
Translate this page into:
An older male with fever-induced Brugada Syndrome
*For correspondence: fengxiangfei@xinhuamed.com.cn
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
An 81 yr old male† was referred to the department of Cardiology, Xinhua Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, PR China, in February 2016 because of two episodes of syncope over the past week. The patient denied a history of coronary artery disease and family history of structural heart disease or sudden death but reported a previous hospitalization for investigation of fever two years ago, and a routine electrocardiography (ECG) demonstrated Type 1 Brugada pattern (Fig. l). The temperature at the time of ECG recording was 101.8 °F. Repeated ECG after resolution of fever was near normal (Fig. 2).
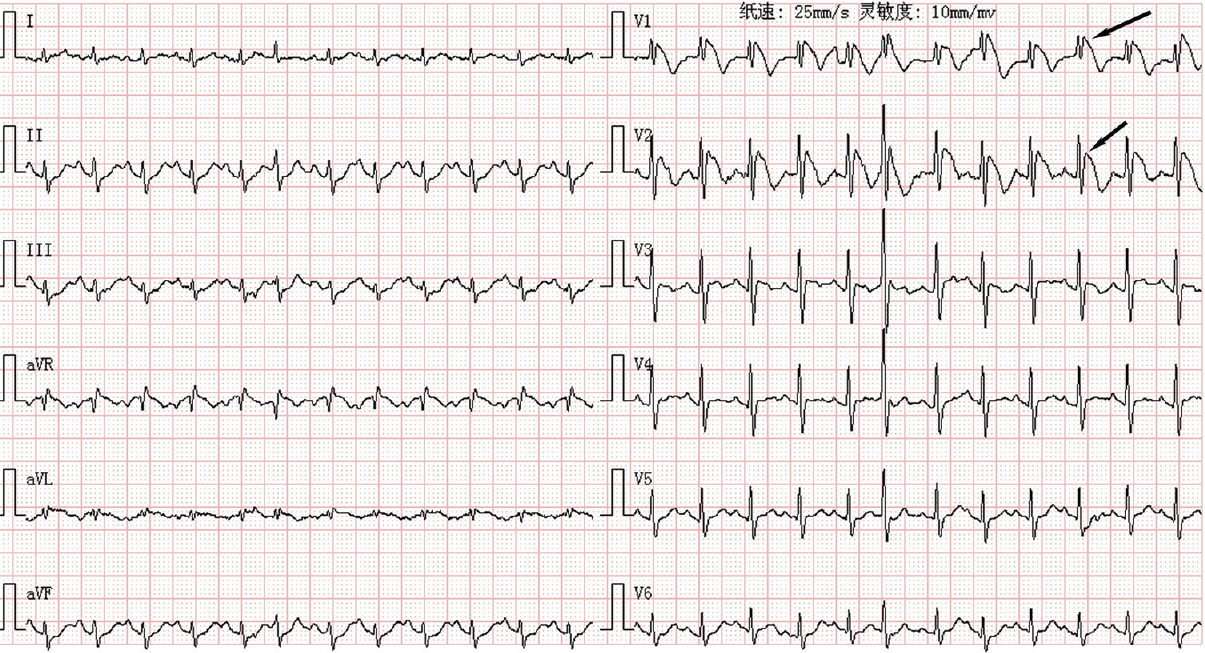
- Twelve-lead electrocardiography (ECG) when febrile. Note the pseudo-right bundle branch pattern and ‘coved’ ST-segment elevations in V1, V2 leads (arrows) consistent with a Type 1 Brugada pattern.

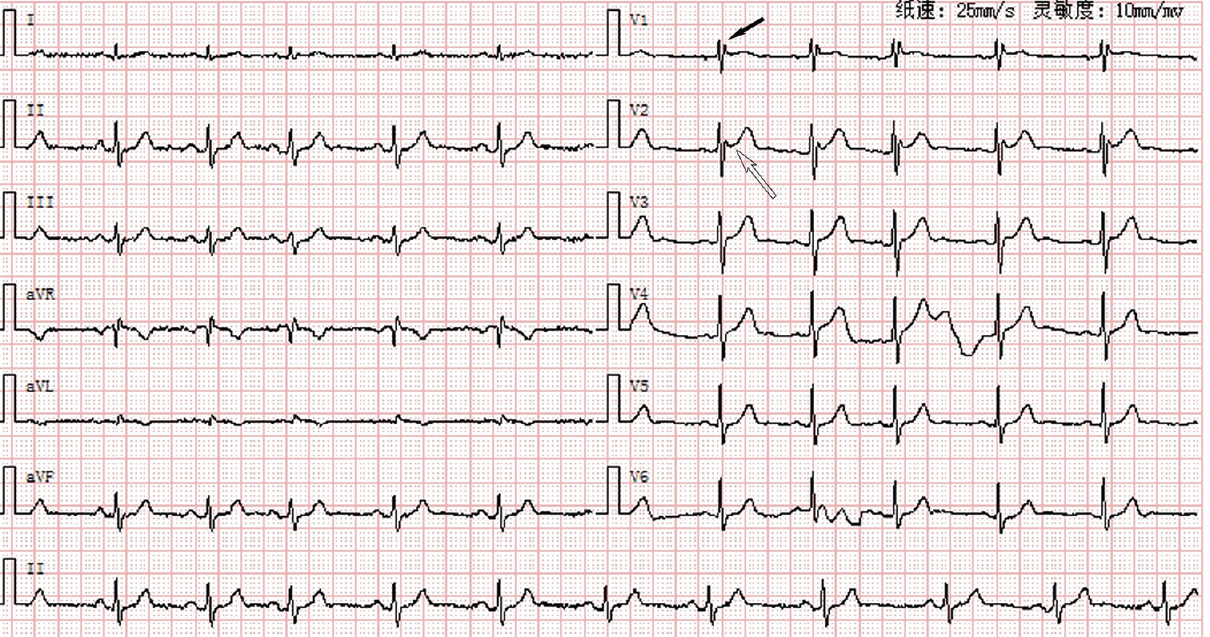
- Twelve-lead ECG when afebrile. Repeated ECG after resolution of fever was near normal, especially ST segment in V1, V2 leads (arrows).
