
Translate this page into:
Assessment of self-care practices & associated factors among hypertensives in urban slum areas of Mysuru city: A community-based cross-sectional study
For correspondence: Dr Madhu B., Department of Community Medicine, JSS Medical College, JSS Academy of Higher Education & Research, Mysuru 570 015, Karnataka, India e-mail: madhub@jssuni.edu.in
-
Received: ,
Accepted: ,
Abstract
Background & objectives
Hypertension is a significant modifiable risk factor for cardiovascular diseases (CVDs) and premature mortality worldwide, particularly affecting low- and middle- income countries (LMICs). This study focused on evaluating self-care practices among hypertensive affected individuals in urban slum areas of Mysuru city, India, and explore associated factors and their relationship with hypertension control levels.
Methods
A community based cross-sectional study was carried out from March 2022 to August 2023, enrolling 650 hypertensive affected individuals from 63 urban slums of Mysuru city. Data on sociodemographic characteristics, self-care practices, and hypertension control were collected using structured questionnaires and standardized scales. Descriptive statistics and chi-square tests were used for data presentation and analyses.
Results
Among the participants, 62.9 per cent reported poor self-care awareness, and only 37.1 per cent had good self-care awareness. Factors such as age group, education, occupation, type of family, marital status, socioeconomic status, and hypertension control showed significant associations with self-care scores (P≤0.001). However, no significant association was found between gender and self-care scores.
Interpretation & conclusions
This study highlights the critical need for comprehensive interventions integrating self-care awareness into existing health programmes to address the growing burden of hypertension, particularly in urban slum populations. By prioritizing self-care education and empowerment, healthcare stakeholders can equip individuals with the necessary knowledge and skills for effective hypertension management, thus improving health outcomes at individual level and also reducing public health impact of hypertension.
Keywords
Hypertension
self-care behaviour
practice
urban slum population
control level

Worldwide, hypertension or high blood pressure (BP) stands as the primary modifiable risk factor for cardiovascular disease (CVDs) and premature mortality1. In 2019, 10.8 million deaths were attributed to hypertension2. The prevalence of hypertension and the overall burden is substantially increasing, with a staggering 90 per cent rise in the number of individuals worldwide who have high BP, especially in low- and middle-income countries (LMICs). The global rates of treatment, awareness, and control of hypertension are alarmingly inadequate. The global burden of hypertension is anticipated to reach 1.56 billion individuals by the year 2025. It is estimated that two-thirds of this burden will be borne by developing countries3.
In India, hypertension has become the foremost cause of mortality and disability. According to a recent systematic review and meta-analysis by Koya et al4, only 13.2 per cent of hypertensive individuals in India achieved blood pressure control. This rate is notably lower compared to the global average of 21 per cent reported in 2021.
The National Family Health Survey round five (NFHS-5), conducted between 2019 and 2020, reported an increase in the prevalence of hypertension. The survey findings revealed that 24 per cent of men and 21 per cent of women were diagnosed with hypertension4. This represents a notable increase compared to the previous round conducted in 2015-2016, where the prevalence was reported as 17 per cent among men and 19 per cent among women. These rising figures indicate the urgent need for effective interventions and management strategies to address the growing burden of hypertension in India.
The National Non-Communicable Disease (NCD) Monitoring Survey (NNMS) provides evidence of the burden of NCDs and their risk factors in India. The NNMS indicated that only 27.9 per cent of hypertensive individuals were aware of their diagnosis, a figure lower than that reported by NFHS-55. This low awareness underscores the need for better communication between healthcare providers and the general population. Contributing factors to this low awareness include an inadequate emphasis on risk communication in medical education and training, a shortage of counsellors in NCD clinics, and gaps in the training programmes for medical officers. Despite the lower awareness rates, the NNMS reported a higher proportion of participants receiving treatment (14.5% compared to 13.7%) and having their blood pressure under control (12.6% compared to 7.8%) than NFHS-55.
