
Translate this page into:
Cardiac aspergillosis in a patient with chronic granulomatous disease
*For correspondence: manishsoneja@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 29 yr old male† with culture-proven disseminated aspergillosis having cutaneous, orbital involvement and epilepsy was diagnosed with chronic granulomatous disease based on dihydrorhodamine flow cytometry. He came to the Emergency Department of All India Institute of Medical Sciences (AIIMS), New Delhi, India, in March 2018, with acute myocardial infarction with angiography revealing complete left circumflex (LCx) and 90 per cent left anterior descending (LAD) coronary artery occlusion. Cardiac magnetic resonance imaging (cMRI) revealed an intra-myocardial mass encasing the affected coronary vessels (Fig. 1); MRI of the brain showed ring-enhancing lesions in the bilateral cerebral hemispheres (Fig. 2). He was on treatment with voriconazole for seven years; however, serum drug levels were found to be sub-therapeutic. In April 2019, he developed a recurrence of cutaneous lesions and received salvage therapy with intravenous voriconazole and caspofungin. Repeat cMRI showed minimal reduction in size. The patient declined intravenous therapy beyond three weeks and, due to paucity of alternative efficacious oral antifungal agents in disseminated aspergillosis, was continued on voriconazole and remained asymptomatic on follow up for six months.
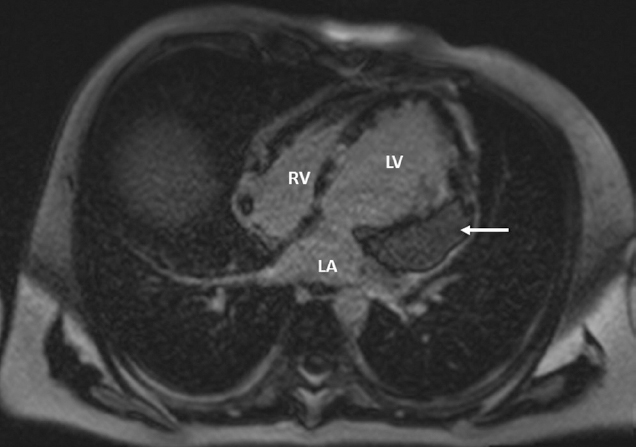
- Four-chamber axial-phase sensitive inversion recovery sequence view. Cardiac magnetic resonance imaging revealed a 7.7 × 6.2 × 6.2 cm heterogeneous intra-myocardial mass (arrow) involving trans-mural left ventricle adjacent to the stented segment of the left anterior descending (LAD) artery. Similar lesions were present in other parts of left ventricle as well as right atrium (RA) at superior vena cava–RA junction. There was no focus of fungal lesion in the lungs. The right ventricle (RV) is also shown.

- Magnetic resonance imaging brain T1 with gadolinium-contrast enhancement: Multiple well-defined peripherally enhancing lesions (arrows) with peri-lesional oedema in the bilateral fronto-parieto-temporal lobes, the largest one measuring 4 × 3.6 cm in the right parietal lobe.
Conflicts of Interest: None.




