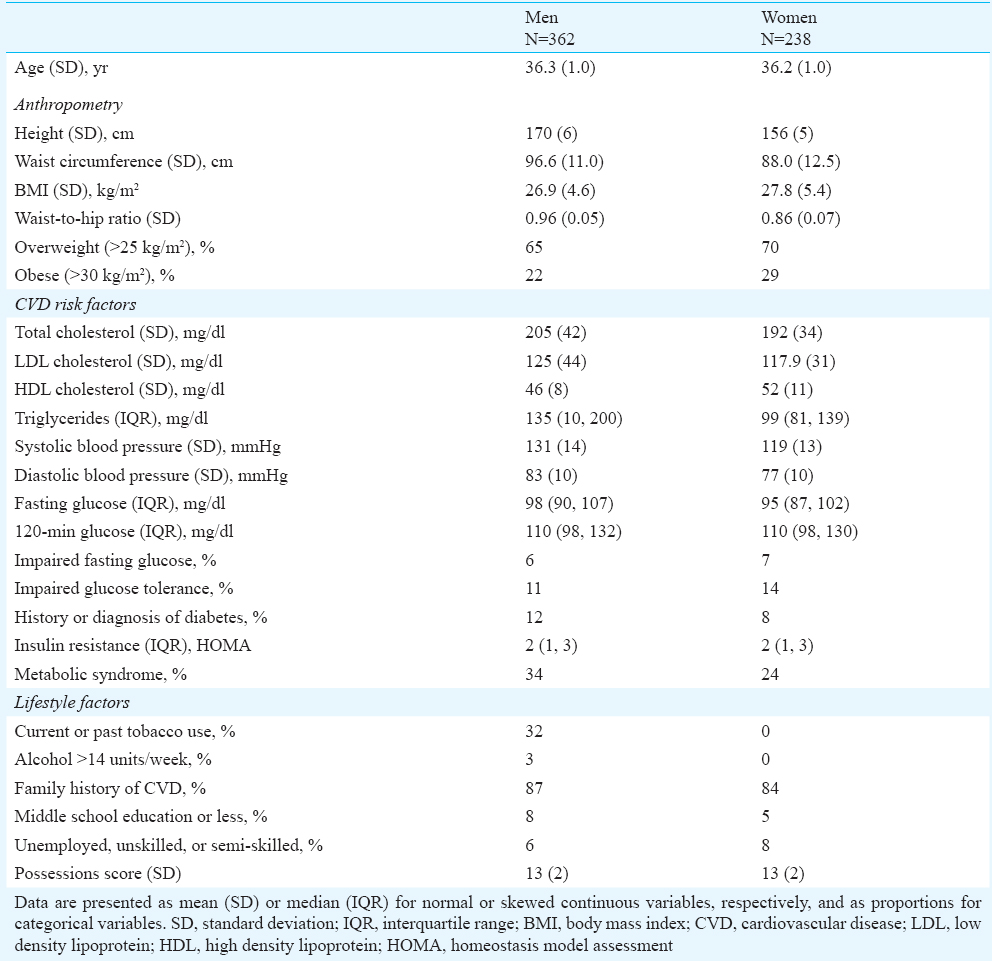
The mean age of participants was 36±1 yr. Twenty two per cent men and 29 per cent women were obese (BMI > 30 kg/m2). Mean systolic blood pressure (SBP) was 131±14 and 119±13 mmHg, and diabetes prevalence was 12 and 8 per cent for men and women, respectively. Brachial artery diameter was higher for men compared with women both before (3.48±0.37 and 2.95±0.35 cm) and after hyperaemia (3.87±0.37 vs. 3.37±0.35 cm). A similar difference was seen before and after nitroglycerin. Markers of increased adiposity, smoking, SBP, and metabolic syndrome, but not early life anthropometry, were inversely associated with endothelial function after adjustment for age and sex.
Interpretation & conclusions:
The analysis of the current prospective data from a young urban Indian cohort showed that cardiometabolic risk factors, but not early life anthropometry, were associated with worse endothelial function.