The National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular Diseases, and Stroke (NPCDCS) was launched in 2010 to prevent and control major NCDs6. This initiative emphasizes enhancing health promotion, early diagnosis, and effective management. While the programme currently includes dietary assessment, physical activity evaluation, and screening of behavioural risk factors, integrating a self-care awareness programme for hypertension can significantly enhance its effectiveness.
An estimated one billion people worldwide reside in slums, and projections suggest that this number will double by 2030. In India alone, there are approximately 100,000 slums, housing over 17 per cent of the country’s population. A significant portion of India’s urban population also resides in slums, which are characterized by impoverished socio-environmental conditions. Further, it is important to recognize in this context that the disparities in health outcomes (hypertension and NCD being no exception) between the urban poor and non-poor are a significant concern within the country4. Notably, factors leading to poor hypertension control include limited access to healthcare, insufficient awareness, inadequate treatment, and poor medication adherence. Efforts are therefore essential to enhance the detection, treatment, and control of hypertension in India4,7.
In India, reported hypertension prevalence varies between studies from 10 per cent and 30.9 per cent. Studies conducted in slum areas have reported high prevalence rates of hypertension, ranging from 14 per cent to 26 per cent8-12. Slum dwellers often neglect self-care, rendering them more susceptible to lifestyle-related diseases. Factors such as irregular employment, the constant threat of eviction, overcrowding, alcoholism, and other social challenges contribute to poor health outcomes in slum areas. These circumstances also present challenges in providing adequate health services to these communities13. Hypertension-affected individuals face the challenges of implementing measures at home to ensure effective self-care, and management practices. Adhering to these self-care practices is crucial for successfully managing hypertension and reducing the risk of associated complications14,15.
Self-care has been acknowledged as a significant factor in attaining optimal blood pressure control at the individual level. The World Health Organization (WHO) defines self-care as ‘the ability of individuals, families, and communities to promote health, prevent disease, maintain health, and cope with illness and disability, with or without the support of a healthcare provider.’ This definition highlights the importance of individuals taking an active role in managing their health and well-being16.
In hypertension self-care management, the primary focus should be on two key aspects: medication adherence and lifestyle modifications. By incorporating self-care awareness in hypertension management monitoring, individuals can gain valuable knowledge and skills to better hypertension management. This proactive approach empowers people to understand the importance of self-care practices, such as abstaining from smoking and limiting alcohol consumption, adopting a low-salt diet to reduce sodium intake, aiming for weight reduction in case of overweight or obesity, increasing physical activity levels, practicing self-monitoring to track and manage high BP17. Such integration not only improves individual health outcomes but also strengthens the overall effectiveness of controlling hypertension and reducing related complications.
To address this pressing need for optimal hypertension management in urban slum populations, the present study aimed to assess self-care practices among hypertensive affected individuals in Mysuru city, and identify influencing factors, and investigate their relationship with hypertension status in individuals.
Material & Methods
Study design
A community-based cross-sectional study design was employed. It was carried out during March 2022 to August 2023, from the School of Public Health, JSS Medical College, JSS Academy of Higher Education & Research, Mysuru, Karnataka. The study was conducted in 63 urban slums of Mysuru city after obtaining the ethical approval from the Institutional Ethical Committee. The flow chart of the study is presented in Figure 1.
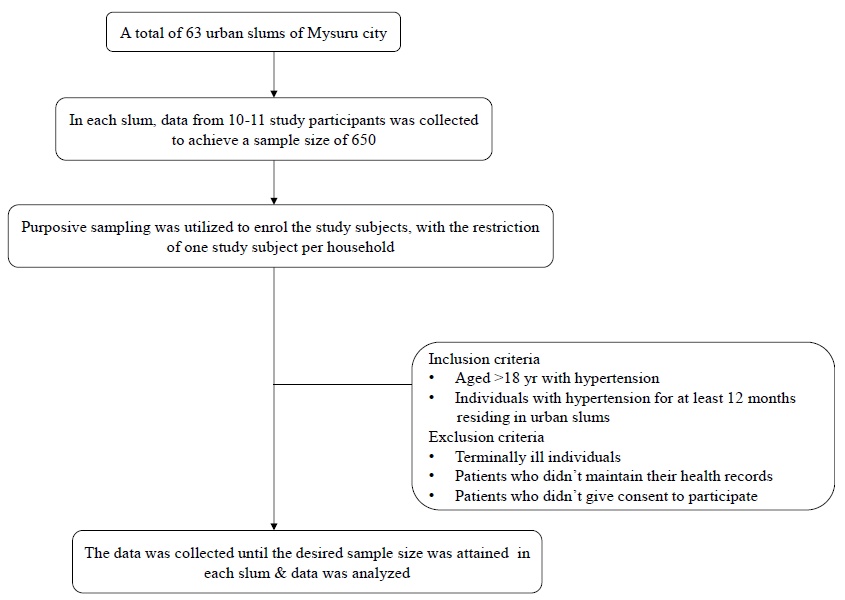
- Flow chart of the study.
