Translate this page into:
Effect of exercise training on functional capacity & quality of life in head & neck cancer patients receiving chemoradiotherapy
Reprint requests: Dr G. Arun Maiya, Associate Dean, Professor & Head, Department of Physiotherapy, Manipal College of Allied Health Sciences, Manipal University, Manipal 576 104, India e-mail: ajmaiya@yahoo.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Patients with head and neck cancer (HNC) undergoing chemoradiotherapy (CRT) suffer from fatigue causing a decrease in functional capacity and quality of life (QoL). Limited research in the field of exercise training among these patients demanded the need for this study to assess the effects of exercise training on functional capacity and quality of life.
Methods:
A randomized controlled trial was conducted on 48 patients with HNC undergoing CRT. The exercise group received an individually tailored, supervised, exercise programme for six weeks, while the control group did not receive any form of exercise. Functional capacity and QoL were assessed at baseline and at the end of the intervention using the six minute walk distance (6MWD) and medical outcomes survey short form 36 (SF 36).
Results:
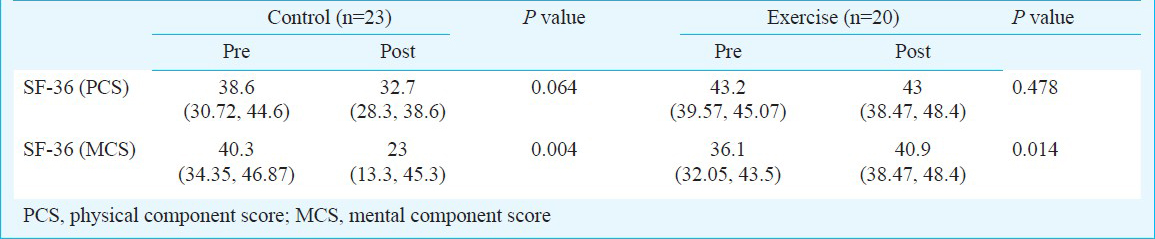
The mean age of patients was 52 yr with 42 males. After six weeks, the 6MWD improved by 42 metres (P<0.05) in the exercise group while the control group showed a decrease by 96 metres (P<0.001). There was an improvement on the mental component score (MCS) of SF36 for the exercise group (4.8; P<0.05) and the physical component score (PCS) remained almost the same, while a decrease in PCS and MCS was seen in the control group (-5.9; P=0.064 and -17.3; P<0.05). When 6MWD and SF36 were compared between the groups, there was a statistically significant difference (P<0.001) seen after six weeks.
Interpretation & conclusions:
Our results showed that the functional capacity and QoL decreased among those not receiving a supervised exercise program, while exercise training improved functional capacity and QoL in HNC patients undergoing CRT.
Keywords
Cancer
exercise
functional capacity
quality of life
rehabilitation
six minute walk test

Head and neck cancer (HNC) is common in regions of the world where the use of tobacco and alcohol is rampant. In India, HNC accounts for about one third of all cancers1. Concurrent chemoradiotherapy (CRT) in HNC patients affects speech, swallowing and respiratory functions. Patients usually depend on soft or liquid diet and in majority of the cases require a gastrostomy tube for feeding due to oral mucositis2. Fatigue and depression lead to physical inactivity in HNC patients. All these factors together, impair their functional capacity and quality of life (QoL)3.
Exercise has been associated with positive effects on the cardiovascular system, the lean body mass and on the risk for metabolic disorders. Among breast cancer patients undergoing CRT, exercise has been seen to improve functional capacity and QoL4. Recent epidemiological studies report that regular physical activity (3-5 h of moderate-intensity walking per week) is associated with a 30-50 per cent reduction in the risk of cancer-specific mortality and all-cause mortality in colorectal patients compared with patients who were physically inactive5.
Most of the studies on exercise training have been done on patients suffering from breast cancer6. There is limited information available on the effects of exercise training in HNC patients. Only one study has reported the effect of an exercise programme in HNC patients.7 This pilot, randomized controlled trial of a progressive resistance training programme focused only on shoulder dysfunction in HNC patients post neck dissection surgery. There was neither aerobic exercise component included in this study nor was the functional capacity evaluated7. In view of the morbidities faced by these patients and the paucity of literature, there is a need to assess the effects of a supervised exercise training programme for these patients undergoing CRT on their functional capacity and QoL. Therefore, the aim of the present study was to assess the effects of a supervised exercise training programme on functional capacity and QoL in patients with HNC undergoing CRT. The study began assuming the null hypothesis to be true, i.e., supervised exercise training programme will not improve the functional capacity and quality of life in patients with HNC undergoing CRT.
