
Translate this page into:
Assessment of osteoporotic fracture risk in urban Indian population using quantitative ultrasonography & FRAX tool
Reprint requests: Dr Vipul Vijay, Consultant, Department of Orthopedics, Indraprastha Apollo Hospital, Sarita Vihar, New Delhi 110 076, India e-mail: dr_vipulvijay@yahoo.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
There have been studies around the world on the prevalence of osteoporosis and its related risk factors, but there have been limited studies on risk factors and osteoporosis in the Indian population. In this study, the incidence of osteoporosis and the associated clinical risk factors (CRFs) were studied in the urban Indian population.
Methods:
Bone mineral density of 445 individuals >38 yr of age using qualitative ultrasound (QUS) was assessed. The patients were also questioned regarding the presence of the various CRFs as per the FRAX tool. The patients were categorized into normal, osteopenia and osteoporosis groups on the basis of T-score from QUS.
Results:
There were 223 males and 222 females in this study. Sex was significantly associated with T-score (P<0.001). Forty (8.99%) patients were osteoporotic, 265 (59.55%) were osteopenic and the remaining 140 (31.46%) were normal. A significant association of T-score was found with parent history of fracture (P<0.05), rheumatoid arthritis (P<0.05) and secondary osteoporosis (P<0.05). Previous history of fracture's association was not found to be significant. Smoking, alcohol intake and steroid intake were not found to be significantly associated with T-scores.
Interpretation & conclusions:
The incidence of osteoporosis was found to be high in the urban Indian population. More care and attention should be targeted towards elderly, especially the ones with the risk factors to prevent osteoporosis in future.
Keywords
BMD
epidemiology
fracture risk
FRAX
osteoporosis
risk
urban Indian

Osteoporosis is usually considered a ‘silent disease’ until a fracture occurs1. Osteoporosis leads to nearly nine million fractures annually worldwide2. Osteoporotic fractures are defined as fractures associated with low bone mineral density (BMD) and include clinical spine, hip, forearm and shoulder fractures.
BMD using dual-energy X-ray absorptiometry (DXA) is the standard diagnostic technique for osteoporosis but its cost is relatively high, and there is a shortage of DXA machines through most of the developing Asian countries3. As a result, other clinical prediction tools have been developed, such as the Osteoporosis Self-assessment tool4 and the Kohn Kaen Osteoporosis Study Score5 in an attempt to identify people at risk of osteoporosis and who should receive a DXA scan.
The issues with measurement of DXA linked to DXA scan can be circumvented by quantitative ultrasound (QUS) as it may offer an alternative tool for screening or assessment of risk of poor bone health in large populations. QUS measures the peripheral skeleton and may give assessment of bone micro-architecture in addition to bone mass6.
BMD tests alone are not optimal for the detection of individuals at high risk of fracture7 because osteoporotic fracture can occur in patients with any given T-score8, even in individuals with normal BMD values, according to the World Health Organization (WHO) classifications9. Fracture risk is multi-factorial; thus, many independent factors, including those related to the risk of fall, contribute to the risk over and above that reflected by BMD10.
A WHO scientific group proposed that the 10-yr probability of fracture calculated using information on clinical risk factors (CRFs), with or without BMD data, should be used to express fracture risk for clinical assessment8 and to determine interventional thresholds11.
The FRAX tool developed by the WHO is used in assessment of both clinical fracture risk and BMD12. In the final FRAX® model, developed by the University of Sheffield in 2008, the risk of fracture is calculated in men or women from age, body mass index (BMI) computed from height and weight and independent risk variables comprising a prior fragility fracture, parental history of hip fracture (HF), current tobacco smoking, long-term use of oral glucocorticoids, rheumatoid arthritis (RA), other causes of secondary osteoporosis and daily alcohol consumption of three or more units daily. However, fracture risk is strongly affected by ethnicity13, so fracture risk factors should be evaluated according to each ethnic and population group14.
In this study, the occurrence of osteoporosis in the urban Indian population was studied. Identification of various risk factors that predict fracture, alone and in association with QUS of the calcaneus, was also done.
Material & Methods
This study was conducted in the department of Orthopaedics, Indraprastha Apollo Hospital, New Delhi, India. The community outreach programme was organized with the help of a non-government organization (NGO). The senior citizen forum and the resident welfare associations in the areas of Central and East Delhi were contacted and those who volunteered for the camp were included in the study. Fourteen camps were organized in total and every third person attending the camp was included in the study. The study duration was from October 2012 to March 2013. The areas covered were Sukhdev Vihar, Ishwar Nagar, Sarita Vihar, Jasola, Kalkaji, East of Kailash, New Friends Colony, Maharani Bagh, Lajpat Nagar - I, II, III, IV, Nizamuddin and Mayur Vihar. The cluster of individuals mainly belonged to the middle and upper class, according to revised modified BG Prasad classification15. The number of patients included in the study from each camp ranged from 20 to 35. The study protocol was approved by the institutional ethics committee and written informed consent was obtained from each participant.
