Translate this page into:
An unusual cause of superior vena cava syndrome
*For correspondence: sksharma.aiims@gmail.com sksharma.aiims@yahoo.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 17-year-old boy presented with gradually increasing retrosternal bulge of four years duration. He developed multiple non-tender woody nodules and discharging sinuses over anterior chest wall over the years and presented with features of superior vena cava obstruction (Fig. 1). Multiple biopsies from nodules were inconclusive and he had received anti-tuberculosis treatment twice in the past. Contrast-enhanced computed tomography (CECT) revealed soft tissue density in the anterior and middle mediastinum (Fig. 2A). Magnetic resonance imaging (MRI) revealed hypointense mass in T2-weighted axial image (Fig. 2B). Fine needle aspiration cytology (FNAC) from a lump revealed actinomyces. He received ceftriaxone for 6 weeks followed by doxycycline for 1 year. The sinuses dried, the nodules softened and decreased in size with modest reduction in retrosternal bulge; however, dilated veins persisted. Surgical option was ruled out in view of extensive fibrosis encasing the major vessels. Fibrosing mediastinitis (FM) has been most commonly associated with histoplasmosis and tuberculosis. Other infectious causes implicated include aspergillosis, mucormycosis, blastomycosis, and cryptococcosis. Actionomycosis is a rare cause of FM and superior vena cava syndrome12.

- shows retrosternal bulge, multiple discharging sinuses (black arrow) over anterior chest wall, non-pulsatile engorged neck veins (white arrow) and dilated, tortuous veins over the chest and abdominal wall with downward flow, suggestive of post-azygous superior vena cava (SVC) obstruction.
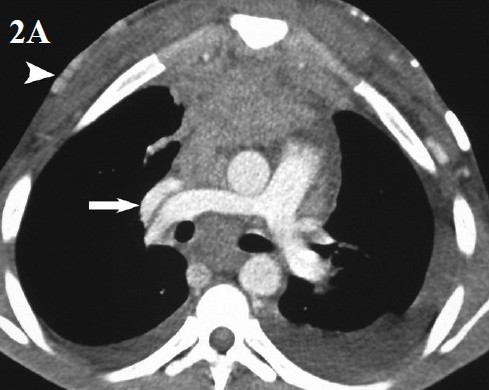
- CECT scan of the chest shows soft tissue density in the anterior and middle mediastinum encasing the SVC, aorta and pulmonary artery. SVC is chinked (arrow) with formation of multiple collaterals in the chest wall (arrowhead).

- MRI of the chest, T2-weighted axial image shows hypointense mass (arrow) suggesting its fibrotic nature.
References
- Thoracic actinomycosis as a cause of superior vena cava syndrome: report of a case. Surg Today. 2004;34:447-9.
- [Google Scholar]