Keywords
Anthropometry
birth cohort
cardiometabolic risk factors
endothelial functions
flow mediated dilatation
insulin sensitivity

Abnormal endothelial function represents a preclinical marker of atherosclerosis. Though the relationships between low birth weight and early life growth and cardiometabolic diseases, including hypertension1, diabetes2, and ischaemic heart disease3 appear robust, previous research evaluating the association between birth weight and endothelial function appears inconsistent. Norman in a systematic review demonstrated an association in half of the 20 included studies of 1,500 participants4. Ten of these studies were very small (N < 50 participants), none included more than 350 participants, and only one cohort5 was based in a low- or middle-income country (Brazil). In addition, previous studies evaluating the association between cardiometabolic risk factors measured in adulthood and endothelial function have been largely performed in high-income countries.
Therefore, we sought to evaluate the association between anthropometry, cardiometabolic risk factors, and early life factors and adult measures of endothelial function in a large, prospective cohort of young urban Indian adults free of clinical cardiovascular disease (CVD), namely the New Delhi Birth Cohort.
Material & Methods
Study sample: The details of the New Delhi Birth Cohort have been published6. Briefly, between 1969-1972, the original New Delhi Birth Cohort study team recruited 20,755 married women living in a 12 km2 area of New Delhi for participation in a pregnancy outcomes and childhood growth study27. Over this period, there were 9,169 pregnancies and 8,181 live births. Trained study personnel measured the weights and lengths of infants within 72 h of birth and then every six months until 14-21 yr. The All India Institute of Medical Sciences, New Delhi, India, ethics committee approved the study, and all participants provided written informed consent.
Follow up surveys and examinations have occurred over six Phases: Phase 1 (1969-1972), Phase 2 (1973-1980; with interruptions in 1972-1973 and 1980-1982 due to municipal closure of unauthorized housing of some of the study participants), Phases 3 and 4 (1983-1990), Phase 5 (1999-2002), and Phase 6 (August 2006-January 2009). Phases 3 and 4 were combined and lasted for approximately seven years. During this Phase, trained anthropologists recorded anthropometry of the participants at 6-month intervals (±15 days).
At Phase 1, the majority of participants were Hindus (84%), followed by Sikhs (12%), Christians (2%), Muslims (1%) and Jains (1%). Forty three per cent of participants lived in one-room homes, whereas 60 per cent of participants’ families had incomes >50  per month (national mean 28 ), and 15 per cent of parents were illiterate (national mean 66%).
per month (national mean 28 ), and 15 per cent of parents were illiterate (national mean 66%).
Phase 5 follow up (April 1999-August 2002): During 1999 and 2002, a total of 2,584 (32%) participants from the initial birth cohort were successfully contacted after one attempt, and 1,526 (59% of participants contacted, or 19% of the original cohort) agreed to participate. The trained study personnel performed follow up in the participants’ homes where they explained the study procedures, obtained informed consent, and administered surveys to collect information on health behaviours, medical and family history, education, occupation, and household possessions to evaluate socio-economic position as we have previously reported7.
Phase 6 follow up (August 2006-January 2009): The study participants were followed up at a mean (SD) interval of 6.9 (1.0) years after the Phase 5 follow up, including for a repeat of the above investigations. The following algorithm was used to minimize loss to follow up until nearly all non-responders were accounted for: telephone calls/emails, house visits, meeting with neighbours, and contact with local post office. Fifty four (3.5%) participants could not be located, and 18 (1%) had died. Of the surviving participants, 1100 (72% of Phase 5 participants; 13% of the original sample) agreed to participate in Phase 6.
Health behaviours measures included tobacco, physical activity and alcohol. Tobacco was measured by consumption in any form: smoking (cigarettes, bidis, cigars, or hookah), chewing (raw tobacco or with pan), or inhaled (snuff). Physical activity was measured as one of six categories of ‘almost entirely sedentary’ to ‘heavy physical work’. We also measured activities and time performed across domains related to domestic work (e.g. sweeping, washing clothes, cooking), leisure time physical activity (e.g. jogging, swimming, yoga), and transport (walking and cycling, with and without a load). These measures were converted into time estimates, which were multiplied by metabolic constants, derived from the relative energy expenditure of activities8 and summed to derive an activity score, as previously reported7. Alcohol consumption was measured by one of the four categories of none, < 7 units, 7-14 units, and > 14 units/week, with units of alcohol being estimated from the frequency of intake and measure-size of spirits, beer and wine per week (1 unit = 25 ml of spirits, 282 ml of beer, or 125 ml of wine).
