Translate this page into:
Endpoints in advanced breast cancer: methodological aspects & clinical implications
Reprint requests: Dr Everardo D. Saad, Dendrix Research, Ltd., Rua Joaquim Floriano, 72/24 - 04534-000 - Sao Paulo, Brazil e-mail: everardo@dendrix.com.br
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Breast cancer is an increasingly important public health problem in developing countries, with disproportionately high mortality. The increasing availability of active agents against advanced breast cancer makes the development of novel treatments and their choice in clinical practice progressively more complex. Furthermore, there is often a tension between the adequacy of endpoints used in clinical trials and the clinician's aim of improving survival and quality of life, the two most important therapeutic goals in advanced breast cancer. However, overall survival (OS) is no longer a suitable indicator of treatment efficacy within clinical trials in settings for which effective subsequent-line therapy exists. Conversely, progression-free survival (PFS) currently represents the most sensitive parameter to assess the efficacy of a new drug or combination in such settings. When coupled with a favourable toxicity profile and cost, the demonstration of an improved PFS may be enough evidence for the superiority of a treatment. Despite arguments favouring the use of PFS as a primary endpoint in clinical trials, clinicians who need to make sense of the available literature may be reluctant to use PFS as an indicator of clinical benefit when deciding among different therapeutic strategies for their patients. This choice is further complicated if one fails to distinguish between the use of an efficacy parameter as an indicator of therapeutic objective for individual patients and as a clinical trial endpoint. This brief review aims at helping clinicians in their daily need to interpret the literature and make informed treatment choices for patients with advanced breast cancer.
Keywords
Breast neoplasms
disease-free survival
endpoint determination
survival
survival analysis

Introduction
Over the past few decades, breast cancer has become an increasingly important public health problem in developing countries, which currently contributes to half of the disease burden worldwide1. In poor countries, mortality from breast cancer is disproportionately high, in comparison with more developed nations1, probably as a reflection of incomplete implementation of screening strategies, later stage at presentation, and lack of adequate use of adjuvant systemic therapy2. In parallel to these epidemiological trends, improvements in systemic therapy brought on by clinical trials have considerably expanded our therapeutic arsenal against advanced breast cancer. The increasing availability of active agents makes the development of novel treatments and their choice in clinical practice progressively more complex. As a result, the role of endpoints has become more critical than ever before, both for clinical trial design and for interpretation of study results. Indeed, there is often a tension between the adequacy of endpoints used for drug development (in clinical trials) and for the choice of treatments in real patients. The clinician's aim of improving survival and quality of life, the two most important therapeutic goals in advanced breast cancer3, cannot always be achieved through the use of information derived from clinical trials, not only because such trials include patients with a different profile from those in the clinic, but also because clinical trial endpoints have limitations as indicators of therapeutic benefit. Overall survival (OS), for example, appears increasingly more elusive in clinical trials4, and clinicians who treat patients with advanced breast cancer often have to base their practical decisions on the results of clinical trials that have used other efficacy endpoints. This brief review on clinical trial endpoints aims at helping clinicians in their daily need to make treatment choices for patients with advanced breast cancer.
Hierarchy and definitions of endpoints
Primary and secondary endpoints
Clinical trials often have one primary and a few secondary endpoints, all of which are objective parameters that represent study results regarding efficacy or safety variables of interest and whose differential change after treatment allows for comparisons between groups of patients. Mostly due to statistical concerns against the practice of multiple testing, there needs to be a hierarchy of endpoints within a given clinical trial. According to this hierarchy, efficacy endpoints are ranked according to their perceived importance, reflection of treatment effect upon the natural history of the disease, historical practice within the field, and regulatory constraints. In practice, primary endpoints serve two very important functions: to allow estimation of the sample size and to ascertain whether a given trial yields positive results (Fig.). Following the usual conceptual framework that underlies statistical hypothesis-testing, studies are considered positive when the P value for the primary endpoint is below a prespecified value of interest in the main population for analysis (it should be noted that this view has been questioned with the argument that not only statistical significance, but also the magnitude of benefit, should be used for declaring a phase III trial positive). From a statistical standpoint, secondary endpoints have an exploratory nature; moreover, they should be limited in number and should work as supportive measurements regarding the primary endpoint5.
