
Translate this page into:
Comparison of efficacy, safety & satisfaction of intermittent versus continuous phototherapy in hyperbilirubinaemic newborns ≥35 week gestation: A randomized controlled trial
For correspondence: Dr Giridhar Sethuraman, Department of Neonatology, A- Block 1st Floor, Chettinad Hospital & Research Institute, Kelambakkam, Kanchipuram, Chennai 603 103, Tamil Nadu, India e-mail: giridharsethu@gmail.com
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Phototherapy (PT) has become the standard of care for treating neonatal jaundice. This study was aimed to find out if intermittent PT (IPT) results in comparable rate of fall of bilirubin level to continuous PT (CPT) and results in lesser side effects and better acceptance.
Methods:
In this non-inferiority trial, 174 neonates ≥35 wk gestation and >2000 g with jaundice requiring PT were randomized to receive either IPT (one hour on and two hours off) or CPT (with minimum interruptions for feeding) after device stratification [light-emitting diode (LED) or compact fluorescent light (CFL)]. Bilirubin was checked 12th hourly, and calcium, vitamin D and nitric oxide (NO) levels were analyzed along with the clinical side effects and nursing and maternal satisfaction scores (CTRI Registration No. CTRI/2018/01/011072).
Results:
The rate of fall of bilirubin was similar in both the CPT and IPT groups [0.16 (0.10, 0.22) vs. 0.13 (0.09, 0.20) mg/dl/h, P=0.22]. The median difference with 95 per cent confidence interval of 0.03 (0.03, 0.03) mg/dl was also within the pre-defined inferiority limits. There was no significant change in the duration of PT and side effects such as fall in calcium levels, rise in vitamin D and NO levels or the clinical side effects. Maternal satisfaction favoured the IPT group, but the nurses opined that IPT was difficult to implement. Subgroup analysis for PT devices used showed that efficacy of both CFL and LED devices was equivalent.
Interpretation & conclusions:
IPT was non-inferior to CPT in reducing bilirubin levels in ≥35 wk neonates, irrespective of device used, and also mothers reported better satisfaction with IPT. Although IPT appears promising, CPT does not increase clinical and biochemical side effects compared to IPT.
Keywords
Compact fluorescent light
continuous phototherapy
intermittent phototherapy
jaundice
light-emitting diode
neonate

Neonatal hyperbilirubinaemia is a common newborn condition, which, if not identified and treated early, may result in neurological complications. Phototherapy (PT) is the current standard of care for treating neonatal jaundice. To increase effectiveness, continuous PT (CPT) is recommended which involves maintaining the jaundiced neonate under PT virtually all the time with only minimal interruptions (e.g., during feeding or cleaning). However, this often results in interference with mother–infant bonding and it impedes breastfeeding12. PT exposure is also known to cause a few side effects, mainly due to the duration of PT exposure3. Notable among these are body temperature changes4, skin rash5, diarrhoea6, fall in calcium levels7, opening up of patent ductus arteriosus, especially in preterm infants, and other haemodynamic changes mainly due to increase in nitric oxide (NO) levels8910. PT may increase plasma levels of vitamin D1112.
Photodegradation of bilirubin is a two-step phenomenon, where the first step is the rapid photochemical reaction at the skin level, followed by the slow migration of unbound bilirubin from the blood into the skin for ongoing photodegradation over a period of 1-3 h1314. Interruptions in PT during this period potentially cause little alterations in bilirubin levels and also allow for migration of bilirubin to proceed effectively. Hence, intermittent PT (IPT) which involves regular cessation of PT at specific times and for specific duration appears to be a plausible alternative to CPT. Furthermore, lesser duration of PT exposure with IPT could potentially result in lesser side effects, allay parental anxiety and improve nursing experience. Hence, this study was conducted to determine if IPT results in comparable rate of fall of bilirubin as CPT, with better acceptance and lesser biochemical and clinical side effects.
Material & Methods
A non-inferiority, open-labelled, randomized controlled trial was conducted in the neonatal intensive care unit of Chettinad Hospital and Research Institute, Chennai, India, from October 2016 to September 2017. Approval from the Human Ethics Committee (50/IHEC/6-16 dated 18 July 2016) and Clinical trials Registry of India registration (CTRI/2018/01/011072) were obtained. All neonates ≥35 wk of gestation and ≥2000 g at birth, whose serum bilirubin was at a level requiring PT, as decided by the treating clinician, were included during the study period. As per the Unit policy, a PT cut-off of 2 mg/dl less than the threshold suggested by the American Academy of Paediatrics (AAP) guidelines15 was chosen to initiate PT in jaundiced neonates. PT was discontinued if bilirubin levels fell to <6 mg/dl on day 1, <10 mg/dl on day 2 and <13 mg/dl thereafter. Neonates needing immediate exchange transfusion, those with significant haemolytic jaundice, major congenital anomalies, birth asphyxia, significant haemodynamic instability and significant conjugated hyperbilirubinaemia and those who already received >5 h of PT were excluded.