The total population according to 2011 census16 in the areas of Central and East Delhi above the age of 38 yr was 1,480,492. The sample size required for a precision of 5 per cent and a 95 per cent confidence interval and a power of 80 per cent was 385. The minimum sample size was decided to be 385. The investigated risk factors included dairy product consumption, cigarette smoking, alcohol consumption (>3 units per week), personal history of RA, history of medication use, such as steroids (oral glucocorticoids for more than three months at a dose of prednisolone of 5 mg daily or more or equivalent doses of other glucocorticoids) and history of previous fracture (to include a fracture occurring spontaneously or due to trauma which would not cause fracture in an otherwise healthy individual). Individuals were asked about cigarette smoking (current, past or never) and alcohol consumption (units per week). Height, body weight and BMI were calculated, and weight was stratified into four categories based on BMI17: underweight <18.5 kg/m2, normal 18.5 to 22.9 kg/m2, overweight 23.0 to 24.9 kg/m2 and obese >25.0 kg/m2.
BMD measurement in 445 individuals of more than 38 yr of age, using Ultrasonic GE Machine (model no GE: Achilles EXPII, GE Healthcare, USA), was done. The T-score of each individual was calculated and recorded, after testing by the machine at calcaneum. Jin et al18, in a population-based study on 106 Chinese women, have suggested that the division of the population into subgroups on the basis of QUS can be done using the same criteria as for DXA scan as advised by the WHO. Hence, the groups were divided into normal, osteopenic and osteoporotic on the basis of T-score from QUS as per the WHO criteria1. The T-scores were classified into normal, osteopenia and osteoporosis, as per the WHO criteria (osteoporosis: ≥−2.5, osteopenia: −1.0 - −2.5 and normal: ≤−1.0).
Age, sex, BMI, history of previous fractures, parental history of HF, history of smoking, alcohol and glucocorticoids use, RA and secondary osteoporosis (premature menopause, malnutrition, type 1 diabetes/hyperthyroidism/ liver disease) were recorded. A probability of future fracture was calculated using FRAX tool of WHO. Using the FRAX tool, the number and percentage of the population needing treatment was calculated. A major osteoporotic fracture (MOF) risk of greater than or equal to 20 per cent or an HF risk greater than or equal to three per cent were considered candidates for starting treatement13.
Statistical analysis: Statistical testing was conducted with the Statistical Package for the Social Sciences version 17.0(SPSS, IBM Corp., Armonk, NY, USA). Continuous variables were presented as mean. Categorical variables were expressed as frequencies and percentages. Categorical data between the groups were compared using Chi-squared test. Correlation between continuous variables was computed using Pearson's correlation test.
Results
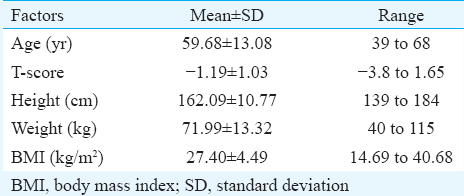
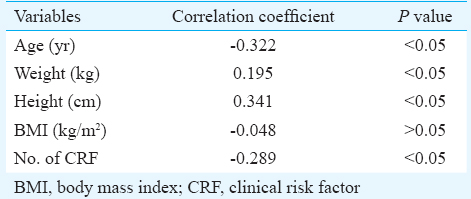
The 445 individuals in this study were in the age group of 38-68 yr (mean±SD: 59.68±13.08 yr) (Table I). Difference in mean age among three group was significant i.e., age of patients was significantly (P<0.05) associated with T-score (Table II). There were 223 males and 222 females in this study. Forty (8.99%) individuals belonged to group 2 (osteoporotic) whose T-score ranged from −3.8 - −2.5, 265 (59.55%) belonged to group 1 (osteopenic) (T-score: −2.49 - −1.0) and the remaining 140 (31.46%) belonged to group 0 (normal) (T-score: −0.99 - max). The ages (mean±SD, range) of the groups 0, 1 and 2 were 61.32±13.83 (40-89 yr), 61.23±13.33 (40-90 yr) and 61.15±13.33 (40-89 yr), respectively.
