Translate this page into:
A pilot study on real-time transvaginal ultrasonographic elastography of cystic ovarian lesions
Reprint requests: Dr Nazan Ciledag, Ankara Oncology Research & Education Hospital, Department of Radiology, 06460 Demetevler, Ankara, Turkey e-mail: drnazangokbayrak@yahoo.com.tr
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
This study was carried out to determine the appearance of various cystic ovarian lesions on transvaginal real-time ultrasonographic elastography and to investigate its potential in the differential diagnosis of cystic ovarian lesions.
Methods:
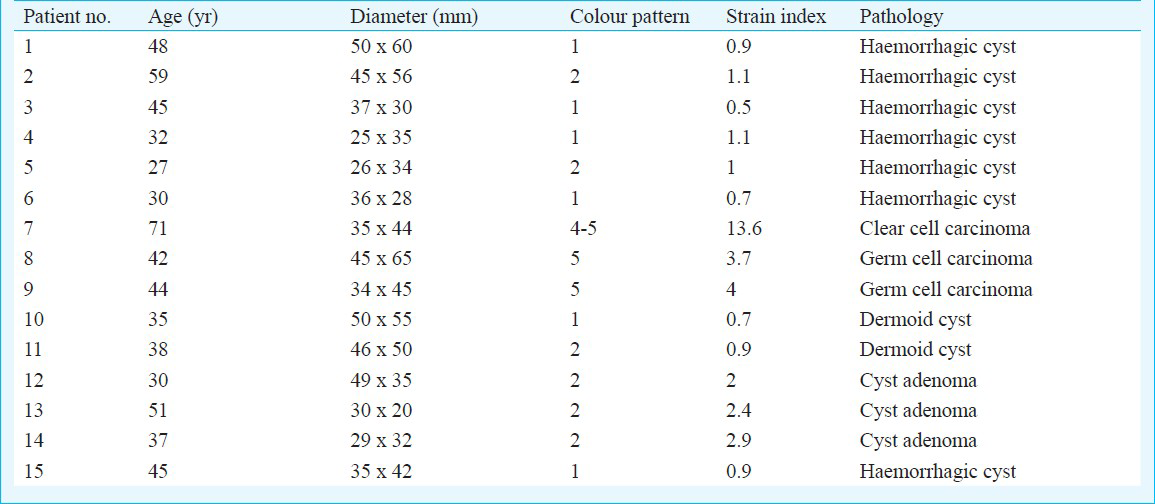
Twenty six women (age range, 27-71 yr; mean age 42 ± 16 yr) with cystic ovarian masses underwent transvaginal B-mode and Doppler ultrasonography, and transvaginal real-time ultrasonographic elastography. Those having ovarian cysts with solid components underwent to biopsy or surgical excision. The elasticity colour code (pattern 1-5), and strain index of cystic ovarian lesions were analyzed and associated with histopathological diagnosis.
Results:
Eleven of 26 ovarian cysts (42%) (diameter range, 3.2-4.5 cm) without solid component were not colour coded with blue or colour coded with blue-red-green heterogenous mosaic pattern. Fifteen of 26 cystic ovarian lesions (58%) (diameter range, 3.5-6.5 cm) had solid components. Among these, two had colour pattern 5, their strain indexes were 3.7 and 4, and their histopathologic diagnosis were germ cell carcinoma. One had colour pattern 5, with strain index 13.6, and histopathologic diagnosis was clear cell carcinoma.
Interpretation & conclusions:
Transvaginal real-time ultrasonographic elastography has potential role in the differential diagnosis of cystic ovarian lesions and this technique may be useful in differentiation of the benign lesions from those of malignant.
Keywords
Cyst
elastography
ovary
transvaginal ultrasound

Real-time ultrasonographic elastography is a method for dynamic imaging that displays tissue elasticity by measuring the degree of distortion by external compression, and decompression of the hardness of soft tissue as important indicator in the diagnosis of malignant lesions1. Elastographic colour codes are created by comparing ultrasonographic echo data obtained before and after a slight compression of tissue. Elastography was first introduced for diagnosis of malign breast lesions by Ophir et al in 19911. Several studies have been performed using real-time elastography on various tissues123456789101112, but there is no report on transvaginal real-time elastographic application with US in the differential diagnosis of cystic ovarian lesions. The purpose of the present study was therefore, to determine the appearance of various cystic ovarian lesions on transvaginal real-time ultrasonographic elastography and to investigate the potential role of this technique in the differential diagnosis of cystic ovarian lesions to decrease unnecessary biopsies and select the most suitable area before biopsy.