Education was measured as one of the seven categories, ranging from no schooling to professional degree. Occupation was measured as one of size categories ranging from unemployed, unskilled manual labour to professional. Women who were housewives were categorized according to their husband's occupation. Household possessions were measured by counting the number of possessions from the following list: electricity, fan, cycle, radio, motorized 2-wheel vehicle, gas stove, television, cable television, electric mixer, electric food grinder (replaced with mobile phone in Phase 6), electric air cooler, washing machine, car, air conditioner, computer, television antenna, and telephone. A global possession score was derived as the first principal component from a correlation matrix of the 17 binary variables and these estimates were compared with national demographic survey data9.
After the home visit, the trained study personnel performed anthropometric measures and phlebotomy using standardized techniques. Blood pressure was measured using an automated device (Omron 711, Bannockburn, IL, USA) with the participants seated after a five-minute rest. The mean of two consecutive blood pressure measurements was recorded. A second blood sample was collected for glucose estimation 120 min after a 75 g oral glucose load. Glucose, cholesterol, and triglyceride concentrations were measured by enzymatic methods using Randox kits (Randox Laboratories Ltd, Crumlin, UK) on a Beckman autoanalyser (Beckman Instruments Inc, Brea, CA, USA), and HDL-cholesterol using the same method after phosphotungstate precipitation. Insulin concentration was measured by radioimmunoassay (Coat-a-Count insulin kit, Diagnostic Products, Los Angeles, CA, USA).
The World Health Organization (WHO) criteria were used to define impaired fasting glucose (IFG), impaired glucose tolerance (IGT) and diabetes10. The National Cholesterol Education Program, Adult Treatment Panel III criteria were used to define metabolic syndrome11. Insulin sensitivity was evaluated according to the homeostasis model assessment (HOMA) and HOMA was taken as a continuous variable12.
Measures of endothelial function: To evaluate endothelial function as a sub-study of the cohort, endothelium-dependent and -independent measures of endothelial function were collected on 600 study participants (362 men; 238 women) out of 631 invited between August 2006 - January 2009 in a fasting, temperature controlled, and supine position. The brachial artery was visualized 5-10 cm above the antecubital fossa in a longitudinal axis using aGE ultrasound machine (Model 5X3; GE Healthcare, Barrington, IL, USA) and a 5 MHz transducer. Five measurements of baseline end-diastolic brachial artery diameter were made from the near-to-far blood-wall interface (intima-media line). To evaluate flow-mediated dilatation (FMD) (a measure of endothelium-dependent endothelial function), a blood pressure cuff was inflated to 300 mmHg for 5 min. Brachial artery diameter was re-measured (5 measurements) one minute after cuff deflation. After five minutes rest, non-endothelium mediated vasodilation was assessed before and five minutes after receiving a single sublingual nitroglycerin (NTG) 400 µg spray (Medley Pharmaceuticals, Ltd., Mumbai, India; 70 µg per metered dose; 200 metered doses per bottle; vehicle included absolute ethanol, peppermint oil).
Exposures: The associations of endothelium-dependent and -independent measures of endothelial function were evaluated with the following exposure variables: age, current body size (Phase 6 BMI, height, waist circumference, waist/hip ratio, obesity and overweight status), current lifestyle [Phase 6 activity, smoking, alcohol, socio-economic status, parity (women)], current CVD risk factors (Phase 6 lipids, blood pressure, glucose tolerance and diabetes/impaired glucose tolerance/impaired fasting glucose), family history, birth weight, size at birth, two years, 11 yr (height, BMI).
Statistical analysis: The mean of each set of five measurements of brachial artery diameter was calculated before and after artery occlusion, and before and after NTG was derived by removing the minimum and maximum values and averaging the remaining three. Changes in endothelial function are generally reported as either absolute change in arterial diameter (post-intervention diameter minus baseline diameter), as percentage change in diameter (post-intervention diameter/minus baseline diameter/baseline diameter x 100), or both. It is well recognized that the percentage change is inversely correlated with baseline arterial diameter, as found here. Therefore, we chose to evaluates absolute change in arterial diameter after hyperaemia, and absolute change in arterial diameter after NTG. These outcome measures were Z-standardized as were exposure variables, where appropriate, to compare effect sizes across parameters.
Multivariable linear regression models were used to evaluate these associations. Phase 6 age and sex were included in all models, and regression models were created with and without adjustment for adult size (waist circumference).We stratified by sex a priori and tested for exposure-outcome interactions by sex. A total of 65 significant sex interaction tests were obtained out of 1,296 individual associations [which is the number expected by chance alone (5%)]. No consistent interaction patterns were found and there was no strong evidence of different relationships between men and women and, therefore, men and women were pooled for our regression modelling.
