Translate this page into:
A unique presentation of multiple myeloma in an HIV patient
*For correspondence: drsumi84@gmail.com
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 62 year old male, known case of HIV infection on HAART had first come to Department of Medicine, J.J. Hospital, Mumbai in 2009 with the complaint of depression felt over the scalp since last one year. His skull was shaved and an excavated area of 14 × 9 × 1.5 cm in size in the central region of the skull was seen (Fig. 1).

- Shaved head of the patient showing the central excavatory area. (A) Posterior view (B) Lateral view.
There were no other significant complaints or findings on examination. X-ray skull and CT scan brain showed lytic lesion (Fig. 2). Serum calcium, ESR and creatinine clearance were normal. Serum protein electrophoresis for M band and urine for bence jones proteins were negative. On immunofixation a faint band of IgG with monoclonal component was present. Bone marrow biopsy showed 3 per cent plasmacytosis. An osteolytic lesion at the lower end of the left humerus and right tibia was also found. The diagnosis made was symptomatic multiple myeloma, stage IIa (Durie Salmon).
Patient was treated with thalidomide (100 mg/day). Repeat imaging after 3 months showed resolution of the humerus and tibia lesion and a developing bony plate in the skull (Fig. 2).
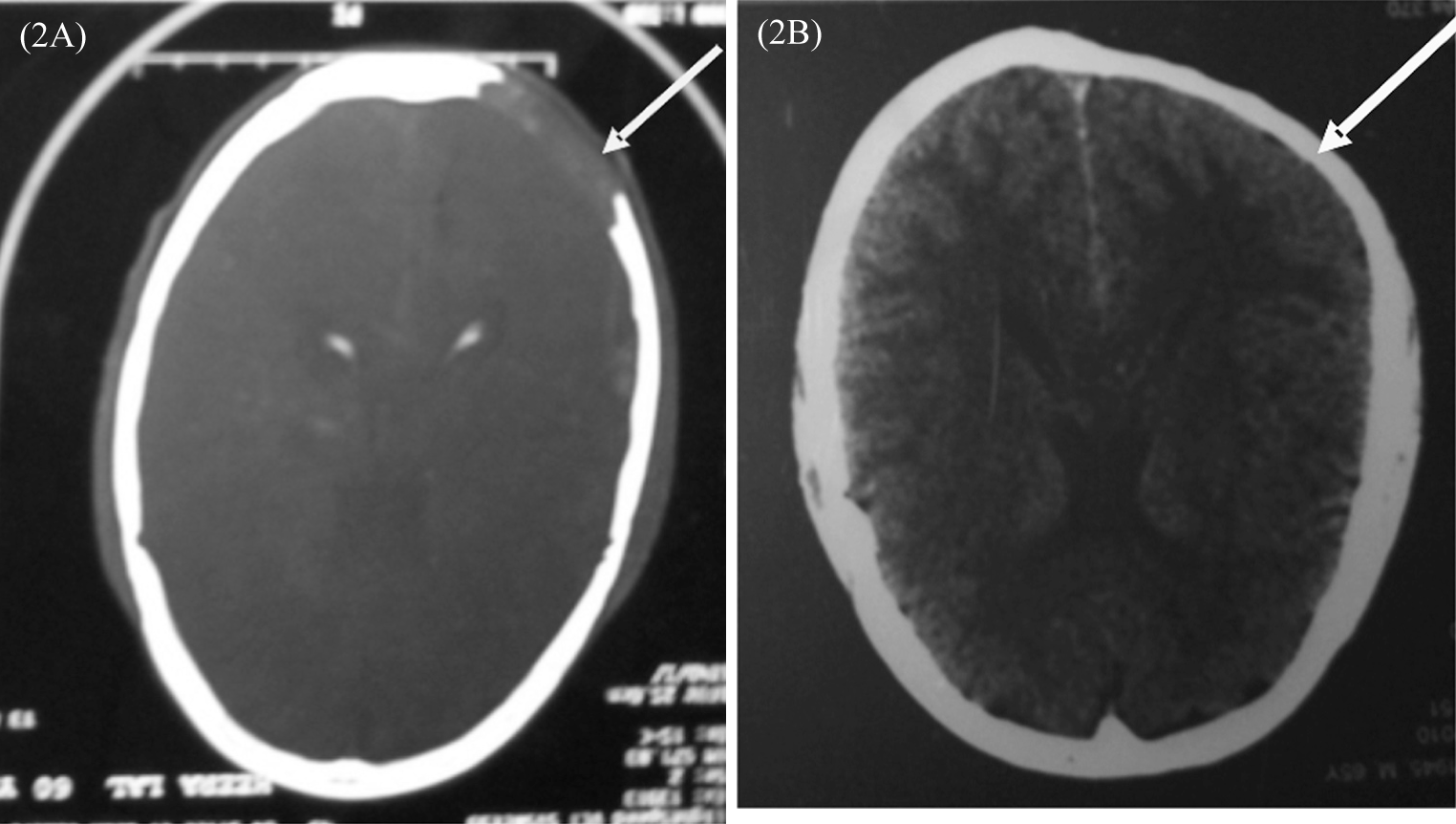
- CT Scan showing the lytic skull lesion and its resolution by thalidomide therapy.
Plasma cell disorders in HIV infected patients range from benign polyclonal hypergammaglonulinemia to indeterminate monoclonal gammopathy of unknown significance (MGUS) to malignant dyscrasias, including multiple myeloma and plasma cell leukemia. Hypergammaglobulinemia and oligoclonal banding had been the most frequently reported disorders in the pre-HAART era1. Though the optimal therapy for an HIV-infected person with plasma cell dyscrasia is yet to be defined, treatment with immunomodulatory agents (e.g. thalidomide) and proteasome inhibitors (e.g. bortezomib) may be worth considering1. Only a few cases of multiple myeloma with HIV with detailed treatment outcome have been reported2.
References
- Plasma cell disorders in HIV-infected patients: from benign gammopathy to multiple myeloma. AIDS Read. 2004;14:372-4.
- [Google Scholar]
- Thalidomide-based treatment for HIV-associated multiple myeloma: a case report. AIDS Read. 2003;13:383-9.
- [Google Scholar]