Study population and recruitment
The study enrolled hypertensive-affected individuals residing in 63 urban slums of Mysuru city who met the inclusion criteria. The study population included individuals aged ≥18 yr with a confirmed diagnosis of hypertension, residing in urban slums for at least 12 months. Exclusion criteria were established to exclude individuals who were unable to provide informed consent, terminally ill patients, and those not maintaining their health records.
The study utilized a purposive sampling method to enroll the participants. The interviewer cum investigator approached the potential study participants residing in urban slum households who met the inclusion criteria. When multiple hypertensive affected individuals were present in a single household, participants were selected using a lottery method to ensure random selection. Before data collection, all participants provided written informed consent.
Demographic details such as age, gender, body weight, occupation, education, marital status, religion, family type, sociodemographic character, Health insurance, and family history of hypertension were recorded. BP was measured using a sphygmomanometer. The confidentiality and safekeeping of data was ensured.
Sample size calculation
The study enrolled 650 participants to achieve a sample size that allowed for an absolute precision of four per cent at a 95% confidence level (CI), based on a prevalence rate of 44.3 per cent for practicing self-care behaviour18. From each of the 63 slums, 10 to 11 study participants were enrolled.
Study tools
Hypertension Self-Care Profile (HBPSCP): The HBP SCP scale, developed by Han et al19 consists of 20 items measured with each question having five response options: Never = 1, Rarely = 2, Sometimes = 3, Frequently = 4, and Always = 5. This questionnaire assesses self-care awareness among hypertensive patients, with scores ranging from 20 to 100 with higher score indicating better self-care practice. The questions are related to high-salt products being replaced by low-salt products, eating less than one teaspoon of salt per day, eating fruits and vegetables daily and drinking and smoking practices20.
The self-care practice was evaluated using the Hypertensive Self-Care Activity Level Effects (H-SCALE) tool21. The H-SCALE is segmented into six domains: medication adherence, regular blood pressure monitoring, physical activity, low-salt diet, and alcohol consumption, and smoking. Responses of ‘yes’ were interpreted as demonstrating good self-care practices, while ‘no’ responses indicated poor self-care practices. This questionnaire is designed to assess self-care behaviors among hypertensive-affected individuals.
Operational definitions
Low salt diet: ‘A low salt diet is a diet that includes no more than 1,500 to 2,400 mg of sodium per day’.
Hypertension control: ‘Hypertension control is defined clinically as SBP<140 mmHg and DBP<90 mmHg’.
Statistical analysis
The data are presented using descriptive statistics, with categorical variables summarized through frequencies and percentages. To explore the association between sociodemographic characteristics and hypertension self-care scores, we dichotomized the HBP-SCP scores into good (≥ mean) and poor (≤ mean) self-care practices, assessing associations using the Chi-square test or Fisher’s test. A multiple-bar diagram was employed to visualize the self-care practice scores. Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) version 22 (IBM Corp. Armonk, NY, USA) licensed to JSS AHER. A P-value of less than 0.05 was considered significant.
