
Translate this page into:
A rare case of fibrocalculous pancreatic diabetes with diabetic myonecrosis
*For correspondence: dayanidhi.meher@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 38 yr old female† presented to the Endocrinology outpatient department, Kalinga Institute of Medical Sciences, KIIT University, Bhubaneswar, India, on January 2018, with severe pain over left thigh, which was spontaneous and dull aching. She had diabetes for three years with poor glycaemic control (HbA1c=17.3 %) and was on oral anti-diabetic drugs. She had a history of intermittent abdominal pain without steatorrhoea since late childhood. On examination, there was a tender and indurated swelling over the anterolateral aspect of the left thigh. Nerve conduction study revealed axonal degeneration with severe sensory neuropathy. Ultrasonography of the pancreas showed parenchymal atrophy, ductal dilatation and intraductal calculi (Fig. 1). Ultrasound image of the left thigh showed hypoechoeic and enlarged adductor muscle (Fig. 2). Magnetic resonance imaging T2-weighted axial (Fig. 3) revealed oedema in the left thigh and focal enlargement and hyperintensity in the left adductor muscles. Section of the core biopsy from the quadriceps muscle showed the necrotic myofibres with intervening oedema (Fig. 4). Section with trichrome stain (Fig. 5) highlighted the necrotic and atrophic myofibres. Hence, final diagnosis of fibrocalculous pancreatic diabetes with diabetic myonecrosis was made. Myonecrosis in diabetes is not an uncommon complication but is grossly under-diagnosed, and improves with strict glycaemic control, analgesics, and anti-platelets. This patient was treated with above-mentioned therapy and improved within four weeks. At two-monthly follow up, the lesion had resolved clinically and there was no recurrence or appearance of new lesion during subsequent follow ups over the duration of one year.
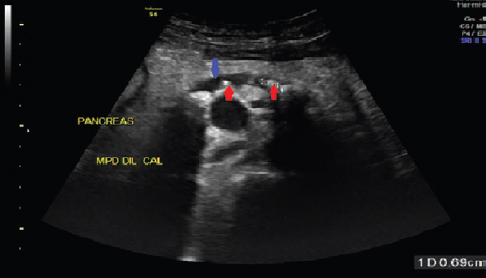
- Ultrasonography of the pancreas showing parenchymal atrophy, ductal dilatation (blue arrow) and intraductal calculi (red arrow).
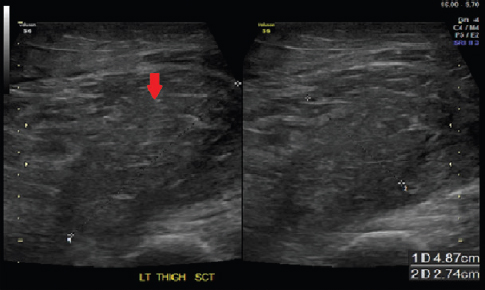
- Ultrasound image of the left thigh showing hypoechoeic and enlarged adductor muscle (red arrow).
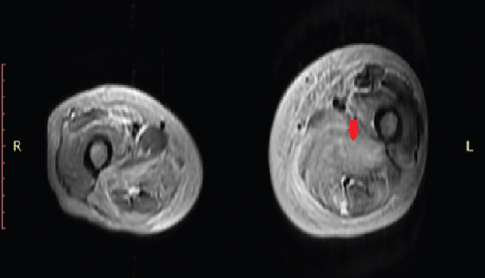
- MRI T2W Axial revealed edema in left thigh and focal enlargement and hyperintensity in the left adductor muscles (red arrow).
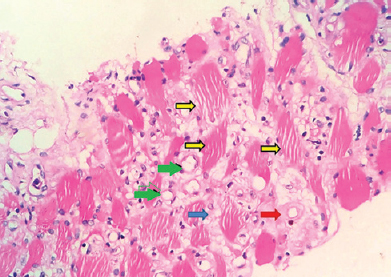
- Section of the core biopsy from the quadriceps muscle showing the necrotic myofibres (yellow arrows) with intervening oedema (blue arrows), mononuclear cell infiltrate, prominent thin-walled capillaries (green arrows) with perivascular hyalinization (red arrow) and areas of fibrosis (H and E stain, ×400)
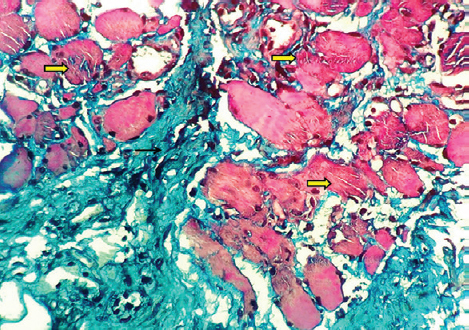
- Section with trichrome stain highlighting the necrotic and atrophic myofibres (thick yellow arrows) and intervening fibrosis (black arrows) (Masson trichrome, ×400).
Conflicts of Interest: None.