Results
We compared the characteristics of Phase 5 participants who underwent evaluation of flow-mediated dilatation with participants who did not. The study participants included were minimally older (29.3 vs. 29.1 yr, P=0.01), had achieved a higher level of education (secondary school graduation 63 vs. 53%, P<0.001), had a higher BMI (25.1 vs. 24.6 kg/ m2, P=0.04), and had a greater waist circumference (90.7 vs. 89.9 cm for men; 81.3 vs. 78.6 cm in women, P=0.04) than those not included. These differences in anthropometry were attenuated and no longer significant after adjustment for education level.
During Phase 6, the mean BMI for men and women was 26.9 ± 4.6 and 27.8 ± 5.4 kg/m2, respectively (Table I). The mean total cholesterol was 205 ± 42 and 192 ± 34 mg/dl, and the mean systolic blood pressure was 131 ± 14 and 119 ± 13 mmHg for men and women, respectively. Compared with men, women had higher rates of impaired fasting glucose (7 vs. 6%) and impaired glucose tolerance (14 vs. 11%), but women had lower rates of diabetes (8 vs. 12%), current or past tobacco use (0% vs. 32%), and low levels of education (5 vs. 8%).
During Phase 6, the mean brachial artery diameter was higher for men compared with women both before (3.48 ± 0.37 and 2.95 ± 0.35 cm) and after hyperaemia (3.87 ± 0.37 vs. 3.37 ± 0.35 cm; Table II). A similar difference was seen before and after nitroglycerin. The absolute differences were similar between genders, but the per cent increase was greater in women because of the lower diameters at baseline. The correlation between response to hyperaemia and response to nitroglycerin was weak (r=+0.16).

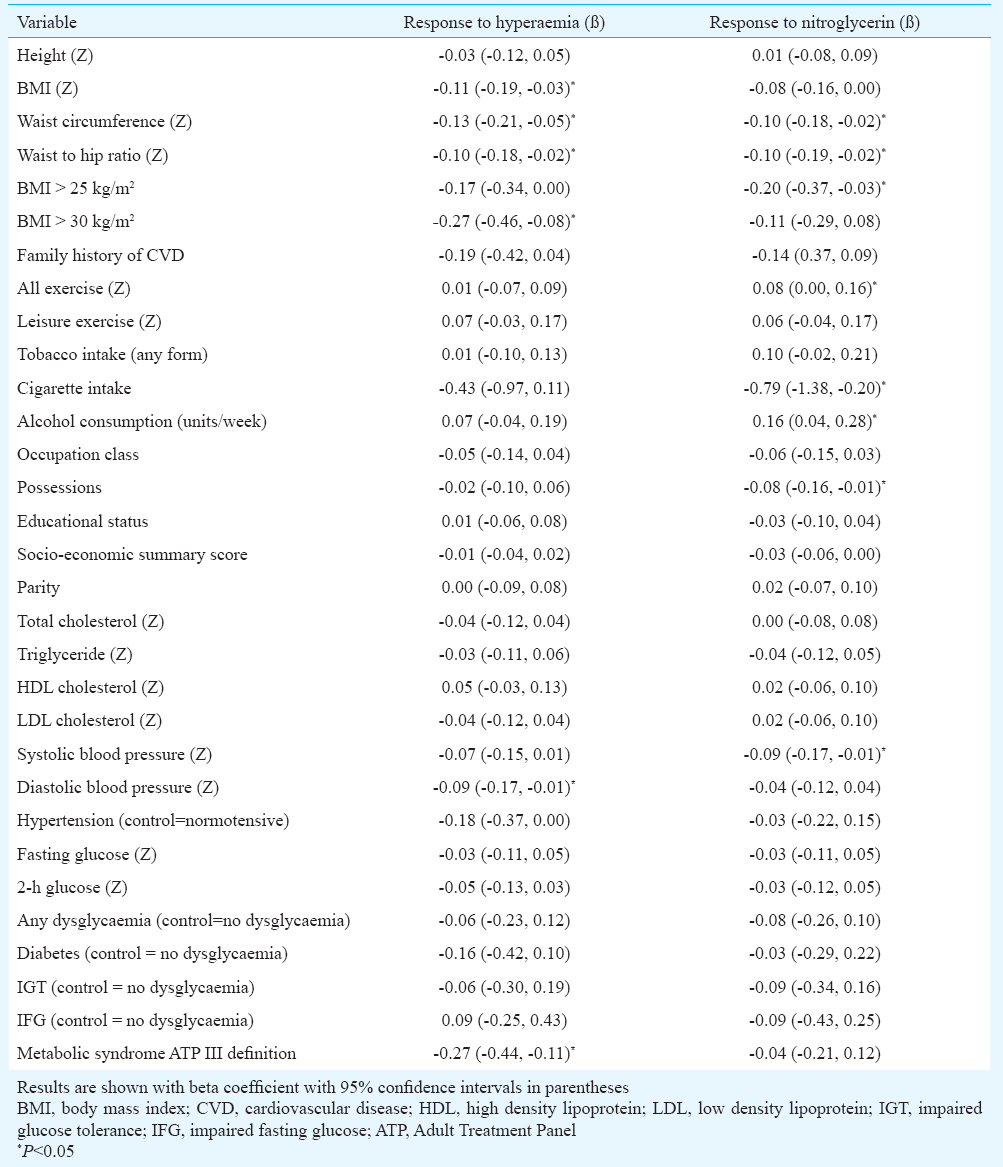
Table III describes the age- and sex-adjusted linear regression models evaluating the associations of anthropometry, lifestyle and behavioural factors, and cardiometabolic risk factors with adult endothelial function, as measured by absolute change in flow mediated dilatation following hyperaemia and/or changes in brachial artery diameter following nitroglycerin. In addition to smoking and systolic blood pressure, markers