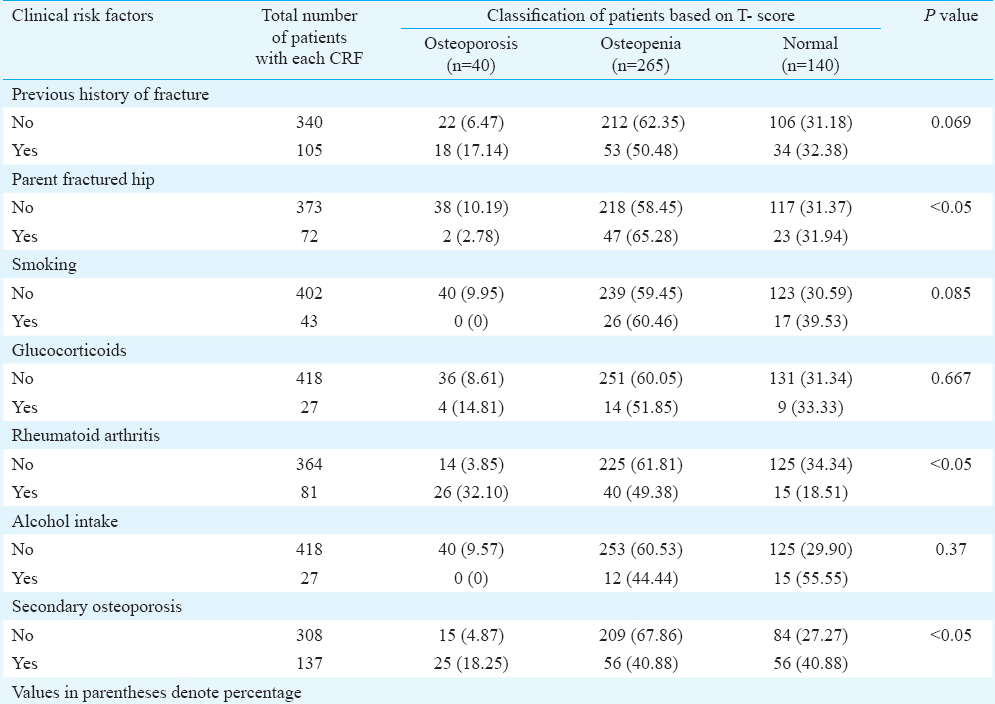
The significance of the association of various risk factors with osteopenia/osteoporosis was studied. Using Chi-square test, significance of association of these risk factors with osteopenia/osteoporosis was also assessed. Sex of the patients was found to be significantly associated with T-score (P<0.001). Significant association was also found with parent history of fracture (P<0.05), RA (P<0.05) and secondary osteoporosis (P<0.05) (Table III). Previous history of fracture was not found to be significantly associated with osteoporosis. Smoking and alcohol intake were not found to be significantly associated with T-scores (Table III). No association of steroid intake was found with T-scores (Table III).
Using the FRAX score, the MOF risk ranged from 0.70 to 25 per cent and the risk of HF ranged from 0 to 21 per cent. Of the 445 participants, the number of individuals with greater than 20 per cent MOF risk was 20 (0.04%) and the number of individuals with HF risk greater than three per cent was 93 (20.89%). The total number of individuals needing treatment, as per the criteria, out of a total population of 445 was 113 (25.39%).
Discussion
Identification of individuals who are at risk of developing osteoporosis and adequate treatment can prevent long-term morbidity due to osteoporotic fractures. Unfortunately, most population is largely unaware of the serious complications associated with osteoporosis.
Even in the absence of a large scale cross-sectional study, HFs are considered common and the peak incidence of osteoporotic HF is in younger age, around 50-60 yr19. Almost four decades ago, Nordin20 reviewed 119 HFs and found that, in India, these occurred at all ages, with two peaks at 30-39 yr and again at 50-70 yr. There was no attempt to distinguish traumatic from fragility fractures20. Shetty et al21, in their epidemiological study of 256 south Indian males, utilized the FRAX tool for fracture risk stratification and found that approximately 25 per cent of the population studied needed treatment (i.e. had MOF risk >20% or HF risk >3%). The probability of fracture risk using the FRAX tool increases when the BMD was added to the CRFs22.
Indians living in Singapore were also found to have HFs at an average age of 58 yr22. A study involving 1393 patients of HFs from three large Delhi hospitals, also indicated that these fractures were common in both sexes, although the sex ratio in different subgroups was variable, and not always in favour of men23.
