
Translate this page into:
A new clinical sign for posterior extrusion of talus
*For correspondence: mamc_309@yahoo.co.in
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 24 yr old male† presented to the Emergency department of Sushrut Trauma Center, New Delhi, India, in October 2019, with ankle trauma following fall from height. He had acute flexion of great toe at the interphalangeal joint. Radiographs (Fig. 1) and computed tomography (Fig. 2) revealed neck of talus fracture with posterior extrusion of talar body. The flexion of great toe persisted even after spinal anaesthesia (Fig. 3). He underwent lag screw fixation with medial malleolar osteotomy using combined anteromedial and anterolateral approaches. The fracture united after four months, but the patient remained on follow up for signs of avascular necrosis.
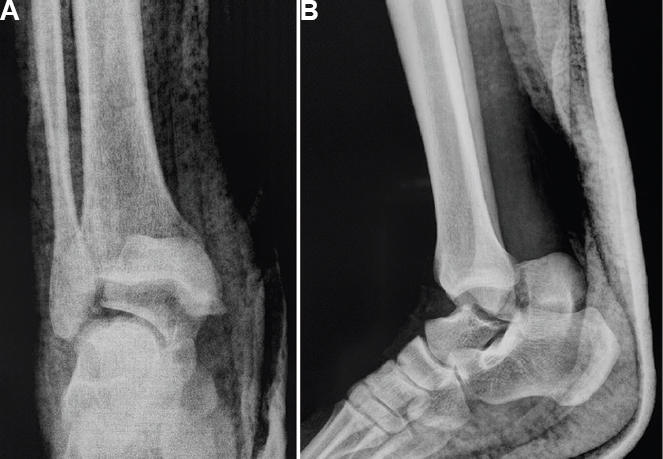
- Anteroposterior (A) and lateral (B) view radiographs of the ankle showing fracture neck of talus with posterior extrusion of talar body.
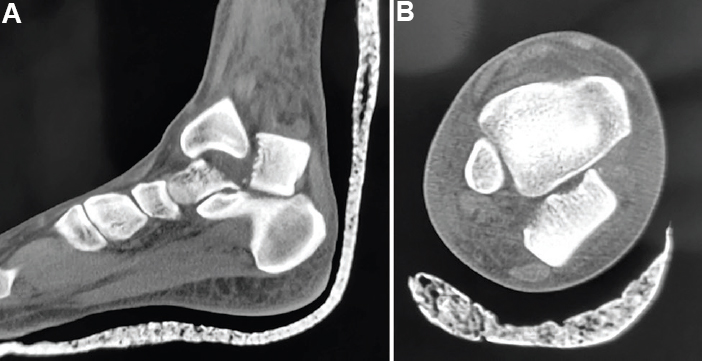
- Sagittal (A) and axial (B) views of non-contrast computed tomography showing fracture neck of talus with posterior extrusion of talar body.

- Clinical photograph after spinal anaesthesia showing persistent acute flexion of interphalangeal joint of the right great toe (arrow).
The tendon of the flexor hallucis longus (FHL), as it passes through the groove located between posteromedial and posterolateral tubercle of the talus, gets tented up with extrusion of the talus posteriorly. Other tendons on the posterior aspect of ankle get pushed aside and do not come in the way.
Conflicts of Interest: None.




