Translate this page into:
A hospital based study on reference range of serum prostate specific antigen levels
Reprint requests: Dr Aditi Gupta, Clinical Lab Services, Medanta-The Medicity, Sector 38, Gurgaon 122 001, India e-mail: aditi.jindel@gmail.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Serum prostate specific antigen (PSA) levels are known to vary with race and ethnicity, environmental factors, lifestyle, metabolic and physiologic changes and advancing age. This study was designed to determine age specific serum PSA level in healthy Indian men and its comparison with that reported in different populations of the world.
Methods:
A total of 1300 adult men who attended Executive Health Check-up programme in a tertiary care hospital in Haryana, India, were included in the study. Forty seven men were excluded from the analysis because of urological conditions affecting PSA values. Overall, 1253 men were analyzed for age specific PSA values.
Results:
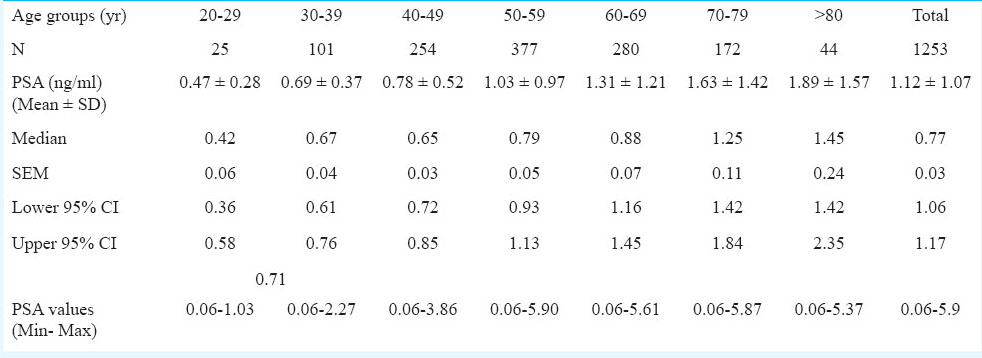
The age specific reference range of serum PSA values was 0.71 ng/ml in those younger than 40 yr; 0.85 ng/ml in 40-49 yr; 1.13ng/ml in 50-59 yr group; 1.45 ng/ml in 60-69 yr group; 1.84 ng/ml in 70-79 yr group and 2.35 ng/ml in men older than 80 yr.
Interpretation & conclusions:
Our study provided the age-specific reference range of serum PSA in healthy men in India. The data suggested that the PSA levels were associated with increasing age.
Keywords
Age specific PSA
healthy men
prostate specific antigen
reference range

Prostate cancer (PC) is the second most common non-dermatological malignancy, frequently diagnosed in men. The incidence of PC has increased rapidly in most Asian countries over the past two decades1. PSA (prostate specific antigen) is one of the most valuable tools for the screening and diagnosing prostate cancer in men. PSA is an androgen regulated serine protease produced primarily by prostate ductal and acinar epithelium as an inactive 244 amino acid pro-enzyme (pro PSA) that is activated by cleavage of seven N- terminal amino acids and then secreted into lumen2. It is organ-specific but not disease-specific, and can be detected in patients with normal prostate and benign prostatic hyperplasia (BPH), and in both primary and metastatic prostate cancer cells3.
Globally, the 95th percentile value (normal upper limit) of serum PSA (4.0 ng/ml) is not always accurate for all ages4. It has been suggested that age specific cut-off values for PSA screening are better compared than the currently used single cut-off of 4.0 ng/ml5. Age specific reference ranges for PSA were first presented from a community based population of 471 healthy American white men by Oesterling et al6. Several studies conducted in India have reported that the serum PSA level varies with different geographical areas, age and ethnicity78.
Standard reference intervals of serum PSA level in Indian men without prostate diseases are not available and the values in use are the reference range reported in the world literature. Therefore, it is desirable to generate reference range of serum PSA levels for healthy Indian men. This study was a step to establish age specific reference range of serum PSA in healthy Indian men and to compare this range with that reported in world literature.