Evidently, the ideal management should be two pronged, one by minimizing the risk of acquiring the disease begins by modification of individuals’ lifestyle to combat-related risk factors and second by identification of patients at high risk to reduce future fractures. Among many risk factors, some are modifiable (such as low BMD and steroid intake) and others non-modifiable (such as advanced age, personal and parental history of fracture) are associated with osteoporosis20242526. Minor risk factors for MOF include, but are not limited to, inadequate nutritional supplementation of vitamin D and calcium, impaired eyesight despite correction, high alcohol and tobacco consumption and immobilization27. The average age at menopause in Indian women has been reported to be slightly lower than the average Caucasian female25. This decreased exposure to oestrogen in a female in her lifetime is a major risk factor for osteoporosis. There are other described modifiable risk factors which have been associated with the low BMD in the Indian population. The most important factor is low dietary intake of calcium and vitamin D. The causes of poor dietary intake of calcium include a large vegetarian population and the absence of government guidelines regarding fortification of food. Moreover, due to the increasing costs of dairy products, a large population is unable to afford them. Harinarayan et al27 attributed the increased intake of phytates in the Indian diet as another major contributing factor for the poor absorption of dietary calcium. Other contributing factors include highly pigmented skin and overall low sun exposure.
A screening tool is hence needed which can be used in the community setup and can help identify people at increased risk of osteoporosis. Several studies have shown that QUS at peripheral sites can be used as a screening tool to assess bone health6. It is relatively inexpensive, and is portable, and therefore, can be used as a tool to screen for poor bone health at the community level. QUS has also been shown to be as good as BMD assessed by DXA in predicting fracture risk28.
In experimental settings, the technique captures some structural aspects, as shown from scans undertaken in different axes of cubes of bone28. The performance of these QUS techniques has been evaluated29. The technique cannot currently provide diagnostic criteria for osteoporosis, but can be used for the assessment of fracture risk in elderly women where the prognostic value of future HF is as good as several other peripheral measurements29. In the elderly people, it has been reported that the QUS may give results similar to a central DXA30. It also appears to predict HF and non-spine fracture in men.
In the present study, 8.99 per cent patients had osteoporosis and 59.55 per cent patients had osteopenia. Thus, the overall population at risk in this study was found to be approximately 69 per cent. This could have serious socio-economic burden in the future as the population of the elderly are bound to increase. Nine per cent prevalence of osteoporosis has been reported in northern India31. In a study in Indian women of different age groups, prevalence of osteoporosis has been described as ranging from 8 to 62 per cent in Indian women of different age groups31. In our study, the presence of osteopenia and osteoporosis was found to be higher in the urban Indian population.
In our study, the overall percentage of the study population needing treatment as per the FRAX score criteria was found to be 25.39 per cent. Of this, majority of the population was at a risk of developing an HF. This correlated well with a similar study by Shetty et al21, who in their study of south Indian males reported that the total percentage of population needing treatment as per FRAX criteria were 24.6 per cent. The 10-yr probability of MOF and HF was significantly associated with higher age and female gender. Parent history of fracture, presence of secondary osteoporosis and RA were also significantly associated with 10-yr probability of HF and MOF. Similar results were found in literature by some authors in other populations26. The results were consistent with results published in literature where similar significant association between risk of osteoporosis and such variables was found24.
Our study had certain limitations. First, the sample was limited to one urban city. Since this was a community-based study, all the patients who presented with any musculoskeletal complaints were included in the study. It has been suggested that in individuals <50 yr of age group, T-score alone should not be used in the diagnosis and management of osteoporosis. The T-score along with the assessment of other risk factors should be used in this population. Since FRAX tool was used in all the patients included in the study, any skewing due to use of only T-scores in patients <50 yr was avoided32. Furthermore, the menstrual status of the population was not recorded at the time of enrolment in the study. Vitamin D levels of the study population were not estimated.
In conclusion, a high incidence of osteopenia and osteoporosis was observed in the studied population. Significant association of sex, parent history of fracture and secondary osteoporosis was found in the present study whereas alcohol and steroid intake were not found to be significantly associated with the low T-scores. Further research and studies regarding fracture rates, genetic component of osteoporosis and evaluation of the applicability accuracy and feasibility of universal use of FRAX in Indian population are needed.
Acknowledgment
The camps for this study were held with the help of Arthritis Care Foundation, New Delhi, India.
Conflicts of Interest: None.
References
- NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA. 2001;285:785-95.
- [Google Scholar]
- An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 2006;17:1726-33.
- [Google Scholar]
- The Asia-Pacific regional audit-epidemiology, costs, and burden of osteoporosis in India 2013: A report of International Osteoporosis Foundation. Indian J Endocrinol Metab. 2014;18:449-54.