Material & Methods
Patients: Between February and April 2009, consecutive 26 women (age, ranging from 27 to 71 yr; mean, 42 ± 16 yr) in Ankara Oncology Research and Education Hospital with cystic ovarian mass who underwent transvaginal B-mode US, Spectral Doppler US, and transvaginal real-time ultrasonographic elastography (Hitachi EUB-5500) with transvaginal 7.5 MHz transducer were enrolled in the study. The study protocol was approved by institutional review board, and each patient gave written informed consent. Ovarian cysts with solid component were biopsied or surgically excised, yielding a histopathological diagnosis.
Technique and evaluation criteria: For each ovarian cyst, transvaginal B-mode and spectral Doppler images were first obtained. Their diameter, shape, location, and resistivity index (RI) of the solid components were analyzed. Then, the system was changed into the elastography mode and real-time free-hand elastography was performed using the same probe for additional two minutes. For elastography, compression was applied in upward and downward directions along the radiation axis of the target lesion. This light pressure was followed by decompression and repeated until a stable image of the target area was obtained. Real-time elastographic and B-mode images simultaneously appeared as a two-panel image. Elastogram appeared in the region of interest (ROI) box to determine the target ovarian lesion and surrounding tissue, then elasticity colour code was classified in 5 patterns2 : pattern 1, an absent or a very small hard area; pattern 2, hard area <45 per cent; pattern 3, hard area >45 per cent; pattern 4, peripheral hard and central soft areas; pattern 5, hard area occupying entire solid component with or without soft rim. Strain index was analyzed, which was obtained by comparing the absolute strain value of solid component of ovarian cyst with that of surrounding soft tissue.
The transvaginal ultrasonography, Doppler ultrasonography and real time transvaginal ultrasonographic elastography of all patients were performed before and blinded to the histopathological diagnosis of the patients. Histopathological results of biopsy or surgical excision specimen were correlated with ultrasonographic and elastographic results. The real-time transvaginal ultrasonographic elastography findings of masses with pattern 3-5 were considered as malignant and pattern 1 or 2 were accepted as benign23. The negative and positive predictive values of technique could not be evaluated because of the small number of samples. All patients were followed up with US for at least 12 months.
Results
Eleven of 26 ovarian cysts (42%) (diameter ranging from 3.2 to 4.5 cm) without solid component were not colour coded with blue representing hard area (n=7) (Fig. 1) or colour coded with blue-red-green heterogeneous mosaic pattern (n=4).

- Right ovarian cyst with multiple septum were not colour coded on elastogram, histopathologic evaluation revealed benign cyst.
Fifteen of 26 cystic ovarian lesions (58%) (diameter ranging from 3.5 to 6.5 cm) had solid components (Table). Among solid components, three lesions whose RI was 0.7 had colour pattern 2, with strain index 2, 2.4, and 2.9, and histopathologic diagnosis was cyst adenoma (Fig. 2), seven lesions with RI 0.6 had colour pattern 1 (n=4) or 2 (n=3), with strain index between 0.9-1.1, and histopathologic diagnosis was haemorrhagic cyst, two lesions with RI 0.6 had colour pattern 1, their strain indices were 0.7 and 0.9, and histopathologic diagnosis was dermoid cyst (Fig. 3), two lesions whose RI was 0.9 had colour pattern 5 (strain index 3.7 and 4) with histopathologic diagnosis germ cell carcinoma, and the last one with RI 0.4 had colour pattern 5, strain index 13, and histopathologic diagnosis was clear cell carcinoma (Fig. 4).
