
Translate this page into:
Acute stroke management
*For correspondence: gbk5000@rediffmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 34 yr old female† suffering from rheumatic heart disease presented to Neurology Casualty of National Institute of Mental Health & Neurosciences (NIMHANS), Bengaluru, India, within two hours with sudden-onset right-sided weakness and inability to speak in August 2019. On detailed evaluation, she was found to have right hemiplegia, global aphasia and left gaze preference. Her National Institutes of Health Stroke Scales (NIHSS) score was 16. The acute stroke team was alerted, her Alberta Stroke Programme Early Computed Tomography Score was 10 and angiography revealed left M1 occlusion (Fig. 1A and B) leading to left middle cerebral artery stroke. She underwent mechanical thrombectomy with successful recanalization (Fig. 2A and B). She made almost complete recovery with modified Rankin Scale of 1 at follow up after three months.
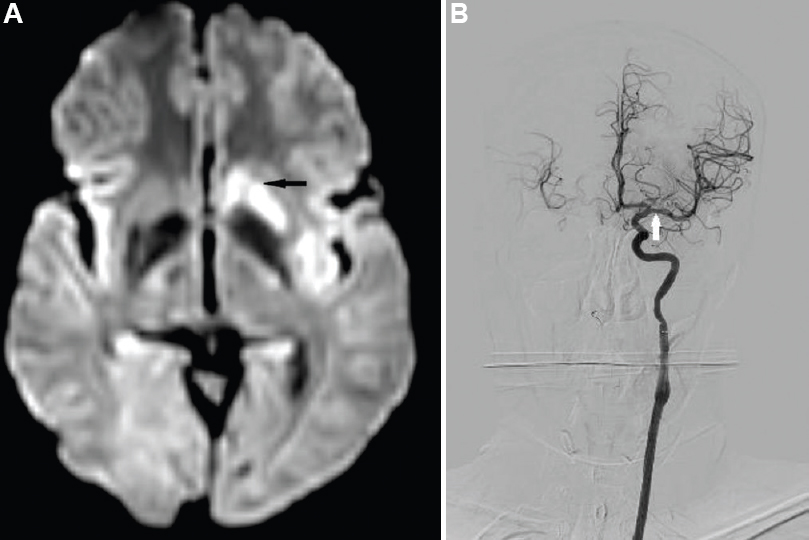
- (A) Diffusion weighted imaging done within 24 h post thrombectomy showing residual left basal ganglia restriction (black arrow). (B) Angiogram-recanalized left middle cerebral artery post-thrombectomy (white arrow).
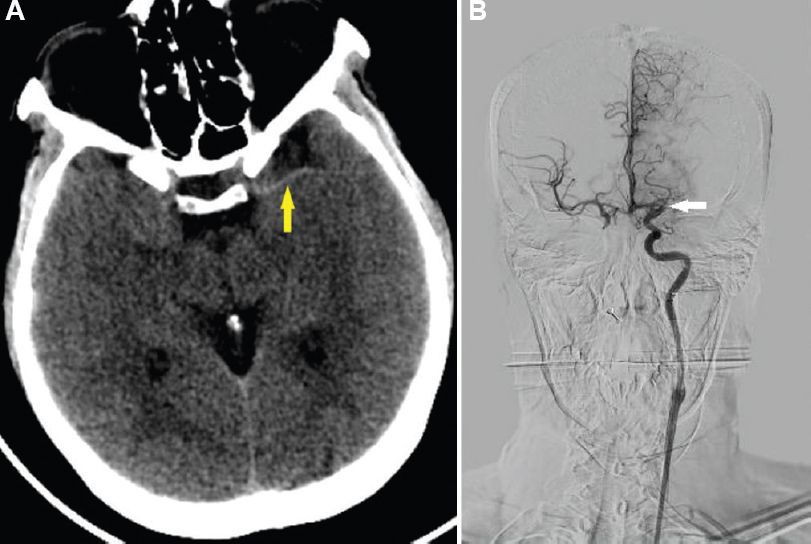
- (A) Computed tomography brain plain-hyperdense left middle cerebral artery (yellow solid arrow). (B) Angiogram-absent flow in the left middle cerebral artery (white solid arrow).
Conflicts of Interest: None.




