
Translate this page into:
An unusual cause of massive right leg swelling
*For correspondence: doctoranimeshray@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 27 yr old male†, non-smoker, presented to the department of Medicine, All India Institute of Medical Sciences, New Delhi, India in April 2019, with debilitating swelling of the right leg which started around two weeks ago. His physical examination showed pitting pedal odema of the right leg (Fig. 1). Routine blood tests, spirometry, tuberculin skin test, two-dimensional echocardiography and lower limb venous Doppler were unremarkable. Serum angiotensin-converting enzyme levels were elevated, while serum and urine calcium levels were normal. Chest imaging and subsequent whole-body positron emission tomography and computed tomography showed mediastinal lymphadenopathy (Fig. 2). Bronchoscopy with trans-bronchial needle aspiration (from the right paratracheal node) showed non-necrotising epithelioid cell granuloma (Fig. 3). Lymphoscintigraphy showed significant lymphatic obstruction of the right lower limb (Fig. 4). He was diagnosed as sarcoidosis with lymphatic involvement, leading to massive pedal odema. Treatment involved steroids to which he showed remarkable clinical improvement within four weeks. This was a rare presentation of a common disease, sarcoidosis.

- Severe pitting pedal oedema of the right leg of the patient; making it difficult for him to walk or drive his car.
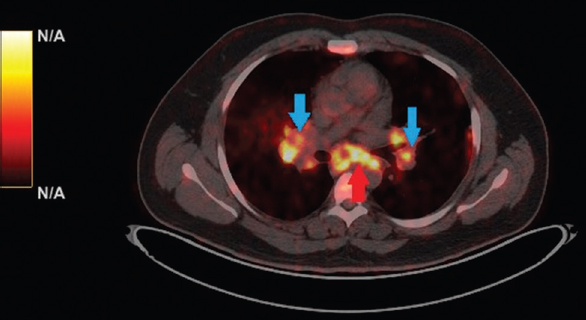
- A mediastinal lung window of 18-fluorodeoxyglucose positron emission tomography and computed tomography showing prominent bilateral interlobar (blue arrows) and sub-carinal (red arrow) lymphadenopathy; the florid fluorodeoxyglucose uptake signifies an active disease process.

- A haematoxylin and eosin-stained slide prepared from lymph node tissue derived from the right paratracheal lymph node; tissue was secured by endobronchial ultrasound sonography-guided trans-bronchial lymph nodal aspiration. It shows the presence of elongated nuclei within the macrophages (blue arrow) suggesting epithelioid granuloma with no evidence of necrosis; these features are suggestive of non-necrotizing granulomatous lymphadenitis; consistent with a picture of sarcoidosis (×400).

- A 99m-Tc sulphur colloid lymphoscintigraphy of both lower limbs; anteriorly the dye has reached both the inguinal nodes freely; posteriorly the dye has reached the left deep inguinal lymph node (blue arrow) but has not completely reached the deep inguinal lymph node on the right; thus signifying a lymphatic obstruction at the right popliteal lymph node (red arrow).
Conflicts of Interest: None.