Results
The sociodemographic characteristics of the study participants are presented in Table I. More than half (54.9%) of the study participants were male, and the majority (58.6%) were within 31 to 50 yr age bracket. Approximately 60.8 per cent of them had normal weight, and 75 per cent (75.5%) were employed. Around 44.6 per cent of the study participants were illiterate. The majority (90.3%) were married, and the majority (88%) of the study participants were Hindu. More than half (59.1%) were from a joint family, and ⁓50.6 per cent belonged to the lower class. Around 63.2 per cent had a family history of hypertension, while only 13.1 per cent had health insurance.
| Variable | Category | Frequency | Percentage |
|---|---|---|---|
| Gender | Female | 293 | 45.1 |
| Male | 357 | 54.9 | |
| Age group (yr) | 18-30 | 28 | 4.3 |
| 31-50 | 381 | 58.6 | |
| 51-70 | 212 | 32.6 | |
| >70 | 29 | 4.5 | |
| BMI category | Underweight (<18.5) | 26 | 4 |
| Normal weight (18.5-24.9) | 395 | 60.8 | |
| Overweight (25-29.9) | 182 | 28 | |
| Obese (>30) | 47 | 7.2 | |
| Occupation | Unemployed | 159 | 24.5 |
| Employed | 491 | 75.5 | |
| Education | Illiterate | 290 | 44.6 |
| Schooling | 271 | 41.7 | |
| Degree/Diploma | 89 | 13.7 | |
| Marital status | Married | 587 | 90.3 |
| Unmarried | 33 | 5.1 | |
| Divorced/Widowed | 30 | 4.6 | |
| Religion | Hindu | 572 | 88 |
| Muslim | 52 | 8 | |
| Christian | 21 | 3.2 | |
| Others | 5 | 0.8 | |
| Family type | Joint | 384 | 59.1 |
| Nuclear | 245 | 37.7 | |
| Three generation | 21 | 3.2 | |
| Socioeconomic status | Upper | 5 | 0.8 |
| Upper middle | 57 | 8.8 | |
| Upper lower | 135 | 20.8 | |
| Lower | 329 | 50.6 | |
| Lower middle | 124 | 19.1 | |
| Family history of hypertension | Yes | 411 | 63.2 |
| No | 239 | 36.8 | |
| Insurance | Insured | 85 | 13.1 |
| Uninsured | 565 | 86.9 |
BMI, body mass index
Among the 650 study subjects, 409 (62.9%) individuals reported poor self-care awareness of hypertension, while only 241(37.1%) reported good self-care awareness. Self-care activity level effect (H-scale) is represented in Figure 2. The majority of the participants had awareness about adherence to the medical schedule i.e., 556 (85.5%). More than half of them were unaware of low salt diet intake, i.e., 396 (60.9%). Around 439 (67.5%) were non-smokers. More than half of them were non-alcoholic, i.e., 422 (64.9%). Most of them were not monitoring their BP regularly i.e., 435 (66.8%). More than half of them were not doing physical exercise, i.e., 408 (62.8%).
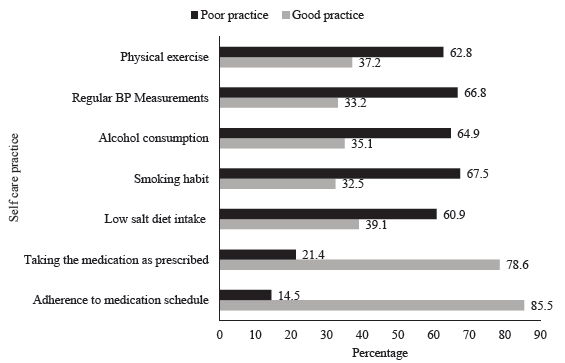
- Distribution of self-care practices among study participants (n=650).