Our earlier unit data (unpublished) showed that the mean rate of fall of bilirubin after CPT was 0.19±0.1 mg/dl/h. To prove, with 80 per cent power and an alpha error of 0.05, that the rate of fall of bilirubin with IPT was not different from CPT by ≥0.04 mg/dl/h, 77 neonates were needed to be enrolled in each group (STATA IC, Version 13, StatCorp, College Station, TX, USA). To account for an additional requirement of 15 per cent to conduct corresponding non-parametric test, the required sample size was 85 neonates in each group.
Of the 210 neonates assessed for eligibility, 36 were excluded for various reasons such as not giving consent (n=21), needing exchange (n=4), haemodynamically unstable (n=9) and conjugated hyperbilirubinaemia (n=2) and 174 were finally randomized. After informed written consent from the parents, the enrolled infants were stratified according to PT device type, compact fluorescent light (CFL) and light-emitting diode (LED). They were randomly allocated to receive either IPT or CPT. The random sequence was generated online (http://www.randomization.com) and serially numbered, opaque, sealed envelopes in block sizes of eight were prepared. The primary investigator allocated the groups by opening the identical envelopes containing the treatment code. Considering the nature of intervention, blinding was not attempted, but the laboratory technician who did the processing of the blood samples, was unaware of allocation.
All enrolled neonates received intensive PT (irradiance ≥30 μW/cm2/nm) using either CFL PT Unit [Nice Neotech (P) Ltd., Chennai, India] or Brilliance Pro LED [Phoenix Medical Systems (P) Ltd., Chennai]. A distance of 25-30 cm was maintained between the neonate and the device, and the irradiance was checked before PT using a Nice 4020 spectroradiometer [Nice Neotech (P) Ltd., Chennai] to ensure deliverance of ≥30 μW/cm2/nm. An additional bottom PT was added, if required.
IPT was defined as PT delivered in cycles of one hour on and two hours off. The two-hours off period was utilized for kangaroo care, feeding and cleaning the infant. CPT was defined as neonates receiving PT with ≤9 interruptions for feeding lasting ≤20 min over a 24 h period. The number of interruptions (both intended and otherwise) was noted, and all efforts were taken to ensure adherence to protocol. A lactation counsellor helped mothers with breastfeeding and coordinated the feed timings and ensured that the neonates were adequately fed during the break period. Nursing satisfaction was obtained at fortnightly intervals using a feedback form, a Likert-type scale developed in our Unit. The mothers scored their experience when PT was stopped, using a scale, developed by Olusanya et al16.
Serum bilirubin levels were measured every 12 h by the Jendrassik-Grof method17 (Coral Clinisystems, Goa, India assay sensitivity – 0.1 mg/dl). Testing was also be done for levels of NO (Griess reaction18 : SRL Pvt Ltd, Chennai; sensitivity 500 nM/l), calcium (o-cresolphthalein complexone method19 : Coral Clinisystems, Goa; sensitivity 2 mg/dl) and vitamin DELISA20 (Eagle Biosciences, Nashua, NH, USA; sensitivity 0.5 ng/ml) at enrolment and immediately after study completion. External quality assurance was done with the department of Clinical Biochemistry, Christian Medical College, Vellore. The vital signs including non-invasive blood pressure were recorded at enrolment and then hourly till completion of PT. Other documentations included skin rashes, number of times of stooling and weight recording.
The primary outcome of the study was rate of fall of bilirubin, which was defined as the difference between maximum bilirubin after enrolment and bilirubin at the end of PT divided by the duration of PT. The secondary outcomes evaluated were duration of PT (from PT initiation to final discontinuation and including interruptions in PT), maternal satisfaction score, nursing satisfaction score, clinical side effects of PT such as hypo/hyperthermia (axillary temperature <36.5/>37.5°C), rash (macular/papular/maculopapular), hypotension (<3rd centile on Zubrow's charts) and increased stooling (> 8 times/day) and biochemical parameters such as fall in calcium, NO and vitamin D. The CFL and LED subgroups were defined a priori.