Material & Methods
The present study was conducted in a multispecialty hospital in Gurgaon, Haryana, India, over a period of two years from January 2010 to January 2012. During this period, approximately 1300 men were enrolled in the Executive Health Check-up pragramme and they opted to undergo serum PSA test. Of the1300 men, 1253 men in the age group between 19-97 yr were selected for the study after excluding the subjects as per appropriate exclusion criteria defined by International Federation of Clinical Chemistry (IFCC)9. Apart from this, men having some urological complications (22), post-operation of prostate gland or history of prostate diseases (15) were excluded from the present study. Further, those taking any chemotherapy or radiotherapy and anti androgen drugs (7) were also excluded. Men having pus cell more than 4 in urine analysis (3) were also excluded.
The subjects were divided as per age group: <40 yr (n = 126), 40-49 yr (n = 254), 50-59 yr (n = 377), 60-69 yr (n = 280), 70-79 yr (n = 172) and above 80 yr (n = 44). Blood samples (5 ml) were collected10 and serum was separated. Samples were assayed by using an immunometric assay technique (VITROS 5600 Clinical Chemistry Analyzer, USA) based on chemiluminescence method. All samples were analyzed in the same laboratory to prevent the variations in measurement. A comprehensive internal quality control programme was followed and results were released after calibrating values between mean ±1SD. This internal quality control analysis was performed daily.