Material & Methods
This study was conducted with 48 patients with HNC undergoing CRT at Shirdi Sai Baba Cancer Hospital and Research Institute, Manipal, Karnataka, from January 2010 to February 2011. Ethical clearance was obtained from institutional ethics committee and written informed consent was taken prior to the enrollment of subjects into this randomized controlled trial. Patients included into the study were those above 18 yr of age, receiving treatment CRT for HNC with an Eastern Cooperative Oncology Group (ECOG) Score8 <2. Patients with platelet count <80,000/μl of blood, haemoglobin count<8g/dl, severe orthopaedic and neurological problems and patients having any contraindication to the exercise training were excluded from the trial.
The sample size was calculated based on a pre- post within group change of 50 meters on the 6MWT using an effect size of 0.45. The power of the study was kept at 80 per cent with a confidence interval of 95%. Estimating a 20 per cent drop out rate, 24 subjects in each arm was required for this study.
A description of the study participants has been shown as per the CONSORT guidelines9 (Fig.). Once patients met the inclusion criteria and written informed consent was obtained, they were randomized into two groups, i.e., exercise training and control groups, using the lottery method. The allocation was not concealed from the enrolling investigator. Block randomization in blocks of 12 was used to ensure equal numbers of subjects in both the groups at the end of each block.
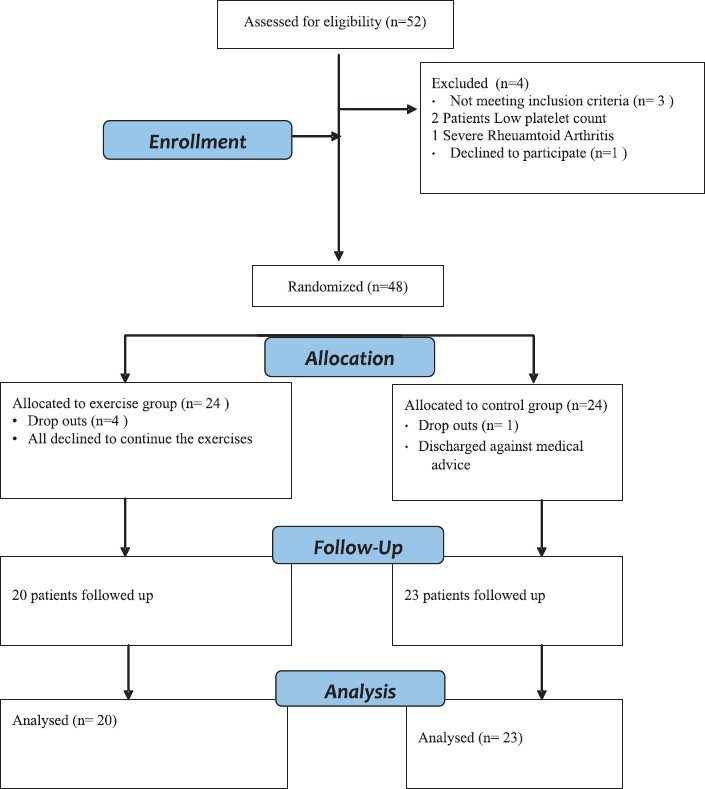
- CONSORT flow chart for the study participants.
The exercise training group received an individualized and structured exercise training programme during CRT while the control group received standard hospital care (i.e., medical and nursing care as required). The exercise training group, apart from the standard hospital care, received a programme based on the protocol by Mustain el a110 and the guidelines by American College of Sports Medicine11 which consisted of a brisk walking programme and an active exercise programme. The intensity of both these components was guided by the modified rating of perceived exertion (RPE). The first component consisted of an individually tailored brisk walking programme for 15 to 20 min at an RPE between 3-5/10 for five days a week for six weeks. The second component was an individually tailored active exercise programme (3-5/10 RPE) for the major muscle groups of upper limb and lower limb, five days a week for the six weeks. Progression was made from active to active resisted exercises for the biceps, triceps, hamstrings and quadriceps. Patients performed the exercises 8-10 times for 2-3 sets depending on their RPE levels. These exercises were performed in sitting with the back supported and the proximal part of the limb being exercised properly stabilized. Periodic assessments of the exercise programme to ensure quality control was done. The adherence rate was not monitored and calculated as this was not a part of the study objective. The family members of the patients were asked to keep the patients motivated regarding the benefits of exercise training. The control group, on the other hand, did not receive any of these exercises. They were advised to remain as physically active as possible during the study period. Following the study period, they were given a home exercise programme.
Patients in both these groups received 66 grays of radiation in 33 fractions over 6 wk. Chemotherapy consisted of 100 mg/m2 body surface area (BSA) of cisplatin on day 1, 22 and day 43. Both the groups were evaluated at baseline (before the commencement of CRT) and after six weeks for the outcome measures by the same investigator trained in assessing and evaluating these patients. The 6MWT (six minute walk test) was done as per the recommended guidelines to assess the functional capacity11. Quality of life was assessed using the medical outcomes survey short form (SF36), which is a standardized generic questionnaire13.