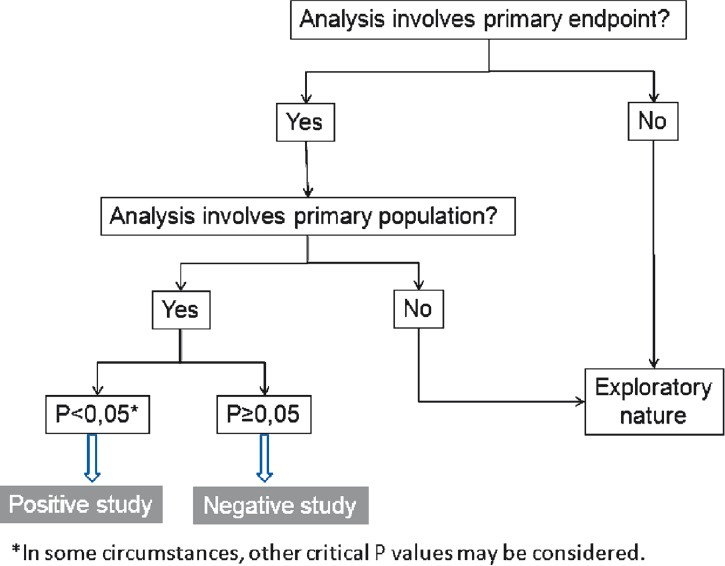
- Suggested algorithm for interpretation of a phase III clinical trial.
Time-to-event endpoints
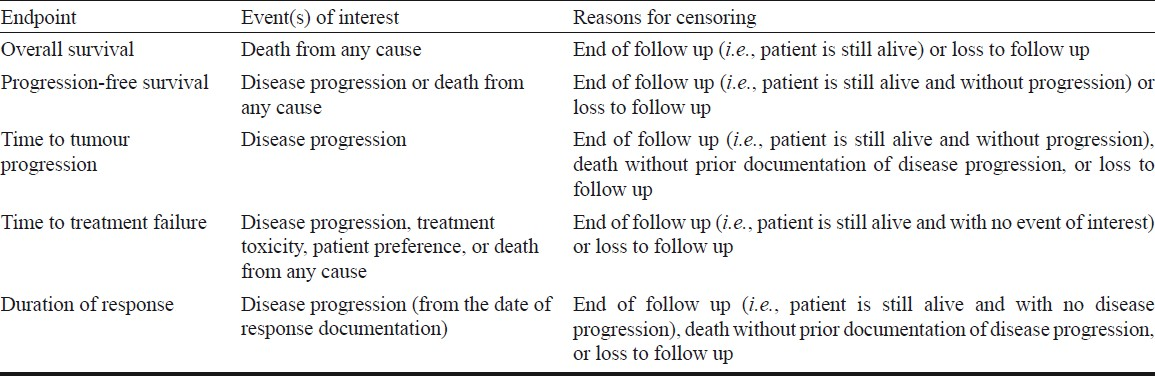
As a general rule, efficacy endpoints in oncology represent variables that may be of three types: time-to-event, categorical and continuous. Time-to-event endpoints provide information on the timing of occurrence of events of interest in oncology, such as disease progression and death. Given the importance of such events in oncology, time-to-event endpoints are usually the most important in later phases of drug development. The analysis of such events is most frequently done using the Kaplan-Meier method,6 for which one or more events of interest and one or more reasons for censoring must be defined in advance. The events of interest and reasons for censoring in the most commonly used endpoints are shown in the Table. In the case of overall survival (OS), the event of interest is death, and patients are censored when they are last seen alive or when they are lost to follow up. Over the past decade or so, OS has been used only rarely as a primary endpoint in advanced breast cancer, but has been the most frequently used secondary endpoint7. In the original definition of progression-free survival (PFS), the events of interest are tumour progression and death from any cause, with censoring of patients who are lost to follow up89. On the other hand, for time to tumour progression (TTP) the event of interest is only disease progression, with censoring of patients who die from any cause or who are lost to follow up9. In recent studies, however, many investigators have used PFS and TTP interchangeably7. As a result, either PFS or TTP have been the most frequently used endpoint in advanced breast cancer in recent studies710. Other time-to-event endpoints sometimes used in breast cancer include time to treatment failure, rarely used as primary endpoint or for regulatory purposes11, and duration of response, for which only responding patients constitute the denominator (Table).