The physical examination and the computed tomography of coronary angiogram were unremarkable. The 12-lead ECG at admission revealed a Type 2 Brugada pattern (Fig. 3). Programmed electrical stimulation could induce ventricular fibrillation (Fig. 4).
- Initial ECG on presentation several hours after syncope. Note the pseudo-right bundle branch block (solid black arrow) and the saddleback ST-segment elevation in V2 lead (hollow arrow) consistent with a Type 2 Brugada pattern.
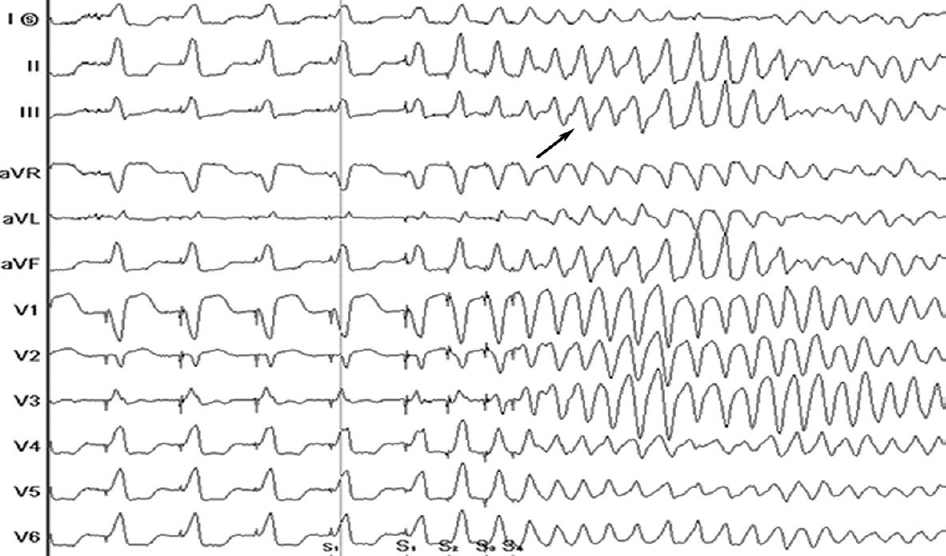
- Electrocardiography of induced ventricular fibrillation. Note the ventricular fibrillation (arrow) could be induced by vigorous programmed stimulation (S1S2S3S4, 500/300/300/250 ms) from the right ventricular apex. Defibrillation with 200 joules was successful.
The patient was initiated on cilostazol 50 mg twice a day per os administration and received an implantable cardioverter defibrillator (ICD). During the six-month follow up period, ECG was normal (Fig. 5), and the patient was uneventful, without recurrence of ventricular tachyarrhythmia at ICD controls.
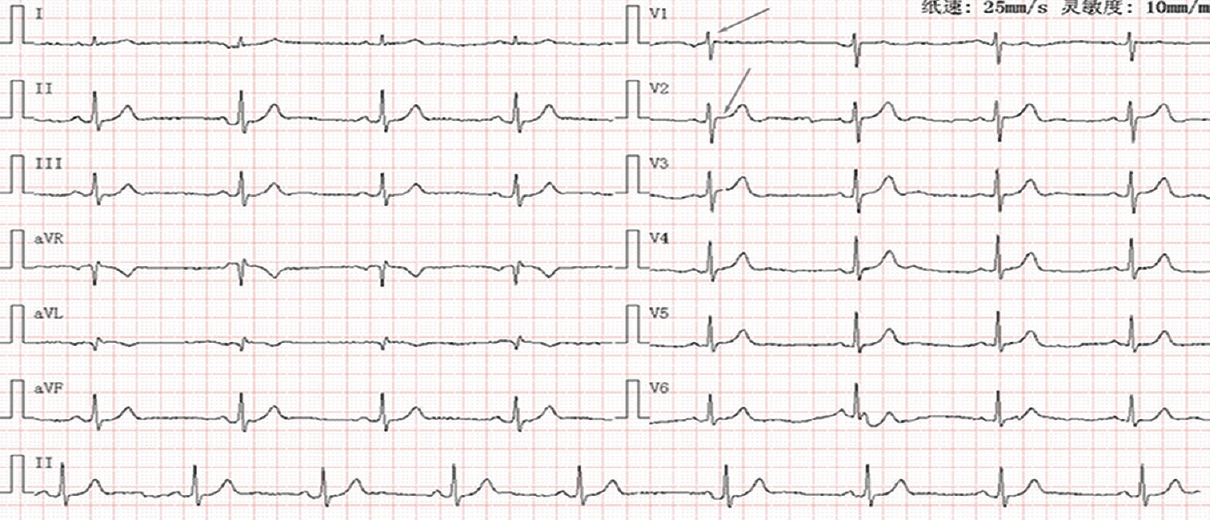
- Twelve-lead ECG during the follow up period. During the follow up period, repeated ECG was normal like, especially ST segment in V1, V2 leads (arrows).
Conflicts of Interest: None.




