
Translate this page into:
A rare case of meconium peritonitis
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 26 yr old primigravida† at 35 wk gestation presented to the department of Obstetrics & Gynaecology, Mahatma Gandhi Medical College & Research Institute, Puducherry, India, reported loss of foetal movement for one day. She had perceived reduced foetal movement (RFM) for the past two days. She was a booked patient with low risk and normal anomaly scan. Clinical examination revealed a symphysial fundal height of 32 cm, single live foetus, cephalic presentation and relaxed uterus. Ultrasound examination revealed oligohydramnios, foetal ascites, dilated bowel loops (Figs 1 and 2) and cardiotocography (CTG) – non-reassuring trace. An emergency caesarean section for foetal distress was carried out and the baby was ventilated postnatally. Ultrasound confirmed meconium peritonitis and the baby was operated on the second day of neonatal life. Intraoperative findings are shown in Figs 3 and 4. Jejunal resection with anastomosis was done. Mother and baby recovered well and were discharged on the eighth day postoperatively.
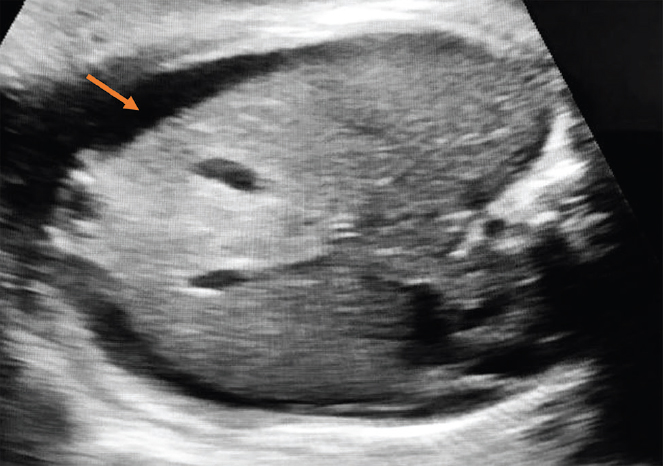
- Foetal ascites.

- Dilated bowel loop.
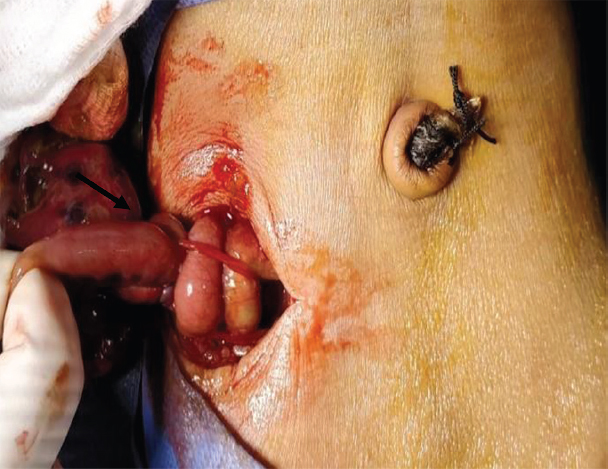
- Volvulus of jejunum.

- Jejunal perforation.
Maternal counselling for early reporting of any perceived abnormality of foetal movement can prevent stillbirths. Ultrasound should be performed as preliminary investigation along with CTG in evaluation of these women. Improved prenatal diagnosis and surgical management of meconium peritonitis will have increased survival rates.
Conflicts of Interest: None.