of increased adiposity were inversely associated with endothelial function. For example, BMI was inversely associated with hyperaemia-induced dilatation [β (95%CI) = -0.11 (-0.19, -0.03)] and with nitroglycerin-induced dilatation [β (95%CI) = -0.08 (-0.16, 0.00)]. The presence of metabolic syndrome was inversely associated with endothelial function measured through hyperaemia [β (95%CI) = -0.27 (-0.44, -0.11)] but not through nitroglycerin [β (95%CI) = -0.04 (-0.21, 0.12)]. Socio-economic position as measured by possessions was inversely associated with dilatation following nitroglycerin but not hyperaemia. The above associations were attenuated but no longer significant after multivariable adjustment for adult size (BMI, height, and waist circumference) but the association between metabolic syndrome and response to hyperaemia remained significant [β (95%CI) = -0.20 (-0.38, -0.02)].
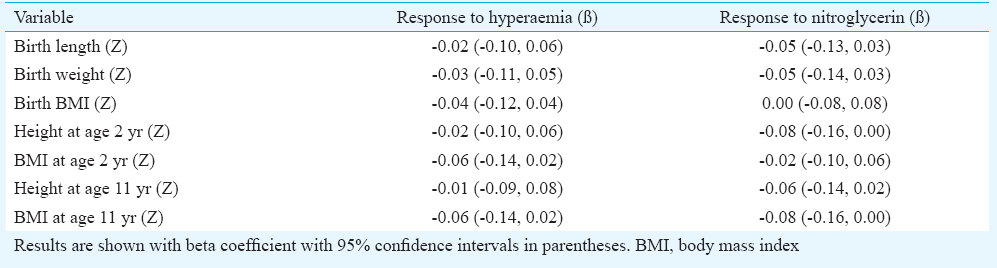
The results of age- and sex-adjusted linear regression models did not demonstrate any associations between early life anthropometry and adult endothelial function (Table IV). Measures of weight and length at birth, height and BMI at two years, and height at 11 yr were unrelated to endothelial function measured by hyperaemia or nitroglycerin. These results remained similar after adjustment for adult body size measures. There was an inverse association of borderline significance, between BMI at 11 yr and nitroglycerin-induced dilatation. This was no longer significant after adjusting for adult body size [β (95%CI) = -0.08 (-0.16, 0.00)].
Discussion
Our data from the New Delhi Birth Cohort showed that among young, urban Indian adults, greater adiposity (BMI, waist circumference, waist/hip ratio and presence of overweight or obesity), higher blood pressure, presence of metabolic syndrome, lower levels of physical exercise, and tobacco use were associated with poorer endothelial function. By contrast, size (weight and length) at birth, and during infancy (2 yr) and childhood (11 yr) were not associated with endothelial function measured in adulthood.