Statistical analysis: Statistical analysis was done using SPSS (SPSS V. 16, IBM, USA) software. Data were analyzed using student t test; P<0.05 was considered significant. Confidence intervals (CI, low-high), mean, median, SEM were also calculated. Confidence intervals low represented 5th percentile value while CI high represented 95th percentile value for each age groups.
Results & Discussion
The results of serum PSA levels in 1253 healthy men as per age group from <40 to > 80 yr are shown in Table I. The range of serum PSA values in healthy men was 0.06-5.90 ng/ml. The analytical sensitivity of the test was 0.03 ng/ml. The mean serum PSA values was 0.64 + 0.37 ng/ml in those younger than 40 yr; 0.78 + 0.52 ng/ml in 40-49 yr; 1.03 +0.97 ng/ml in 50-59 yr group; 1.31 + 1.21 ng/ml in 60-69 yr group; 1.63 + 1.42 ng/ml in 70-79 yr group and 1.89+ 1.57 ng/ml in men older than 80 yr. Age-wise distribution of serum PSA in the entire study group is shown in Fig. 1. There was a progressive increase in mean and 95% CI values with advancing age from below 40 yr to above 80 yr (Fig. 2).
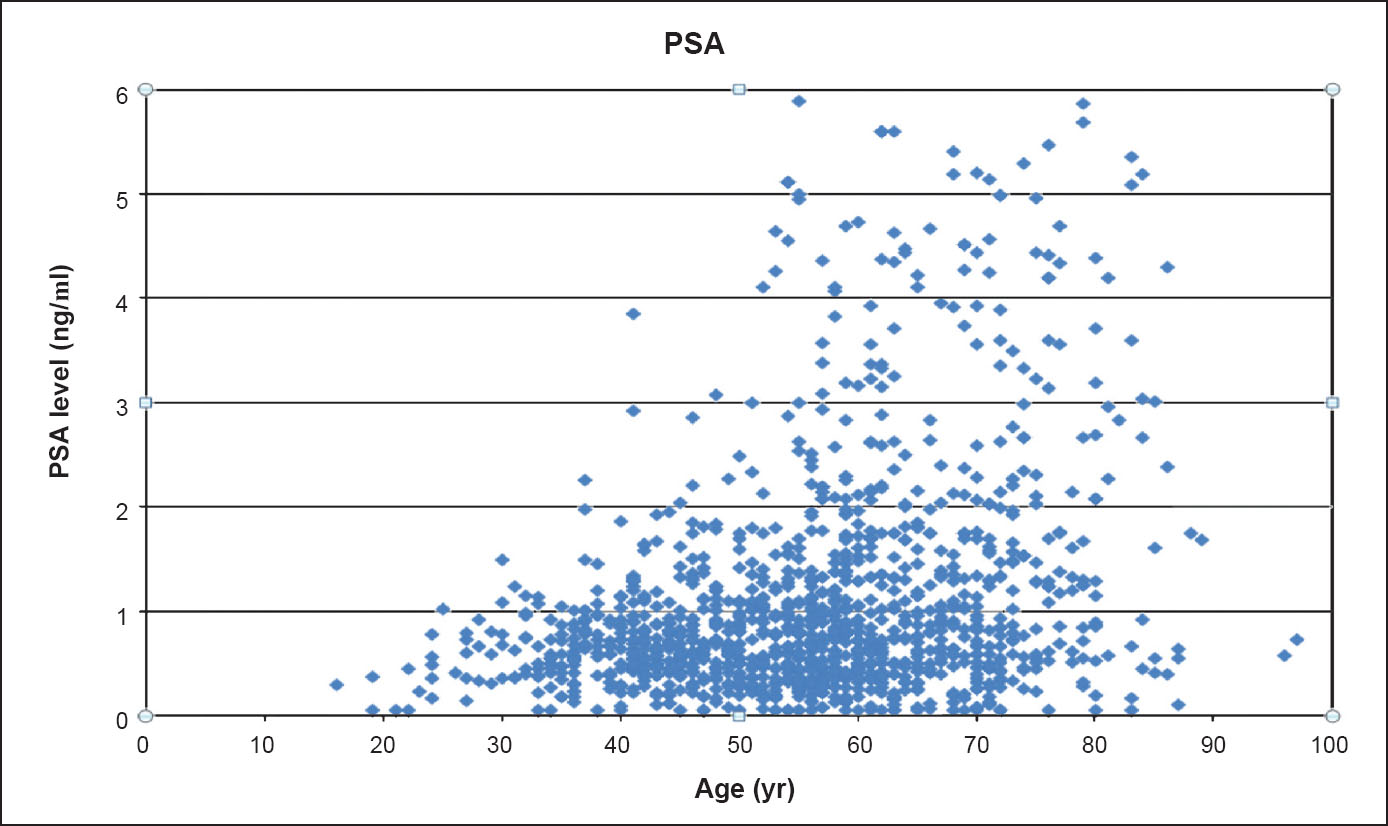
- Distribution of serum PSAvalue (ng/ml) with advancing age group (year).
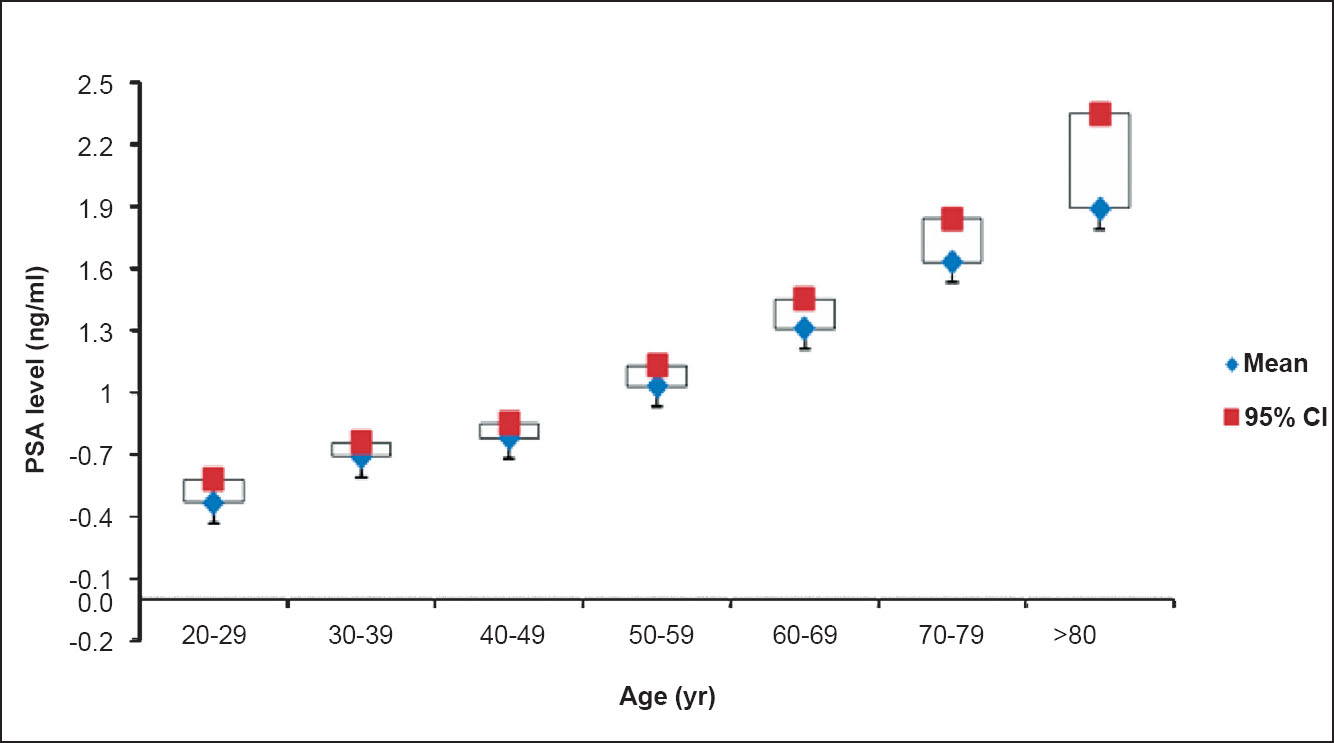
- Mean and 95% confidence interval (CI) of PSA levels (ng/ml) with ascending age groups (years).