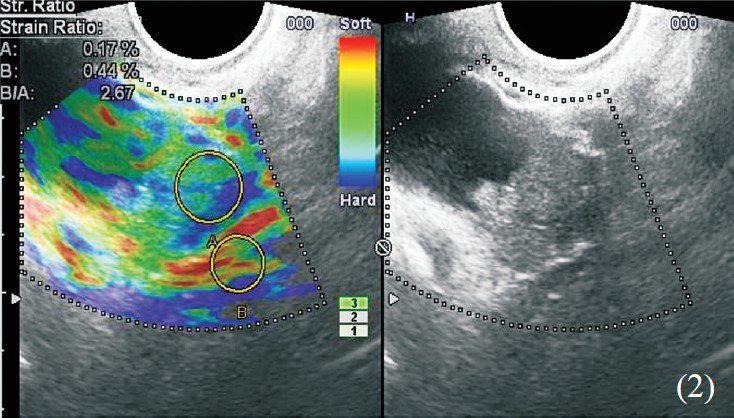
- Left ovarian cyst with solid nodular component, coded type 2 colour pattern on elastogram, histopathologic evaluation revealed cyst adenoma.
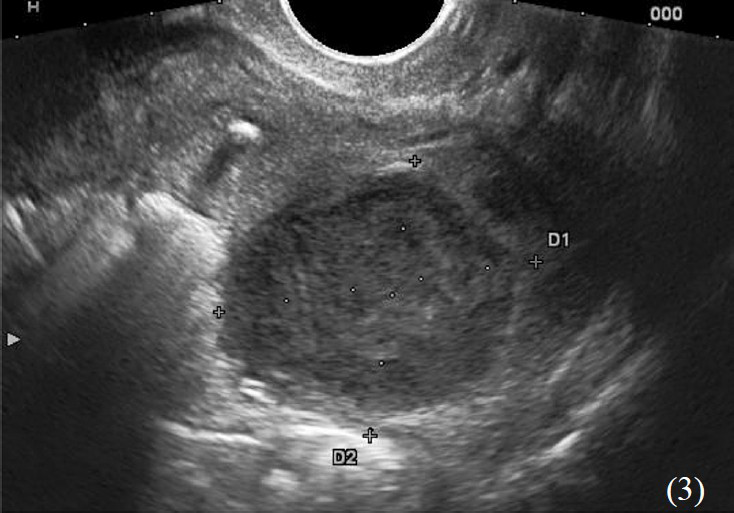
- B-mode ultrasonography of ovarian cyst with heterogeneous components, histopathologic evaluation revealed dermoid cyst.
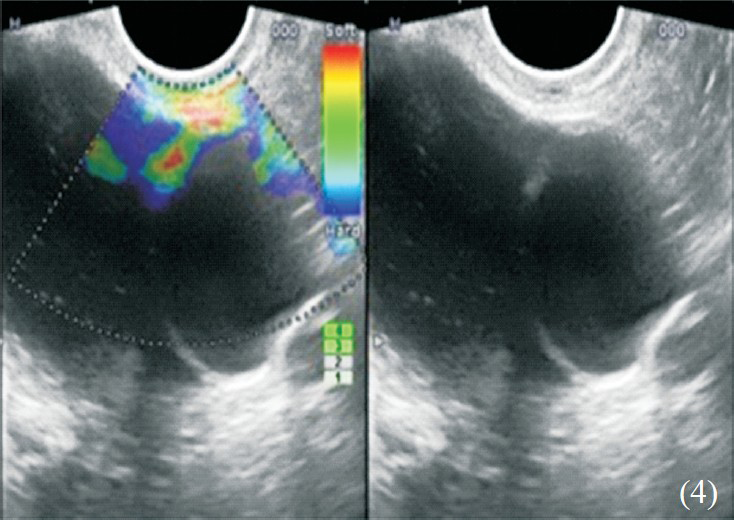
- Ovarian cyst with solid nodular components, coded type 5 colour pattern on elastogram, histopathologic evaluation revealed clear cell carcinoma.
Among 15 lesions investigated by elastograpy, 12 were evaluated as benign and the remaining three as malignant due to real-time transvaginal ultrasonographic elastographic results. This finding was confirmed by histopathologic results.
Discussion
Real-time ultrasonographic elastography has been used via conventional or other (transvaginal, endoscopic, so forth) US methods to examine several organs such as; pancreas34, lymph nodes23, breast567, thyroid8, prostate910, cervix11, and liver12. The sensitivity and the specificity of transvaginal ultrasonography differs from 80 to 90 per cent in different studies1314. Sokalska et al15 reported a sensitivity of 86 per cent for the diagnosis of teratoma or dermoid cyst, and the highest sensitivity of 11 per cent for benign ovarian tumours (cyst adenomas). They suggested that B-mode ultrasound and Doppler ultrasound imaging may be almost conclusive diagnostic for dermoid cyst, endometrioma or hydrosalpinx, but other adnexial pathologies can only be recognized with these techniques without confirmation.