Cardiometabolic risk factors: The data were consistent with prior meta-analytic data from 211 studies13, including results from the Chennai Urban Population Study14, demonstrating associations between cardiometabolic risk factors, particularly diabetes and smoking, and worse endothelial function. However, these associations are limited to individuals with low coronary heart disease risk (<10% 10 year Framingham Risk Score). The New Delhi Birth Cohort has a high burden of cardiometabolic risk factors in the context of early life events, which may increase participants’ risk for CVD events. It has been demonstrated that for every 1 per cent decrease in FMD, there is an approximately 12 per cent increase in CVD events, though these associations have been attenuated when controlling for traditional cardiometabolic risk factors1516. Given these findings, FMD is not indicated for non invasive cardiovascular screening for asymptomatic individuals17.
Birth weight: An association of low birth weight with poor endothelial function has been demonstrated in approximately half of 20 previous studies, almost all from high-income countries, in participants ranging from newborns and children to young adults4. The remainder showed no association between birth weight and endothelial function. In his systematic review, Norman4 was unable to identify reasons for the inconsistent results, although several of the studies that did not show an association had a very small sample size (N<50), and a few or no participants of low birth weight, which would have limited the power of these studies. Suggested mechanisms for the birth weight association include mediation through elevated pro-inflammatory markers such as white blood cell count, fibrinogen, von Willebrand factor, Factor VIII, albumin and activated partial thromboplastin time, which have also been linked to lower birth weight1819, and/or nitric oxide synthesis inhibition20. In animal models it has been shown that undernutrition and high-fat feeding of the pregnant mother led to endothelial dysfunction in the offspring21.
The previous human study most similar to ours was carried out by Leeson et al22 in the UK, among 315 young adults. This showed an inverse association between birth weight and endothelium-dependent flow-mediated dilatation of the brachial artery. The effect was graded across the whole range of birth weight, and similar in magnitude to that seen with smoking. The large sample size in our study, along with a wide range of birth weights, including a high percentage (23%) of low birth weight individuals, means that our study would have been adequately powered to detect such an effect. However, the literature suggests that the association is weak or absent in participants with a greater cardiometabolic risk factor burden23. An interaction by risk factor burden between birth weight and endothelial dysfunction has been demonstrated which suggests that abnormal risk factors may mask the association with birth weight22. The New Delhi Birth Cohort had a relatively high burden of abnormal cardiometabolic risk factors in the fourth decade of life, which might explain why we did not demonstrate an association.
Potential implications: We have previously demonstrated that the individual and collective components of metabolic syndrome are associated with carotid intima-media thickness and carotid plaque but that markers of adult adiposity attenuated these associations6. In our current analysis of FMD, these relationships appear similar, which suggest that strategies to prevent the development of abnormal risk factors in young adulthood, and adiposity in particular, are important to prevent the development of atherosclerosis and to promote normal endothelial function and thus cardiovascular health, even among relatively young individuals. Abnormal FMD has been shown to improve with physical activity24 and drug treatment for hyperlipidaemia2526 and hypertension27, highlighting the reversible nature of impaired FMD.
Strengths of our study include measurement of FMD by a single operator on a prospective, longitudinal community-based cohort study in India with a standardized protocol for measurements of anthropometry by trained staff from early life through young adulthood. Our study also had limitations. First, we included approximately 40 per cent of Phase 5 participants for this sub-study; also, the cohort experienced substantial attrition since its inception (13% of the original cohort participated in Phase 6), which could have led to attrition bias. Participants with FMD measures were modestly older and modestly wealthier than non-participants. Second, we did not evaluate intra-observer variability of FMD measures. Third, while we adjusted for potential confounders that may be associated with our exposures and outcomes, residual confounding may have still been present and have influenced our results. However, the direction of this potential confounding is uncertain. Fourth, while we have evaluated the prospective association between Phase 5 exposures and FMD measured during Phase 6, there is a potential for reverse causality for exposures such as blood pressure, where abnormal FMD may cause higher blood pressures28.
In conclusion, these are perhaps the first prospective data from India showing that cardiometabolic risk factors, but not early life anthropometry, are associated with impaired endothelial function.
References
- Relation of serial changes in childhood body-mass index to impaired glucose tolerance in young adulthood. N Engl J Med. 2004;350:865-75.