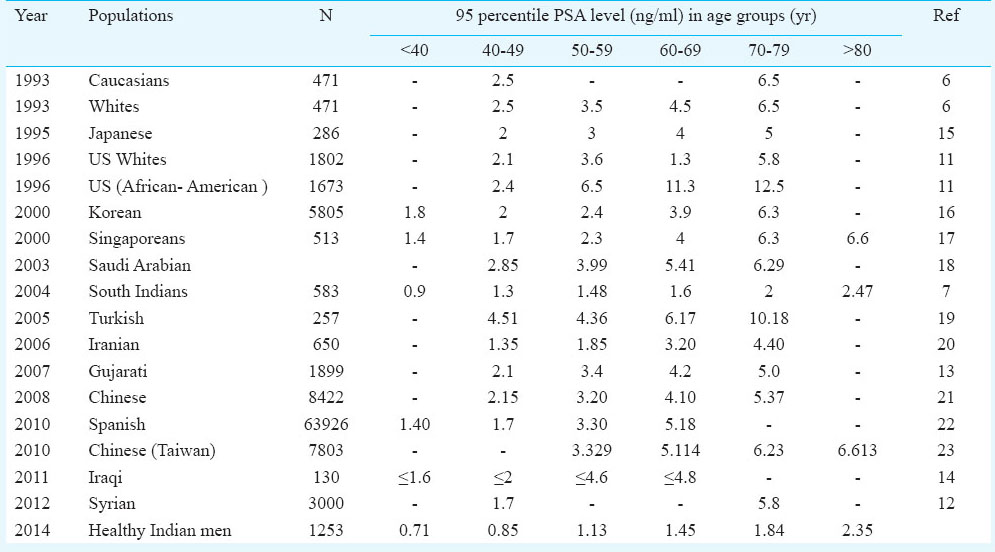
Comparison of the results of present study with other studies indicated that the normal level of serum PSA in our study subjects was lower than that of US, African, American, Turkish, Japanese, Chinese, Spanish, Iranian, Singaporeans, Syrian and Korean men (Table II). Asian men have been shown to have lower PSA level than other races (African & American)11. It may be due to lower levels of androgen in Asian men but there have not been any studies investigating this. Sutclifee et al24 conducted a study on a young male Caucasian African – American members of the US military and reported that the PSA levels was significantly higher in African-than in Caucasian - American men. Pradhananga et al25 have reported lower PC rates in Nepal compared to India and Pakistan. A study conducted in south Indian men suggested that the mean serum PSA levels of south Indian men were slightly higher as compared to men from Korea but slightly lower than American men7. Another study from Syria correlated serum total PSA levels with age and concluded that Syrian men had lower PSA values compared with other races12. In our study, it was found that 95th percentile of serum PSA level in healthy men was 1.17 ng/ml that was slightly lower than healthy Gujarati men, south Indian men (1.51 ng/ml) and other regions for all age groups (Table II).