Censoring, the key feature of Kaplan-Meier analysis, consists in excluding from the denominator of the analysis those patients who have not had one of the events of interest at the time they are last known to be at risk for having such events, provided no further information is available for those patients thenceforth. The Kaplan-Meier method is only valid if there is reason to believe that the probability of being censored is randomly distributed among patients in the study and is not related to the probability of having the events of interest (in statistical jargon, censoring must be non-informative). When this is not the case, Kaplan-Meier analysis may be biased. The number of patients censored in the analysis of a given endpoint of a particular study can often, but unfortunately not always, be known directly by numerical information provided by authors or indirectly by analyzing the tick marks on survival curves. Two or more survival curves may be compared using non parametric tests, the most common being the logrank test. Furthermore, multivariate analysis of time-to-event endpoints may be conducted using various methods, with the Cox proportional hazards model being the most frequent.
Other efficacy endpoints
The categorical endpoint most frequently used in medical oncology is the objective response rate (ORR), currently defined according to the Response Criteria in Solid Tumors guidelines1213. Although typically considered a phase II endpoint, ORR has been used as the primary endpoint in 40 per cent of recent phase III trials in advanced breast cancer10. A variant of ORR is the clinical benefit rate, often defined as the proportion of patients with no disease progression after 6 months of therapy. Categorical endpoints may be compared between groups using various tests, such as Fisher's exact test and Pearson's chi-square test, among others. Multivariate analyses of such endpoints may be undertaken with logistic regression models. In medical oncology in general, and breast cancer in particular, continuous endpoints are rarely used, with the possible exception of quality of life variables measured on numerical scales.
Advantages and disadvantages of major endpoints
Overall survival
In view of its objective measurement and the unquestionable benefit derived by patients, OS has been historically considered the most important endpoint in medical oncology14. The US Food and Drug Administration considers OS as a direct measure of treatment benefit; according to that agency, OS is usually the preferred endpoint when studies can be conducted to adequately assess survival9. However, OS is increasingly an elusive endpoint, mostly because it may be confounded by the use of treatments administered to patients after participation in a given trial, including post-progression cross-over to the experimental arm4. As a result, many randomized trials in breast cancer are underpowered to detect significant OS differences; notably, only approximately 7 per cent of recent phase III trials in advanced breast cancer have used OS as their primary endpoint10. Nevertheless, nearly 20 per cent of such trials demonstrated a significant survival improvement, most frequently in association with an accompanying gain in PFS/TTP and in trials involving patients in second- and third-line therapies10. From a strictly methodological standpoint, it is arguable that the extent to which survival gain in those trials - especially in the first line - was due to trial therapy is unknown, given the effect of post-trial interventions. As a corollary to the prior statement, the expectation of OS gain in trials for which PFS was the primary endpoint may be elusive.
PFS and TTP
Efficacy endpoints based on tumour assessments have been increasingly used in drug development, and both have been accepted as markers of clinical benefit for drug approval111516. For regulatory purposes, PFS seems preferable to TTP in so far as it captures fatal toxicities11. PFS is an attractive endpoint because it is available earlier than OS, is less likely than OS to be influenced by competing causes of death, and is not influenced by treatments administered after progression in a given trial. On the other hand, PFS is subject to measurement error and bias. Measurement error may stem from inconsistent use of definitions and standards among investigators17, whereas bias may results from unblinded ascertainment of progression and from the fact that the date at which progression is confirmed radiographically is a proxy for the true progression date, which lies somewhere within two successive assessments18. This overestimation of PFS does not raise serious methodological issues in randomized trials in which the same evaluation schedule is used for all arms, but may compromise comparisons across trials if different schedules have been used.
ORR
As stated previously, ORR is a frequent endpoint in phase III trials on advanced breast cancer. However, there are known limitations of ORR as an indicator of treatment benefit in oncology19, and patients with breast cancer and stable disease after therapy may also accrue benefit. In advanced, hormone-receptor-positive breast cancer, for example, the clinical benefit rate is often used because the survival experience of patients with stable disease after hormone therapy is commonly similar to that of patients with an objective response20. Indeed, the same has been found on occasion for patients treated with chemotherapy21. Thus, ORR is probably weaker than PFS as an efficacy parameter in advanced breast cancer, despite the fact that observing a response to treatment may be the only reliable indicator of treatment benefit in individual patients with cancer22.
