Translate this page into:
Anomalous origin of left coronary artery in an adult
* For correspondence: senthilkumarpgi@yahoo.co.in upasranga@yahoo.co.in
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
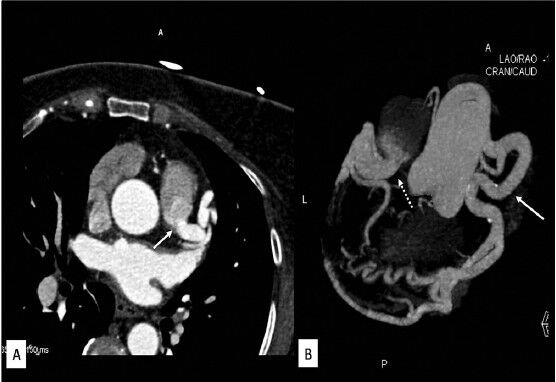
A 50-year-old female patient presented to Department of Cardiology, Saveetha Medical College and Hospital, Kancheepuram, India, in December 2012, with a history of exertional chest pain relieved by rest for the past three months. Electrocardiogram showed ST/T wave changes in leads I, V6 and AVL suggesting lateral ischaemia. No significant past medical or surgical history was present. Transthoracic echocardiography showed mildly decreased left ventricular ejection fraction (45%) with abnormal septal doppler flow pattern and reverse flow in pulmonary artery. No regional wall motion abnormality was detected in resting echocardiography. Stress test was inconclusive. The patient was suspected to have ALCAPA (anomalous origin of the left coronary artery from the pulmonary artery) hence 128 slice CT coronary angiography was requested. Electrocardiographically-gated multidector computed tomographic (CT) angiography showed origin of left main coronary artery from pulmonary artery (Fig. 1A and B). Right coronary artery was dilated and tortuous with presence of multiple dilated collateral branches (Figs 1B and 2). The patient was advised catheter coronary angiogram and surgery, however, the patient refused and she is currently on medical management.
-
(A) Axial CT coronary angiography image showing origin of left coronary artery from main pulmonary artery (white arrow), and (B) Coronal maximum intensity projection image showing origin of left coronary artery from main pulmonary artery (white arrow with dotted line). Right coronary artery arising normally from aorta is dilated and tortuous (white arrow) with multiple prominent collateral branches.
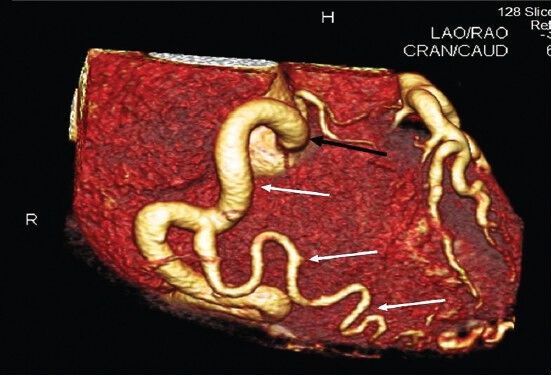
- Coronal 3-D volume rendered CT coronary angiography image showing dilated tortuous right coronary artery arising from aorta (black arrow) with dilated collateral branches (white arrows).
ALCAPA is a rare congenital anomaly with an incidence of 1 in 300,000 live births and represents 0.5 per cent of all cases of congenital heart disease. Most of the cases (85%) are diagnosed within first month of life1. Nearly 90 per cent of untreated patients die within one year, however, a few patients can survive into adulthood due to adequate collateral blood supply to the left coronary circulation through dominant right coronary artery. Regional wall motion abnormality is commonly seen in most of the patients with ALCAPA surviving till adult life, although surprisingly not seen in our case likely due to extensive collaterals from right coronary artery2. Coronary CT angiography can demonstrate the primary and secondary features of ALCAPA in 3-dimensional projection thereby helping the surgeon. ALCAPA presenting at older age should be treated surgically3.
References
- Anomalous right coronary artery arising from the pulmonary artery: a report of 7 cases and a review of the literature. Am Heart J. 2006;152:1004.
- [Google Scholar]
- Presentation of anomalous origin of the left coronary artery from the pulmonary artery with left sided coronary ostium in an adult patient. Iranian Cardiovascular Res J. 2009;3:109-15.
- [Google Scholar]
- A 69-year-old woman with anomalous origin of left coronary artery from the pulmonary artery: surgical repair using a trap-door flap. Korean J Thorac Cardiovasc Surg. 2011;44:358-60.
- [Google Scholar]




