
Translate this page into:
A case of repeated misdiagnosis of amyloid cardiomyopathy
*For correspondence: fengxiangfei@xinhuamed.com.cn
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 65 yr old woman† was transferred to the department of Cardiology, Xinhua hospital, Shanghai, China in September 2018 due to slowly progressive dyspnoea over a 12 month period. She was previously diagnosed with variable angina with dilated cardiomyopathy or pericardial effusion, however, the prescribed diltiazem, furosemide, or spironolactone did not seem to have worked well. Her electrocardiogram showed significant peripheral low-voltage QRS and transthoracic echocardiogram showed diffuse hyper-refractile ‘granular sparkling’ appearance (Fig. 1), apart from left ventricular dysfunction and pericardial effusion. Cardiac magnetic resonance imaging using phase-sensitive inversion recovery showed global subendocardial late gadolinium enhancement typically seen in light chain amyloidosis (Fig. 2). Free light chain κ and λ levels were elevated in serum and urine, respectively, which further confirmed the above diagnosis. Abdominal skin biopsy also showed a pathognomonic yellow-green birefringence under polarized light. Other investigations, such as coronary computed tomography (CT) angiography (mild stenosis), bone marrow biopsy (slight plasmacytosis) and abdominal fat aspirate (negative Congo red staining) were of little diagnostic value. The patient was treated with bortezomib and dexamethasone. At six month follow up, some improvement was found in her symptoms and lung CT.
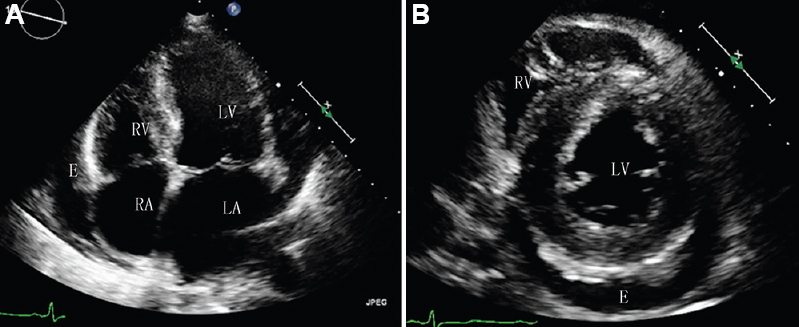
- Transthoracic echocardiogram two-dimensional still images. Both views showed the thickened diffuse hyper-refractile granular sparkling myocardium and pericardial effusion (E). (A) The apical four-chamber view; (B) the short-axis view at the papillary muscle level. LV, left ventricle; RV, right ventricle; LA, left atrium; RA, right atrium; E, pericardial effusion.

- Cardiac magnetic resonance imaging. (A) Early gadolinium phase showing asymmetric hypertrophy of the interventricular septum compared with the ventricular free wall. (B and C) Short-axis view showing global subendocardial late gadolinium enhancement (arrows) typically seen in light chain amyloidosis.
Conflicts of Interest: None.




