
Translate this page into:
An unusual cause of dysphagia in a child: Gastrointestinal manifestations of epidermolysis bullosa
*For correspondence: puriarchana@hotmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
An 11 yr old† child with histologically proven diagnosis of dystrophic epidermolysis bullosa (DEB) presented with progressively increasing dysphagia for solids for 2 years. There was no history of caustic ingestion or drug intake. He was malnourished and had generalised extensive cutaneous scarring, blistering, and erosions with haemorrhagic incrustation (Fig. 1A & B), irregular dentition (Fig. 1C) with enamel defects, microstomia and dystrophic nails. An oral contrast study showed a persistent concentric narrowing at the level of cricopharyngeus with delayed gastric emptying beyond eight hours, suggestive of esophageal and pyloric stenosis (Fig. 2A & B). He was started on peripheral parenteral nutrition and a gentle esophageal dilatation was attempted during flexible endoscopy but of no avail. Gastrostomy with gastrojejunostomy was planned and the risk of restenosis at the anastomotic site was explained to the attendants; however, they took the child away against medical advice. Esophageal webs, stricture and hiatal hernia are the manifestations of upper gastrointestinal involvement in DEB. Treatment options for esophageal stenosis include endoscopic fluoroscopic-guided balloon dilatation, steroids, hyperalimentation and oesophageal replacement as a last resort. Although neonatal pyloric atresia and stenosis are reported to occur in junctional EB, gastric outlet obstruction in an older child, as reported here, is unusual.

- (A) Photograph showing extensive generalized scarring with focal areas of hypopigmentation on abdomen (arrow). (B) Raw erosions, haemorrhagic encrustation and scarring in both legs (arrow). (C) Dental caries with enamel defect and irregular dentition with gingival oedema.
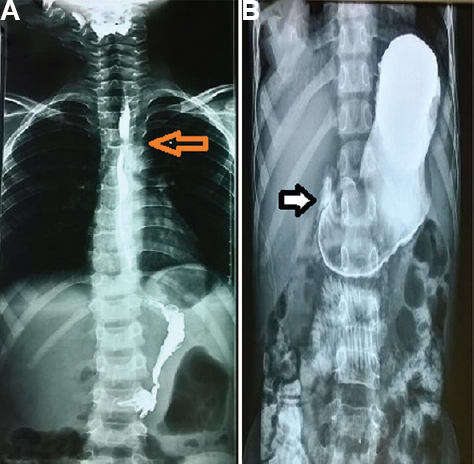
- (A) Oral contrast study showing persistent narrowing at cricopharyngeus (arrow). (B) Oral contrast study showing delayed gastric emptying at eight hours (arrow).
Conflicts of Interest: None.