Statistical analysis: The data were analyzed using SPSS.17 (Chicago, IL, USA). Normality was checked using Kolmogrov-Smirnov test. Data were represented as mean and standard deviations for normally distributed data and median and interquartile ranges for non-normal data. Within group analysis was done using Wilcoxon signed ranks test and between group analysis was done using Mann-Whitney test.
Results
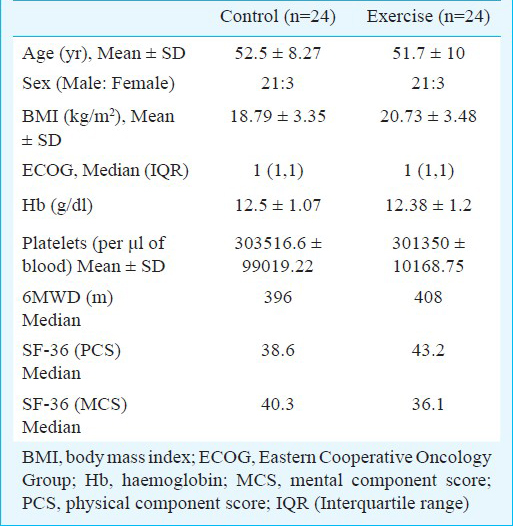
There were no adverse events or protocol deviations during the course of the study and all participants assessed provided complete data. Of the 48 patients studied, 42 were men. None of the patients were post-operative. Both the groups were comparable at baseline with regard to age, BMI and ECOG scores and did not differ with respect to the other outcomes (Table I).
The risk factors leading to HNC identified in this study were tobacco chewing (32/48; 66.6%) > smoking (27/48; 56.2%) > alcohol consumption (20/48; 41.6%).
The 6MWD improved in the exercise group (42 m) while the control group showed a decrease of 96 m (P<0.05). There was a statistically significant (P<0.001) difference in 6MWD from baseline within the groups (Table II) and also between the groups [median (IRR) for controls -100.8 (-189, 53) and for exercise group 20 (0, 46.5)] with a moderate effect size (d=0.46) for the between group comparison. Quality of life also improved with exercise training. The physical component score (PCS) decreased to 32.7 (18%) at the end of six weeks in the control group while it remained almost the same in the exercise group. The mental component score (MCS) increased to 40.9 from 36.1 (11.73% change) following the exercise training programme, while in the control group there was a 75.21 per cent decrease (Table III).

Discussion
This study evaluated the efficacy of a 6 wk exercise training programme in HNC patients undergoing CRT. Several trials have evaluated the effect of exercise training in patients suffering from cancer of the breast, colon and prostrate6. This study provides preliminary evidence that a walking and active exercise programme is safe and well tolerated by HNC patients undergoing CRT.
Functional capacity was seen to be low in both the groups prior to enrollment into the study. However, improvements in functional capacity seen with this exercise programme suggest that the harmful side effects of the CRT can be counteracted with a structured exercise programme. Our results are in line with the study done by Coleman et al14, with a similar five week exercise programme in multiple myeloma patients during chemotherapy, and Mustain et al10, who gave a four week exercise programme to breast cancer patients receiving radiotherapy. Both found a significant decrease in 6MWD in the control group. The greater magnitude of decrease in 6MWD in our study compared to these studies can be attributed to a longer treatment regime (6 wk) and that our subjects received CRT.
The patients in the exercise training group responded well to the exercise programme used in this study. A median increase of 42 meters in the exercise group highlights the positive effects of exercise training in maintaining and improving functional capacity during CRT in HNC patients. Even though this difference is lesser than the minimal clinically important difference (MCID) of 50 meters for the 6MWT12, there was still a statistical significance seen with this 42 m change. Future research needs to be done to ascertain if the MCID noted in other chronic disease populations can be generalized to cancer rehabilitation as well.
There was a significant difference in the 6MWD at the end of the CRT between the groups. This difference showed the loss in functional capacity in HNC patients who had not undergone a structured exercise programme during CRT. Along with changes in functional capacity, QoL also showed a change following the intervention with improvements in only the MCS and not in the PCS which creates a paradox. It could be hypothesized that the improvements in functional capacity probably did not translate to improvements in physical function. Perhaps the PCS did not improve because the change in the 6MWD was large enough to be statistically improved but not large enough to cross the MCID of 50 meters for the 6MWT12. However, with regard to the MCS component, the scores improved significantly suggesting a better psychological frame of mind with exercise training. This is contrary to earlier findings showing an increase in the PCS15. However, these findings were based on a small sample size (n=12) and did not include HNC patients who suffer from pain due to radiotherapy induced oral mucositis; and pain is an essential component of SF-36. The changes in only the MCS scores in the exercise training group suggest that patients with HNC undergoing CRT probably show more improvements in psychological aspects than the physical function. Perhaps a longer duration of intervention (i.e., >6 wk) may be required for demonstrable improvements in the physical function.