Statistical analysis: Numerical outcomes such as rate of fall of bilirubin, duration of PT, calcium, NO, vitamin D and maternal and nursing satisfaction score were analyzed by non-parametric tests like Mann–Whitney U-test for independent samples considering their skewed distribution. Categorical outcomes such as hypo/hyperthermia, rash, hypotension and increased stooling were analyzed by Chi-square test or Fisher's exact test. Analysis was done using IBM SPSS Statistics for Windows, Version 21.0 (IBM Corp. NY, USA). Intention-to-treat analysis was performed.
Results
Of a total of 210 neonates who were eligible, 36 were excluded for various reasons and 174 were randomized into either CPT or IPT group. In either group, neonates were stratified to receive either CFL or LED (Figure).
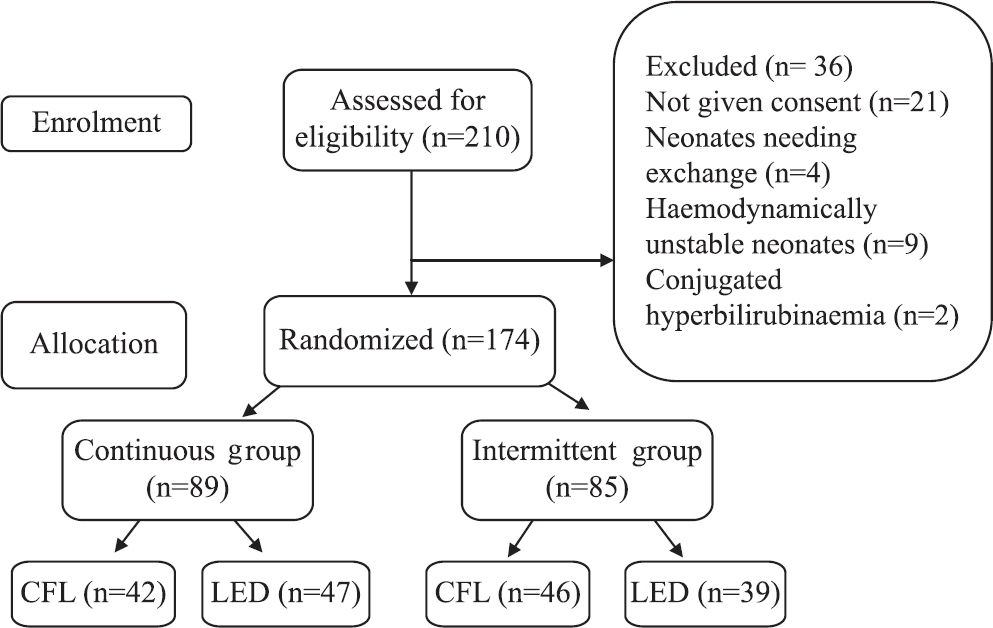
- Consort flowchart showing study design.
The baseline demographic characteristics of the two groups were similar (Table I). Analysis of the primary outcome (Table II) showed that the median rate of fall of bilirubin was higher but non-significant in the CPT group compared to the IPT group (0.16 vs. 0.13 mg/dl/h). The median difference was 0.03 mg/dl/h and the 95 per cent confidence interval (CI) of the median difference ranged from 0.03 to 0.03 mg/dl/h, which was within the pre-defined limits of non-inferiority (Δ=0.04 mg/dl/h).