Age is one of the key risk factors for the prostate disease; with the increase in the age, susceptibility towards the disease also increases8. For a healthy 60 yr old man with no evidence of prostate cancer, the serum PSA concentration increases by approximately 3.2 per cent per year (0.04 ng/ml)6. Oesterling et al6 have reported that the serum PSA concentration is directly correlated with patient age rather than rely on a single reference range for men of all age groups. They concluded that the age specific reference ranges for serum PSA were lower in Japanese men living in a small fishing village of Japan than for similarly aged white men. This may be either due to inherited susceptibility associated with genetic factors or other factors that are influencing serum PSA level like race and ethnicity, difference in lifestyle characterized by dietary habits and physical expenditure. Morgan et al11 reported that the serum PSA concentration directly correlated with advancing age in a large study population of African-American men. Lim et al26 have conducted a study on healthy multiethnic Asian population (Malay, Chinese and Indian men) and their findings support the concept that the baseline PSA level varies between different ethnicities across all age groups. Therefore, age précised PSA values should also be applicable for Indian population.
Chia and colleagues27 conducted a community based study in Singapore which concluded that the mean PSA levels in the Chinese, Malays and Indian ethnic groups in Singapore were positively associated with age and were lower than PSA levels of the white population in the USA. A study done on serum PSA levels in a community-based population of Gujarat concluded that age specific PSA ranges were on the lower side and the prostate specific antigen density on the higher side13. This study also concluded that 89.17 per cent had a PSA of <4 ng/ml, 8.9 per cent had a PSA between 4-10 ng/ml, while 1.8 per cent had a PSA more than 10 ng/ml.
Belbase et al28 in their study on prostate cancer in a healthy population group in Eastern Nepal, reported that the sensitivity of PSA more than 4 ng/ml in detecting carcinoma prostate was 100 per cent and the positive predictive value for serum PSA was 19.0 per cent. Hailam et al14 reported that the serum PSA measurement in Iraqi men was maximum at 4.8 ng/ml, was slightly more than the international standard threshold of 4.0 ng/ml. Agnihotri et al29 conducted a study on 4702 patients for defining the cut-off value of PSA for biopsy in symptomatic Indian men and concluded that 70.9 per cent had PSA of <4 ng/ml and 29.1 per cent had PSA of >4 ng/ml.
In our study, the normal upper limit of serum PSA level in healthy men was 1.17 ng/ml which was considerably lower than the international standard reference range of 4.0 ng/ml. The mean PSA level of healthy men was 1.12 ng/ml which was lower than that of healthy Gujarati and south Indian men (1.4 ng/ml). The men were distributed into six age groups (<40 to >80 yr) to see the upper limit of normal range (95th percentile) across the different age groups which increased from 0.71 to 2.35 ng/ml with advancing age group.
There were certain limitations of this study as information on TRUS (trans rectal ultrasound) findings about prostate size and abnormality was not available and no prostate biopsy was done in any of the participants, because the participants were apparently healthy men who opted for this test as a part of regular health check-up.
In summary, there is need to have separate age specific reference ranges of serum PSA for Indian men. Our findings showed lower age-specific serum PSA ranges for healthy Indian men compared to certain other populations of the world. The study has also confirmed that serum PSA correlates with advancing ages.
Acknowledgment
The authors acknowledge the contributions of Bhavana Alapati and Dr Padam Singh for their guidance in statistical analysis of this manuscript.
References
- Usefulness of prostatic specific antigen (PSA) for diagnosis and staging of patients with prostate cancer. Arch Espl Urol. 2011;8:659-80.
- [Google Scholar]
- Risk of prostate cancer for young men with a prostate specific antigen less than their age specific median. Urol J. 2007;177:1745-8.
- [Google Scholar]
- Serum prostate-specific antigen in a community-based population of healthy men: establishment of age-specific reference ranges. JAMA. 1993;270:860-4.