Four patients dropped out in the experimental group. An intention to treat analysis was not done since there were only 4 dropouts. The dropout rate was taken into consideration during the a priori sample size calculation and therefore, continues to remain sufficiently powered. These patients refused to continue the exercise programme citing disinterest and fatigue. These patients also lacked motivation and family support which can be a major reason for dropping out. Fatigue is one of the main chemotoxic adverse effects of cancer treatment. Fatigue has been postulated to be the main reason in physical inactivity and decrease in functional capacity in cancer patients6. Since fatigue was not a primary outcome for this study, this was not assessed and, therefore, the contribution of fatigue to the exercise limitation cannot be ascertained.
Chemoradiotherapy negatively affects the oxygen transport cascade thus disrupting the oxygen transport in the body. The increase in functional capacity seen in this study can be attributed to the role of exercise in increasing the cardio-respiratory endurance. Exercise also positively influences the oxygen transport thus increasing the oxygen uptake by the tissues16. As this study involved a walking intervention and active exercises, it can be hypothesized that exercise played an important role in strengthening the peripheral muscles thus improving peripheral muscle oxygen uptake thereby improving the functional capacity of these patients. Similar findings have also been seen in patients with congestive heart failure undergoing peripheral muscle exercises17. However, assessment of the cellular properties of the muscle fibres in future trials will indeed provide more insight into this hypothesis.
The absence of blinding and lack of long term follow up post CRT are certain limitations of this study. The physical activity status of patients before CRT might have further influenced the 6MWD values. Limitation of the study group to only patients with HNC makes these findings less generalizable. However, since the benefits of exercise are similar, it can be hypothesized that all forms of cancer patients may experience similar benefits.
Future research needs to determine the optimal type and intensity of exercise in HNC patients with a larger effect size to be expected for the primary outcome. The feasibility, efficacy and adherence to a home based exercise programme following CRT needs to be determined. Research involving heterogeneous groups with stratification, to determine how various types of cancers respond to exercise will be of great significance.
In conclusion, exercise training in the form of an active walking programme and active exercises improves functional capacity and quality of life in HNC patients receiving CRT. The exercise programme does not have any adverse responses in these patients.
Acknowledgment
The authors acknowledge Shri M. Milton George for his guidance.
References
- Trends of prevalence and pathological spectrum of head and neck cancers in North India. Indian J Cancer. 2005;42:89-93.
- [Google Scholar]
- Chemoradiotherapy for locally advanced head and neck cancer. J Clin Oncol. 2007;25:4118-26.
- [Google Scholar]
- Physical activity and quality of life in head and neck cancer survivors. Support Care Cancer. 2006;14:1012-9.
- [Google Scholar]
- Physical activity and survival after breast cancer diagnosis. JAMA. 2005;293:2479-86.
- [Google Scholar]
- Physical activity and survival after colorectal cancer diagnosis. J Clin Oncol. 2006;24:3527-34.
- [Google Scholar]
- Exercise for the management of cancer-related fatigue in adults. Cochrane Database Syst Rev. 2008;16(2):CD006145.
- [Google Scholar]
- Effect of exercise on upper extremity pain and dysfunction in head and neck cancer survivors. Cancer. 2008;113:214-22.
- [Google Scholar]
- Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5:649-55.
- [Google Scholar]
- CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7:e1000251.
- [Google Scholar]
- A four week home based aerobic and resistance exercise program during radiation therapy. J Support Oncol. 2009;7:158-67.
- [Google Scholar]
- American College of Sports Medicine. In: ACSM's guidelines for exercise testing and prescription (8th ed). Baltimore: Lippincott, Williams, & Wilkins; 2010. p. :228-9.
- [Google Scholar]
- ATS Statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166:111-7.
- [Google Scholar]
- The MOS 36-item short-form health survey (SF-36). Conceptual framework and item selection. Med Care. 1992;30:473-83.
- [Google Scholar]
- Effects of exercise in combination with epoetin alfa during high-dose chemotherapy and autologous peripheral blood stem cell transplantation for multiple myeloma. Onco Nurs Forum. 2008;35:E 53-61.
- [Google Scholar]
- The effects of group exercise on fatigue and quality of life during cancer treatment. Oncol Nurs Forum. 2006;33:821-5.
- [Google Scholar]
- Exercise intolerance in cancer and the role of exercise therapy to reverse dysfunction. Lancet Oncol. 2009;10:598-605.
- [Google Scholar]