Surrogate and true endpoints
Surrogate endpoints, which are used to replace so-called true endpoints of interest, should ideally be validated in a formal process that has generated considerable controversy over the past two decades23. In a research paradigm in which OS is considered the most appropriate indicator of treatment benefit, PFS, TTP and ORR should undergo formal validation before they replace OS. Such replacement is of interest in so far as it may expedite drug development. In spite of various statistically successful demonstrations of their surrogacy for OS in some tumour types and treatment settings24–26, these endpoints have not been convincingly demonstrated as surrogates for OS in advanced breast cancer27. One possible and more obvious interpretation of such findings (notwithstanding the availability of conflicting evidence in this regard)2829 is that OS remains the true endpoint of interest in advanced breast cancer, in which case these other endpoints should remain with an ancillary role in drug development. Another interpretation, however, is that OS is no longer the true endpoint of interest, as it may no longer indicate treatment benefit within a clinical trial (although it remains the most important therapeutic goal in individual patients)30. Such alternative interpretation, however, does not appear to have been accepted by the scientific community at large, and many still argue that OS remains the most appropriate primary endpoint in advanced breast cancer or in oncology in general31.
What do patients expect?
Patients with advanced cancer often face complex issues regarding their disease and treatment, and clinicians caring for these patients should assess their needs, goals, and preferences32. Although it is probably right to assume that patients with advanced breast cancer are interested in achieving the maximum possible survival and quality of life, it seems important to perform a quantitative assessment of the expectations of patients. A review of the literature suggests that cancer patients are generally willing to face the perspective of major adverse events, in exchange for small therapeutic benefits; moreover, cancer patients appear to do so more frequently than health-care professionals and well people33. In the US, a substantial percentage of women with early-stage breast cancer would accept the risk of major toxicity for minimal increase in survival time34. No similar studies among patients with advanced breast cancer appear to have been published to date.
The clinician's dilemma
Despite the above arguments favouring the use of PFS as a primary endpoint more relevant than OS in clinical trials - due mostly to the confounding effect on OS of subsequent-line therapy –, clinicians who need to make sense of the available literature may be reluctant to use PFS as an indicator of clinical benefit when deciding among different therapeutic strategies for individual patients. This choice is further complicated if one fails to distinguish between the use of an efficacy parameter as an indicator of therapeutic objective for individual patients and as a clinical trial endpoint. In individual patients, survival and quality of life are indeed the most important therapeutic objectives. However, it is questionable whether OS data derived from clinical trials are enough to inform clinicians in their quest for making patients survive longer, if one considers that gain in OS may be due to trial as well as to post-trial therapy, the latter seldom being reported, and if one considers that gain in OS is not a realistic expectation in many trials underpowered for OS gain4.
Thus, clinicians faced with the need to choose among different therapies for their patients need to consider that survival, the chief therapeutic objective in medical oncology, is no longer a suitable indicator of treatment efficacy within the realm of clinical trials in settings for which effective subsequent-line therapy exists, which is often the case in advanced breast cancer. Conversely, PFS currently represents the most sensitive parameter to assess the efficacy of a new drug or combination in settings for which such effective post-trial therapies are available. When coupled with a favourable toxicity profile and cost, the demonstration of an improved PFS may be enough evidence for the superiority of a treatment.
Conclusion
While it seems clear that extending patient survival remains the principal treatment goal in advanced breast cancer, the best way to achieve this goal appears to be the sequential use of treatments with demonstrated superiority in terms of PFS in clinical trials, as long as such treatments are affordable and display a favourable toxicity profile. Expecting to find a significant gain in OS in clinical trials on advanced breast cancer does not appear a realistic expectation in most instances. However, expecting to prolong the survival of our patients is within the reach of clinicians who master the art of clinical practice and understand enough about the science of clinical trials.
References
- Effective but cost-prohibitive drugs in breast cancer treatment: a clinician's perspective. Cancer. 2008;113:2353-8.
- [Google Scholar]
- Goals of treatment for patients with metastatic breast cancer. Semin Oncol. 2006;33:S2-5.
- [Google Scholar]
- Overall survival is not a realistic end point for clinical trials of new drugs in advanced solid tumors: a critical assessment based on recently reported phase III trials in colorectal and breast cancer. J Clin Oncol. 2003;21:2045-7.
- [Google Scholar]
- European Medicines Agency. ICH Topic E9 - Statistical Principles for Clinical Trials. Note for Guidance on Statistical Principles for Clinical Trials (CPMP/ICH/363/96) Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500002928.pdf
- [Google Scholar]
- Nonparametric estimation from incomplete observations. J Am Stat Assoc. 1958;53:457-81.
- [Google Scholar]
- Progression-free survival and time to progression as primary end points in advanced breast cancer: often used, sometimes loosely defined. Ann Oncol. 2009;20:460-4.
- [Google Scholar]
- Clinical trials in oncology. London: Chapman & Hall; 1997. p. :40.