Table II shows the association between socioeconomic characteristics and self-care scores. A statistically significant association was observed between age group, education, occupation, type of family, marital status, socioeconomic status, and self-care scores. However, no statistically significant association was found between gender and self-care scores.
| Variable | Category | Self-care behaviour | X2 value | df | P value | |
|---|---|---|---|---|---|---|
| Good, n (%) | Poor, n (%) | |||||
| Gender | Female | 112 (46.5) | 182 (44.5) | 0.239 | 1 | 0.625 |
| Male | 129 (53.5) | 227 (55.5) | ||||
| Age (yr) | 18-30 | 15 (6.2) | 12 (2.9) | 11.75 | 3 | 0.008 |
| 31-50 | 137 (56.8) | 245 (59.9) | ||||
| 51-70 | 85 (35.3) | 127 (31.1) | ||||
| >70 | 4 (1.7) | 25 (6.1) | ||||
| Education | Illiterate | 132 (54.8) | 159 (38.9) | 19.9 | 2 | <0.001 |
| Schooling | 74 (30.7) | 197 (48.2) | ||||
| Degree/Diploma | 35 (14.5) | 53 (13) | ||||
| Occupation | Unemployed | 121 (50.2) | 38 (9.3) | 137.39 | 1 | <0.001 |
| Employed | 120 (49.8) | 371(90.7) | ||||
| Type of family | Joint family | 99 (41.1) | 285 (69.7) | 52.02 | 2 | <0.001 |
| Nuclear family | 129 (53.5) | 116 (28.4) | ||||
| Three generation | 13 (5.4) | 8 (2) | ||||
| Marital status | Married | 205 (85.1) | 382 (93.4) | 11.69 | 2 | <0.001 |
| Unmarried | 19 (7.9) | 14 (3.4) | ||||
| Divorced/Widowed | 17 (7.1) | 13 (3.2) | ||||
| Socioeconomic status | Upper | 5 (2.1) | 0 | 160.8 | 4 | <0.001 |
| Upper middle | 46 (19.1) | 11 (2.7) | ||||
| Upper lower | 58 (24.1) | 77 (18.8) | ||||
| Lower middle | 80 (33.2) | 44 (10.8) | ||||
| Lower | 52 (21.6) | 277 (67.7) | ||||
df, degree of freedom; X2, Chi square value
Table III presents the association between hypertension control and self-care scores. It was indicated that there was a statistically significant association between the control of hypertension and self-care scores among study participants.
| Hypertension control | Self-care behaviour scale | X2 value | df | P value | |
|---|---|---|---|---|---|
| Good, n (%) | Poor, n (%) | ||||
| Controlled | 230 (42.04) | 317 (57.96) | 36.55 | 1 | <0.001 |
| Uncontrolled | 11 (10.67) | 92 (89.32) | |||
Discussion
This study conducted in the city of Mysuru revealed a male predominance among the study participants (54.8%), which contrasts with the findings from a study conducted in Andra Pradesh in 201922. The potential reasons for this gender disparity in hypertension could be due to sample differences or population-specific differences due to genetic predispositions. Moreover, differences related to lifestyle, such as smoking and alcohol consumption, could be linked to an elevated risk of hypertension. More than half of the hypertensive study participants (58.7%) were within the 31-50 yr age group, which was consistent with the findings from a study in Ethiopia (2022)23.
A majority of the participants had normal body weight (395, 60.8%), followed by 182 (28%) who were classified as overweight, 47 (7.2%) as obese, and only 26 (4%) as underweight. Maintaining a healthy weight is vital for hypertension management, as obesity is a well-established risk factor for its development and progression. However, this finding contradicts a study conducted in southern Iran in 201615. Approximately 44.8 per cent of the study participants in our study were illiterate. This finding aligned with that of a study conducted in Kathmandu in 202224. Moreover, our findings indicated that illiteracy and low education levels could serve as barriers to comprehending and adopting self-care practices.
The majority (75.5%) of the study subjects were employed. This finding aligns with the findings of a study conducted in southern Iran in 201615. It underscores the importance of considering occupational factors when designing interventions, as occupational demands and resources can significantly influence self-care behaviour and health outcomes. The majority of the study subjects were married (90.5%), as was the findings of a study from Eastern Ethiopia in 201625. Marital status can influence social support and the ability to engage in self-care practices, emphasizing the importance of involving spouses or partners in hypertension management.
