
Translate this page into:
Malignant gastric calcification: An enigmatic entity
* For correspondence: drsuvendumaji@rediffmail.com
-
Received: ,
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 35 yr old maleϯ was referred to the department of Surgical Oncology, Institute of Post Graduate Medical Education & Research, a tertiary care teaching hospital in Kolkata, in May 2022, with the chief complaints of abdominal distension and anorexia for the last six months. Five months back, he underwent upper gastrointestinal endoscopy, which showed the presence of an ulcerative growth in the body and fundus region. Biopsy was reported as moderately differentiated adenocarcinoma. Further staging investigations ruled out distant metastasis and confirmed the presence of locally advanced gastric cancer. He underwent three cycles of neoadjuvant chemotherapy and was sent to us for a surgical opinion. On clinical examination, he had pallor, pedal oedema and ascites (Fig. 1). A contrast-enhanced computed tomography scan of the abdomen showed the presence of ascites as well as full thickness coarse mural calcification of the gastric wall (Figs 2-4). The patient was referred back to the Medical Oncology department for initiation of second line chemotherapy due to the presence of progressive disease.

- Abdominal distension due to ascites.
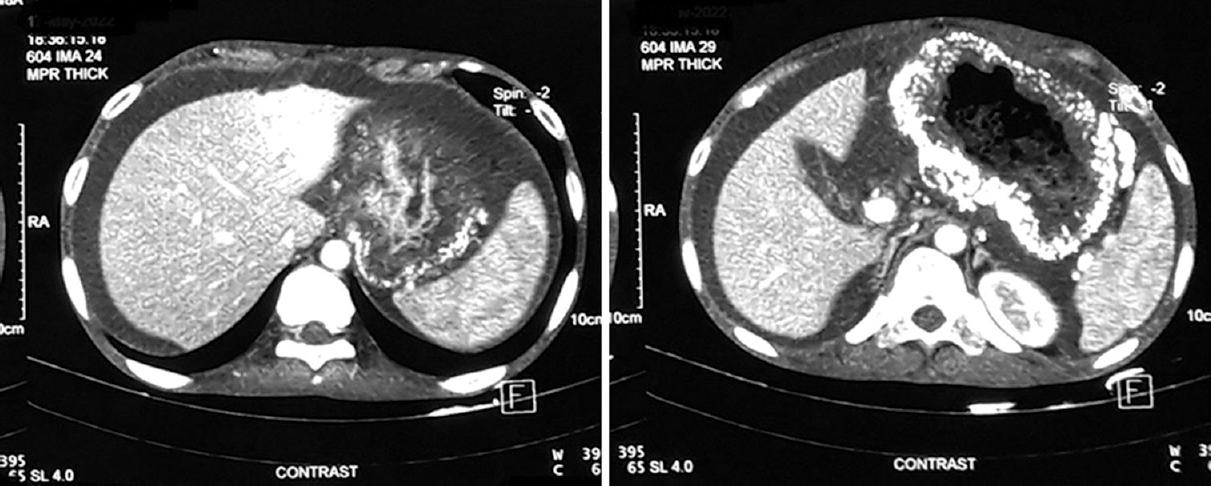
- Axial cuts of CECT scan of the abdomen showing full-thickness calcification of the gastric wall along with ascites. CECT, contrast-enhanced computed tomography.
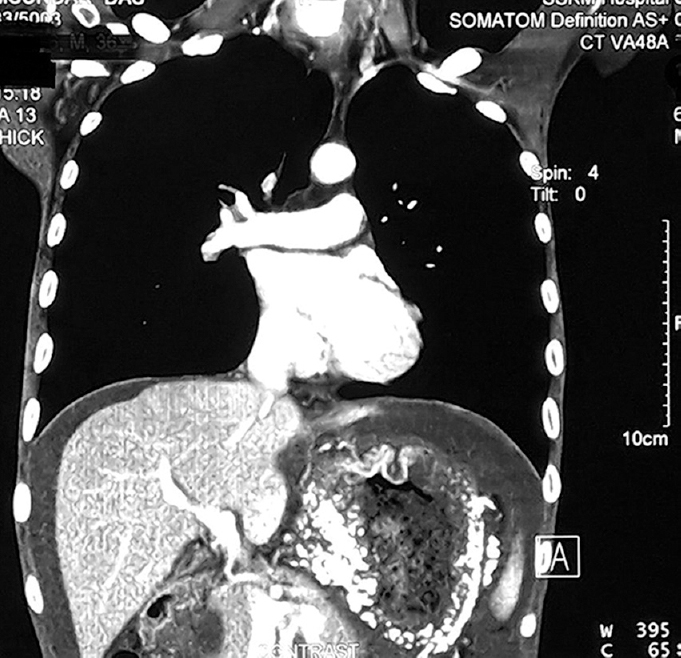
- Coronal cuts of CECT scan showing calcification of the entire stomach wall. CECT, contrast-enhanced computed tomography.

- Non-contrast CT images showing gastric wall calcification. CT, computed tomography.
Pathologic calcification can be broadly of two types: dystrophic and metastatic. While the former refers to deposits of calcium in dead necrotic tissue, the latter indicates calcium deposition in normal body tissues in the setting of deranged calcium metabolism. Calcification in malignancy is mostly dystrophic and is commonly associated with thyroid and female reproductive (breast, ovary and uterine) cancers. Gastrointestinal cancers are rarely associated with calcification, and only a few cases have been reported so far. Predominantly, such calcifications are either punctate or diffuse in nature, occur in young individuals and have been associated with mucinous adenocarcinomas. The exact mechanism and significance of gastric calcification due to underlying malignancy is not known and needs further research.
Financial support and sponsorship
None.
Conflicts of interest
None.