- [Google Scholar]
- The osteoporosis self-assessment screening tool: A useful tool for the orthopaedic surgeon. J Bone Joint Surg Am. 2007;89:765-72.
- [Google Scholar]
- Development and validation of a new clinical risk index for prediction of osteoporosis in Thai women. J Med Assoc Thai. 2004;87:910-6.
- [Google Scholar]
- Evaluation of bone mineral density by quantitative ultrasound of bone in 16,862 subjects during routine health examination. Br J Radiol. 2001;74:602-6.
- [Google Scholar]
- World Health Organization. WHO scientific group on the assessment of osteoporosis at the primary health care level. 2007. Brussels: WHO; Available from: http://www.who.int/chp/topics/Osteoporosis.pdf
- [Google Scholar]
- A new approach to the development of assessment guidelines for osteoporosis. Osteoporos Int. 2002;13:527-36.
- [Google Scholar]
- Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group. World Health Organ Tech Rep Ser. 1994;843:1-129.
- [Google Scholar]
- Assessment of the 10-year probability of osteoporotic hip fracture combining clinical risk factors and heel bone ultrasound: The EPISEM prospective cohort of 12,958 elderly women. J Bone Miner Res. 2008;23:1045-51.
- [Google Scholar]
- FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int. 2008;19:385-97.
- [Google Scholar]
- Osteoporosis and fracture risk in women of different ethnic groups. J Bone Miner Res. 2005;20:185-94.
- [Google Scholar]
- Ten-year risk of osteoporotic fractures in postmenopausal Chinese women according to clinical risk factors and BMD T-scores: A prospective study. J Bone Miner Res. 2007;22:1080-7.
- [Google Scholar]
- Ministry of Labour, Government of India. Construction and Maintenance of Index numbers. Available from: http://www.labourbureau.nic.in
- [Google Scholar]
- Census Organization of India. Population Census 2011. Available from: https://www.census2011.co.in
- 2000. Available from: http://www.wpro.who.int/nutrition/documents/docs/Redefiningobesity.pdf
- Assess the discrimination of Achilles InSight calcaneus quantitative ultrasound device for osteoporosis in Chinese women: Compared with dual energy X-ray absorptiometry measurements. Eur J Radiol. 2010;76:265-8.
- [Google Scholar]
- Prevalence and related risk factors of osteoporosis in peri- and postmenopausal Indian women. J Midlife Health. 2011;2:81-5.
- [Google Scholar]
- Osteoporosis in healthy South Indian males and the influence of life style factors and vitamin D status on bone mineral density. J Osteoporos. 2014;2014:723238.
- [Google Scholar]
- Femoral neck fractures among the major racial groups in Singapore. Incidence patterns compared with non-Asian communities. II. Singapore Med J. 1964;4:150-7.
- [Google Scholar]
- Clinical studies: Incidence of fracture neck of femur and intertrochanteric fractures in three Delhi hospitals. In: Sankaran B, ed. Osteoporosis. New Delhi: South East Asia Regional Office, World Health Organization; 2000. p. :9-18.
- [Google Scholar]
- Oral corticosteroids and fracture risk: Relationship to daily and cumulative doses. Rheumatology (Oxford). 2000;39:1383-9.
- [Google Scholar]
- Age and symptomatology of menopause in Indian women. J Postgrad Med. 1983;29:218-22.
- [Google Scholar]
- 2002 Clinical practice guidelines for the diagnosis and management of osteoporosis in Canada. CMAJ. 2002;167(10 Suppl):S1-34.
- [Google Scholar]
- High prevalence of low dietary calcium, high phytate consumption, and Vitamin D deficiency in healthy south Indians. Am J Clin Nutr. 2007;85:1062-7.
- [Google Scholar]
- Do quantitative ultrasound measurements reflect structure independently of density in human vertebral cancellous bone? Bone. 1998;23:425-31.
- [Google Scholar]
- Prediction of hip fracture in elderly women: A prospective study. BMJ. 1990;301:638-41.
- [Google Scholar]
- Quantitative ultrasound predicts hip and non-spine fracture in men: the MrOS study. Osteoporos Int. 2007;18:771-7.
- [Google Scholar]
- Epidemiology and treatment of osteoporosis in women: An Indian perspective. Int J Womens Health. 2015;7:841-50.
- [Google Scholar]
- Common mistakes in the clinical use of bone mineral density testing. Nat Clin Pract Rheumatol. 2008;4:667-74.
- [Google Scholar]