- [Google Scholar]
- Racial and ethnic variation of PSA in global population: Age specific reference intervals for serum prostate specific antigen in healthy South Indian males. Indian J Clin Biochem. 2004;19:132-7.
- [Google Scholar]
- Effects of aging and ethnicity on serum free prostate specific antigen. Asian Pacific J Cancer Prev. 2011;12:2509-12.
- [Google Scholar]
- International Federation of Clinical Chemistry (IFCC), Scientific Committee, Clinical Section, Expert Panel on Theory of Reference Values. Approved Recommendation on the Theory of Reference values. Part 2. Selection of individuals for the production of reference values. J Clin Chem Clin Biochem. 1987;25:639-44.
- [Google Scholar]
- Clinical and Laboratory Standard Institute (CLSI). Procedures for the collection of diagnostic blood specimens by venipunture; Approved Standard. (6th ed). Wayne, Pennsylvania, USA: CLSI; 2007.
- [Google Scholar]
- Age specific reference ranges for serum prostate specific antigen in black men. N Engl J Med. 1996;335:304-10.
- [Google Scholar]
- Age specific reference ranges for prostate specific antigen among healthy Syrian men. Int J Biol Markers. 2012;27:152-9.
- [Google Scholar]
- Age-specific prostate specific antigen and prostate specific antigen density values in a community-based Indian population. Indian J Urol. 2007;23:122-5.
- [Google Scholar]
- Age specific reference ranges of serum prostate specific antigen in Iraqi men. Arab J Urol. 2011;9:273-7.
- [Google Scholar]
- Serum prostate-specific antigen in a community based population of healthy Japanese men: lower values than for similarly aged white men. Br J Urol. 1995;75:347-53.
- [Google Scholar]
- Ethnic differences in the age related distribution of serum prostate-specific antigen values: a study in healthy Korean population. Urology. 2000;56:1007-10.
- [Google Scholar]
- Age-related reference intervals for free and total prostate specific antigen in a Singaporean population. Pathology. 2000;32:245-9.
- [Google Scholar]
- Prostate specific antigen reference ranges in Saudi men. Saudi Med J. 2003;24:665-8.
- [Google Scholar]
- Population standards of prostate specific antigen values in men over 40: community based study in Turkey. Int Urol Nephrol. 2005;37:299-304.
- [Google Scholar]
- Analysis of serum prostate-specific antigen levels in men aged 40 years and older in yasuj. Iran Urol J. 2005;2:189-92.
- [Google Scholar]
- Age specific PSA reference ranges in Chinese men without prostate cancer. Asian J Androl. 2009;11:100-3.
- [Google Scholar]
- Reference values of prostate specific antigen (PSA) in 63926 workers without prostatic symptoms who participated in prostate screening cancer developed by the Ibermutuamur Prevention Society in 2006. Actas Urol Esp. 2010;34:669-76.
- [Google Scholar]
- Age related reference levels of serum prostate specific antigen among Taiwanese men without clinical evidence of prostate cancer. Chang Guang Med J. 2010;33:182-7.
- [Google Scholar]
- Prostate-specific antigen concentration in young men: new estimates and review of literature. Br J Urol Int. 2012;110:1627-35.
- [Google Scholar]
- Multi-institution hospital based cancer incidence data for Nepal - An initial report. Asian Pacific J Cancer Prev. 2009;10:259-62.
- [Google Scholar]
- Ethnicity is an independent determinant of age-specific PSA level: findings from a multiethnic Asian setting. PLoS one. 2014;9:e104917.
- [Google Scholar]
- Prostate specific antigen levels among Chinese, Malays and Indians in Singapore from a community based study. Asian Pac J Cancer Prev. 2007;8:375-8.
- [Google Scholar]
- Prostate cancer screening in a healthy population cohort in Eastern Nepal: an explanatory trial study. Asian Pacific J Cancer Prev. 2013;14:2835-8.
- [Google Scholar]
- Raising cut-off value of prostate specific antigen (PSA) for biopsy in symptomatic men in India to reduce unnecessary biopsy. Indian J Med Res. 2014;139:851-6.
- [Google Scholar]