- U.S. Department of Health and Human Services. Food and Drug Administration. Center for Drug Evaluation and Research. Center for Biologics Evaluation and Research. Guidance for Industry: Clinical Trial Endpoints for the Approval of Cancer Drugs and Biologics. Available from: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM071590.pdf
- [Google Scholar]
- Overall survival and post-progression survival in advanced breast cancer: a review of recent randomized clinical trials. J Clin Oncol. 2010;28:1958-62.
- [Google Scholar]
- End points and United States Food and Drug Administration approval of oncology drugs. J Clin Oncol. 2003;21:1404-11.
- [Google Scholar]
- New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1) Eur J Cancer. 2009;45:228-47.
- [Google Scholar]
- New guidelines to evaluate the response to treatment in solid tumors.European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst. 2000;92:205-16.
- [Google Scholar]
- General and statistical hierarchy of appropriate biologic endpoints. Oncology (Williston Park). 2006;20:5-9.
- [Google Scholar]
- Review of oncology and hematology drug product approvals at the US Food and Drug Administration between July 2005 and December 2007. J Natl Cancer Inst. 2010;102:230-43.
- [Google Scholar]
- European Medicines Agency. Appendix 1 to the Guidelines on the Evaluation of Anticancer Medicinal Products in Man (CHMP/EWP/205/95 rev. 3): Methodological Considerations for Using Progression-free Survival (PFS) as Primary Endpoint in Confirmatory Trials Registration. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/12/WC500017736.pdf
- [Google Scholar]
- Correlation between progression free survival and response rate in patients with metastatic colorectal carcinoma. Cancer. 2001;91:2033-8.
- [Google Scholar]
- When you look matters: the effect of assessment schedule on progression-free survival. J Natl Cancer Inst. 2007;99:428-32.
- [Google Scholar]
- A call for change in anticancer drug evaluation. Eur J Cancer. 1997;33(Suppl 2):S3-7.
- [Google Scholar]
- The definition of the ‘no change’ category in patients treated with endocrine therapy and chemotherapy for advanced carcinoma of the breast. Eur J Cancer Clin Oncol. 1988;24:1567-72.
- [Google Scholar]
- Multicenter phase II study of capecitabine in paclitaxel-refractory metastatic breast cancer. J Clin Oncol. 1999;17:485-93.
- [Google Scholar]
- Interpreting clinical trials in lung cancer: impact of methodology and endpoints. J Thorac Oncol. 2007;2(Suppl 2):S51-8.
- [Google Scholar]
- The validation of surrogate endpoints in meta-analyses of randomized experiments. Biostatistics. 2000;1:49-67.
- [Google Scholar]
- Progression-free survival is a surrogate for survival in advanced colorectal cancer. J Clin Oncol. 2007;25:5218-24.
- [Google Scholar]
- Surrogate endpoints for overall survival in locally advanced head and neck cancer: meta-analyses of individual patient data. Lancet Oncol. 2009;10:341-50.
- [Google Scholar]
- Leukemia-free survival as a surrogate endpoint for overall survival in the evaluation of maintenance therapy for patients with acute myeloid leukemia in complete remission. Haematologica. 2010;96:1106-12.
- [Google Scholar]
- Evaluation of tumor response, disease control, progression-free survival, and time to progression as potential surrogate end points in metastatic breast cancer. J Clin Oncol. 2008;26:1987-92.
- [Google Scholar]
- Surrogate markers and survival in women receiving first-line combination anthracycline chemotherapy for advanced breast cancer. Br J Cancer. 2005;93:1215-21.
- [Google Scholar]
- Progression-free survival as a surrogate endpoint in advanced breast cancer. Int J Technol Assess Health Care. 2008;24:371-83.
- [Google Scholar]
- Toward progression-free survival as a primary end point in advanced colorectal cancer. J Clin Oncol. 2007;25:5153-4.
- [Google Scholar]
- Issues in using progression-free survival when evaluating oncology products. J Clin Oncol. 2009;27:2874-80.
- [Google Scholar]
- American Society of Clinical Oncology Statement: Toward Individualized Care for Patients With Advanced Cancer. J Clin Oncol. 2010;29:755-60.
- [Google Scholar]
- Why do patients choose chemotherapy near the end of life? A review of the perspective of those facing death from cancer. J Clin Oncol. 2006;24:3490-6.
- [Google Scholar]
- Patient preferences for treatment of metastatic breast cancer: a study of women with early-stage breast cancer. J Clin Oncol. 1995;13:858-68.
- [Google Scholar]