Half of the study participants belonged to the lower class (50.6%), followed by the upper class (20.8%), lower middle class (19.1%), and upper middle class (8.8%). This distribution highlights the association between socioeconomic status and health outcomes, with lower socioeconomic status being associated with a higher prevalence of hypertension and poorer access to healthcare resources, similar to a study conducted in Bangladesh in 202226. Most of the study participants (86.9%) did not have health insurance, indicating a potential barrier to accessing healthcare services. This finding highlighted the need for policy interventions to ensure equitable access to healthcare and financial protection for individuals with hypertension. More than half of the study participants (63.2%) had a family history of hypertension. This suggested a potential genetic predisposition to hypertension and the importance of family-based interventions promoting awareness, screening, and lifestyle modifications for individuals with a family history of the condition. However, the findings of our study contradicted that of a study conducted in Ethiopia in 202223.
The study participants belonging to 31-50 age group had higher proportions of individuals with low self-care behaviour, which was consistent with a study conducted in Northwest Ethiopia (2021)27. The study revealed a significant association between education level and self-care behaviour, with individuals who attained a degree or diploma demonstrating the highest percentage of good self-care practice. This finding is supported by a study conducted in Kolkata in 201613. There was a significant association between the occupation and self-care behaviour. However, this finding aligned with a study conducted in Turkey in 202028.
The study revealed a significant association between socioeconomic status and self-care behaviour. Individuals from higher socioeconomic classes demonstrated good self-care behaviour compared to those belonging to lower socioeconomic classes. This finding contradicted the findings of a study conducted in Nepal (2021)29. There was a statistically significant association between the control of hypertension and self-care behaviour, which was similar to the point highlighted in an systematic review (2023)30, underlining the relationship between self-care and controlled hypertension.
One of the limitations of our study is its cross-sectional design, which restricts establishing temporal relationships between explanatory and outcome variables. Sampling strategy followed by us also introduced selection bias as there was purposive selection and this approach limited the generalizability of the findings to other populations. The absence of ROC analysis for determining the HBP-SCP scale’s cut-off score was another limitation. Additionally, reliance on self-reported data, especially for self-care practices and awareness, might have introduced recall bias. The study also did not consider potential confounding factors like comorbidities or variations in healthcare access, which might have adversely impacted inferences.
Overall, this study emphasized the necessity of integrating self-care awareness into existing health programmes. By incorporating components focused on self-care education and empowerment, these programs can better equip individuals with the knowledge and skills necessary for effective hypertension management. Overall, the findings underscored the urgency of implementing targeted interventions and policy initiatives to address the growing burden of hypertension, particularly among vulnerable populations residing in urban slum areas.
Financial support & sponsorship
None.
Conflict of Interest
None.
Use of Artificial Intelligence (AI)-Assisted Technology for manuscript preparation
The authors confirm that there was no use of AI-assisted technology for assisting in the writing of the manuscript and no images were manipulated using AI.
References
- Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1923-94.
- [Google Scholar]
- World heart federation roadmap for hypertension-update. Available from: https://world-heart-federation.org/wp-content/uploads/WHF-Hypertension-Roadmap-Summary.pdf, accessed on August 8, 2023.
- Addressing global disparities in blood pressure control: Perspectives of the international society of hypertension. Cardiovasc Res. 2023;119:381-409.
- [Google Scholar]
- Hypertension control rate in India: Systematic review and meta-analysis of population-level non-interventional studies, 2001-2022. Lancet Reg Health Southeast Asia. 2023;9:100113.
- [Google Scholar]
- Hypertension treatment cascade among men and women of reproductive age group in India: Analysis of national family health survey-5 (2019–2021) Lancet Reg Health Southeast Asia. 2024;23:100271.
- [Google Scholar]
- National Programme for prevention & Control of Cancer, Diabetes, Cardiovascular Diseases & stroke (NPCDCS). Available from: https://nhm.gov.in/index1.php?lang=1&level=2&sublinkid=1048&lid=604#:∼:text=In%20order%20to%20prevent%20and,early%20diagnosis%2C%20management%20and%20referral, accessed on September 8, 2024.