In this study we aimed to evaluate the appearance of various cystic ovarian lesions on transvaginal real-time ultrasonographic elastography and to investigate the potential value of transvaginal real-time ultrasonographic elastographic colour pattern and strain index in the differential diagnosis of cystic ovarian lesions with solid components. Real-time ultrasonographic elastography has some advantages over off-line elastography: it is easy to perform, and does not require more than 3-5 min. It can provide dynamic visualization of the ovarian lesion during compression and be virtually used in cystic ovarian masses with solid components. The scoring system used in this study was similar to that used by Alam et al2, where scores 1 and 2 were considered benign; score 3 intermediate risk for malignancy, and 4 and 5 were suggestive of malignancy. Though we could not determine positive or negative predictive values or sensitivity and specifity of this technique due to small number of cases, we found that all lesions evaluated as benign or malignant with elastographic findings were confirmed by histopathologic examination. Hence, the unnecessary surgical procedures can be prevented with this technique.
The main limitation of our study was the small sample number as an initial experience and further investigation on larger series in multiple centers is needed. Real-time transvaginal ultrasonographic elastography needs experienced operators to perform light pressure for elastographic evaluation because strong pressure may lead to misdiagnosis. The strain indices of cystic ovarian lesions could not be compared with those of the literature because of absence of these reference values. Also, whether the cyst variously affects on strain index of solid component is another dilemma, although we could not detect this negative effect. So, further studies are needed for these questions.
In conclusion, real-time ultrasonographic elastography can reduce unnecessary invasive procedures for the differential diagnosis of benign and malignant cystic ovarian lesions with solid components. Also, it may help to select the suitable region of the lesion for biopsy.
References
- Elastography: a method for imaging the elasticity in biological tissues. Ultrason Imaging. 1991;13:111-34.
- [Google Scholar]
- Accuracy of sonographic elastography in the differential diagnosis of enlarged cervical lymph nodes: Comparison with conventional B-mode sonography. AJR. 2008;191:604-10.
- [Google Scholar]
- Endoscopic ultrasound elastography for evaluation of lymph nodes and pancreatic masses: a multicenter study. World J Gastroenterol. 2009;15:1587-93.
- [Google Scholar]
- Diagnosis of pancreatic disorders using contrast-enhanced endoscopic ultrasonography and endoscopic elastography. Clin Gastroenterol Hepatol (11 Suppl):S63-7.
- [Google Scholar]
- Elastography of breast lesions: initial clinical results. Radiology. 1997;202:79-86.
- [Google Scholar]
- Breast disease: clinical application of US elastography for diagnosis. Radiology. 2006;239:341-50.
- [Google Scholar]
- Real-time elastography: an advanced method of ultrasound - first results in 108 patients with breast lesions. Ultrasound Obstet Gynecol. 2006;28:335-40.
- [Google Scholar]
- Prostate cancer: three-dimensional sonoelastography for in vitro detection. Radiology. 2005;237:981-5.
- [Google Scholar]
- Real-time sonoelastography of the cervix: tissue elasticity of the normal and abnormal cervix. Acad Radiol. 2007;14:193-200.
- [Google Scholar]
- Real-time elastography for noninvasive assessment of liver fibrosis in chronic viral hepatitis. AJR. 2007;188:758-64.
- [Google Scholar]
- Doppler ultrasonography in the diagnosis of ovarian cysts: indications, pertinence and diagnostic criteria. J Gynecol Obstet Biol Reprod (Paris). 2001;30(1 Suppl):S20-33.
- [Google Scholar]
- Transvaginal sonographic characterization of ovarian disease:evalution of a new scoring system to predict ovarian malignancy. Obstet Gynecol. 1991;78:70-6.
- [Google Scholar]
- Diagnostic accuracy of transvaginal examination for assigning a specific diagnosis to adnexal masses. Ultrasound Obstet Gynecol. 2009;34:462-70.
- [Google Scholar]