- [Google Scholar]
- Trajectories of growth among children who have coronary events as adults. N Engl J Med. 2005;353:1802-9.
- [Google Scholar]
- Low birth weight and the developing vascular tree: a systematic review. Acta Paediatr. 2008;97:1165-72.
- [Google Scholar]
- Effects of low birth weight in 8- to 13-year-old children: implications in endothelial function and uric acid levels. Hypertension. 2006;48:45-50.
- [Google Scholar]
- Predictors of carotid intima-media thickness and carotid plaque in young Indian adults: the New Delhi birth cohort. Int J Cardiol. 2013;167:1322-8.
- [Google Scholar]
- Anthropometric indicators of body composition in young adults: relation to size at birth and serial measurements of body mass index in childhood in the New Delhi birth cohort. Am J Clin Nutr. 2005;82:456-66.
- [Google Scholar]
- Food and Agriculture Organization of the United Nations (FAO). Human energy requirements: report of a Joint FAO/WHO/UNU expert consultation, Rome, 17-24 October 2001. Rome: FAO; 2004.
- [Google Scholar]
- The DHS wealth index. DHS comparative reports 6. Calverton, MD, USA: ORC Macro; 2004.
- [Google Scholar]
- World Health Organization (WHO) In: Definition, diagnosis and classification of diabetes mellitus and its complications report of a WHO consultation. WHO/NCD/NCS/99.2. Geneva: WHO; 1999.
- [Google Scholar]
- Diagnosis and management of the metabolic syndrome. An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Executive summary. Cardiol Rev. 2005;13:322-7.
- [Google Scholar]
- Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia. 1985;28:412-9.
- [Google Scholar]
- Is the association between flow-mediated dilation and cardiovascular risk limited to low-risk populations? J Am Coll Cardiol. 2005;45:1987-93.
- [Google Scholar]
- Comparison of carotid intima-media thickness, arterial stiffness, and brachial artery flow mediated dilatation in diabetic and nondiabetic subjects (The Chennai Urban Population Study [CUPS-9] Am J Cardiol. 2002;90:702-7.
- [Google Scholar]
- Metabolic syndrome, endothelial dysfunction, and risk of cardiovascular events: the Northern Manhattan Study (NOMAS) Am Heart J. 2008;156:405-10.
- [Google Scholar]
- Prognostic role of flow-mediated dilation and cardiac risk factors in post-menopausal women. J Am Coll Cardiol. 2008;51:997-1002.
- [Google Scholar]
- ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2010;122:e584-636.
- [Google Scholar]
- ARIC Investigators. Low birth weight and markers of inflammation and endothelial activation in adulthood: the ARIC study. Int J Cardiol. 2009;134:371-7.
- [Google Scholar]
- Relationship of endothelial function to birth weight in humans. Diabetes Care. 1999;22:2061-6.
- [Google Scholar]
- Could ADMA levels in young adults born preterm predict an early endothelial dysfunction? Int J Cardiol. 2012;159:217-9.
- [Google Scholar]
- Developmental programming of the metabolic syndrome by maternal nutritional imbalance: how strong is the evidence from experimental models in mammals? J Physiol. 2004;561:355-77.
- [Google Scholar]
- Impact of low birth weight and cardiovascular risk factors on endothelial function in early adult life. Circulation. 2001;103:1264-8.
- [Google Scholar]
- Endothelial function is impaired in fit young adults of low birth weight. Cardiovasc Res. 1998;40:600-6.
- [Google Scholar]
- The role of mild systemic heat and physical activity on endothelial function in patients with increased cardiovascular risk: results from a systematic review. Forsch Komplement. 2011;18:24-30.
- [Google Scholar]
- Effect of omega-3 fatty acids supplementation on endothelial function: a meta-analysis of randomized controlled trials. Atherosclerosis. 2012;221:536-43.
- [Google Scholar]
- Meta-analysis of the effects of statin therapy on endothelial function in patients with diabetes mellitus. Atherosclerosis. 2012;223:78-85.
- [Google Scholar]
- Prognostic role of reversible endothelial dysfunction in hypertensive postmenopausal women. J Am Coll Cardiol. 2002;40:505-10.
- [Google Scholar]
- Birth weight relates to blood pressure and microvascular function in normal subjects. J Hypertens. 2000;18:1421-7.
- [Google Scholar]