- Inadequate hypertension control rates: A global concern for countries of all income levels. J Clin Hypertens (Greenwich). 2022;24:362-4.
- [Google Scholar]
- Prevalence of hypertension among the rural population of Mehsana district of North Gujarat region, India. Int J Community Med Public Health. 2021;8:5847.
- [Google Scholar]
- Hypertension and epidemiological factors among tribal labor population in Gujarat. Indian J Public Health. 2008;52:144-6.
- [Google Scholar]
- Prevalence and risk factors of hypertension, among adults residing in an urban area of North India. Int J Pure Appl Biosci. 2015;3:338-44.
- [Google Scholar]
- Study of prevalence and risk factors of hypertension in adults in an urban slum area of Western Maharashtra, India. Int J Community Med Public Health. 2016;3:2812-6.
- [Google Scholar]
- Prevalence, awareness, and control of hypertension in the slums of Kolkata. Indian Heart J. 2016;68:286-94.
- [Google Scholar]
- The association between self-efficacy and self-care in essential hypertension: A systematic review. BMC Fam Pract. 2021;22:44.
- [Google Scholar]
- Self-care behaviors and related factors in hypertensive patients. Iran Red Crescent Med J. 2016;18:e35805.
- [Google Scholar]
- Self-care for health. A handbook for community health workers & volunteers. Available from: https://iris.who.int/bitstream/handle/10665/205887/B5084.pdf?sequence=1&isAllowed=y, accessed on August 8, 2023.
- The PREMIER intervention helps participants follow the dietary approaches to stop hypertension dietary pattern and the current dietary reference intakes recommendations. J Am Diet Assoc. 2007;107:1541-51.
- [Google Scholar]
- Prevalence rates of self-care behaviors and related factors in a rural hypertension population: A questionnaire survey. Int J Hypertens. 2013;2013:526949.
- [Google Scholar]
- Development and validation of the hypertension self-care profile: A practical tool to measure hypertension self-care: A practical tool to measure hypertension self-care. J Cardiovasc Nurs. 2014;29:E11-20.
- [Google Scholar]
- Hypertension self-care practice and associated factors among patients in public health facilities of Dessie town, Ethiopia. BMC Health Serv Res. 2019;19:51.
- [Google Scholar]
- Preliminary validation of the Hypertension Self-Care Activity Level Effects (H-SCALE) and clinical blood pressure among patients with hypertension. J Clin Hypertens (Greenwich). 2013;15:637-43.
- [Google Scholar]
- Hypertension among adults in urban slums, a cross-sectional study in Rajamahendravaram, Andhra Pradesh, India. Indian J Forensic Comm Med. 2019;6:75-80.
- [Google Scholar]
- Self-care practice among adult hypertensive patients at ambulatory clinic of tertiary teaching Hospital in Ethiopia: A cross-sectional study. J Pharm Policy Pract. 2022;15:23.
- [Google Scholar]
- Factors associated with self-care behaviours among people with hypertension residing in Kathmandu: a cross-sectional study. BMJ Open. 2023;13:e070244.
- [Google Scholar]
- Self-care practice and associated factors among hypertensive patients in public health facilities in Harar town, Eastern Ethiopia: A cross-sectional study. SAGE Open Med. 2020;8:2050312120974145.
- [Google Scholar]
- Prevalence, risk factors, awareness, and control of hypertension: A cross-sectional study in an urban slum area of Bangladesh. J Health Med Sci. 2022;5:26-34.
- [Google Scholar]
- Self-care practice and associated factors among hypertensive patients in Debre Tabor Referral Hospital, Northwest Ethiopia, 2020. Int J Hypertens. 2021;2021:3570050.
- [Google Scholar]
- The prevalence of hypertension and influencing factors among the employees of a university hospital. Afr Health Sci. 2020;20:1725-33.
- [Google Scholar]
- Socioeconomic status and its relation to hypertension in rural Nepal. Int J Hypertens. 2021;2021:5542438.
- [Google Scholar]
- Determinants of self-care and home-based management of hypertension: An integrative review. Glob Heart. 2023;18:16.
- [Google Scholar]