| Parameter | Intervention group | |
|---|---|---|
| CPT (n=89) | IPT (n=85) | |
| Sex | ||
| Boys, n (%) | 48 (27) | 43 (25) |
| Girls, n (%) | 41 (23) | 42 (24) |
| Birth weight (kg)# | 3.01±0.47 | 2.98±0.63 |
| Gestational age (weeks)† | 38 (37, 38.5) | 38 (37, 39) |
| Age at starting PT (h)† | 70 (59, 80) | 68 (48, 79) |
| Mode of delivery | ||
| Assisted vaginal delivery, n (%) | 4 (2) | 4 (2) |
| LSCS, n (%) | 48 (27) | 47 (27) |
| NVD, n (%) | 37 (21) | 34 (19) |
| Risk factors | ||
| Incompatibility setting, n (%) | 24 (14) | 24 (14) |
| Previous baby jaundice, n (%) | 2 (1) | 6 (3) |
| IGDM, n (%) | 2 (1) | 1 (0.5) |
| Excessive weight loss, n (%) | 5 (3) | 2 (1) |
| Cephalohaematoma, n (%) | 1 (0.5) | 0 (0) |
| Type of feed | ||
| Exclusive breast feeding, n (%) | 39 (22) | 40 (23) |
| Breast feeding + formula, n (%) | 33 (19) | 29 (17) |
| Formula, n (%) | 17 (10) | 16 (9) |
| Flux delivered (μW/cm2/nm)† | 49 (44, 52.5) | 48 (44, 52) |
| Bilirubin at enrolment (mg/dl)† | 14.4 (13.4, 15.2) | 14.6 (13.6, 16.3) |
#Mean±SD, †Median (IQR). IGDM, infant of diabetic mother; NVD, normal vaginal delivery; LSCS, lower segment caesarean section; IPT, intermittent phototherapy; CPT, continuous phototherapy; SD, standard deviation; IQR, interquartile range; PT, phototherapy
| Parameter | CPT (n=89) | IPT (n=85) |
|---|---|---|
| Rate of fall of bilirubin (mg/dl/h)† | 0.16 (0.10, 0.22) | 0.13 (0.09, 0.20) |
| Duration of PT (h)† | 24 (19, 29) | 24 (18, 28) |
| Fall in calcium levels (mg/dl)# | 0.82±1.29 | 0.96±1.26 |
| Number of neonates with hypocalcaemia (<7.5 mg/dl) | 0 | 0 |
| NO level elevation (µM/l)† | 1 (−2.5, 7.5) | 2 (−2.25, 5.5) |
| Vitamin D level elevation (ng/ml)† | 0 (−2, 2) | 1 (−1.5, 2.5) |
| Side effects | ||
| Increased stooling >8 t/day, n (%) | 3 (3.4) | 2 (2.4) |
| Rash, n (%) | 4 (4.5) | 3 (3.5) |
| Nursing satisfaction score | ||
| Experience with maintaining timing† | 10 (9, 10)*** | 8 (7, 9) |
| Experience with dealing the parents† | 10 (10, 10)*** | 8 (7, 9) |
| Experience with handling the baby† | 7 (6, 9) | 8 (7, 9) |
| Opinion regarding any benefit by trying this method† | 8 (7, 9)*** | 9 (8, 10) |
| Overall experience with current therapy† | 10 (9, 10)*** | 8 (7, 9) |
| Maternal satisfaction score | ||
| Environmental comfort† | 8 (7, 9)*** | 9 (8.5, 10) |
| Care provided by nurse during phototherapy† | 8 (7, 9)*** | 10 (10, 10) |
| Opportunity to feed and bond with child† | 7 (7, 8)*** | 10 (10, 10) |
| Opportunity to socialize with other mothers† | 7 (6, 8)*** | 10 (10, 10) |
| Overall experience with current therapy† | 7 (7, 9)*** | 9 (8, 10) |
P***<0.001 compared to IPT group. †Median (IQR), #Mean±SD. IPT, intermittent phototherapy; CPT, continuous phototherapy; NO, nitric oxide; SD, standard deviation; IQR, interquartile range; PT, phototherapy
There was no significant increase in the median duration of PT between the CPT and IPT groups (24 vs. 24 h, P=0.97). Comparison of biochemical parameters between the IPT and CPT groups was done (Table III). The mean fall in calcium levels (0.82 vs. 0.96 mg/dl,), or the median rise in NO levels (1 vs. 2 μM/l), or median rise in vitamin D levels (0 vs. 1 ng/ml) in the CPT and IPT groups, respectively, was not significant (Table II). Only rash and diarrhoea were noted as clinical side effects in very few cases in either group. CPT and IPT did not show any difference in the proportion of clinical side effects.
| Device | Parameter | CPT (n=89) | IPT (n=85) |
|---|---|---|---|
| CFL | Rate of fall of bilirubin (mg/dl/h) | 0.16 (0.12, 0.21) | 0.16 (0.1, 0.22) |
| Duration of PT (h) | 24 (18.5, 27) | 24 (17.7, 27) | |
| Fall in calcium levels (mg/dl) | 1.3 (0.6, 1.9) | 1.6 (0.84, 2.1) | |
| NO level elevation (µM/l) | 0.75 (−1.5, 6.75) | 3.5 (0, 9.5) | |
| Vitamin D level elevation (ng/ml) | 1 (−2, 2) | 1 (−2, 3) | |
| LED | Rate of fall of bilirubin (mg/dl) | 0.17 (0.1, 0.24) | 0.11 (0.07, 0.15) |
| Duration of PT (h) | 24 (17, 36) | 24 (24, 36) | |
| Fall in calcium levels (mg/dl) | 0.1 (−0.8, 0.83) | 0.1 (−0.4, 1) | |
| NO level elevation (µM/l) | 1 (−5.5, 11) | 0 (−7.5, 3) | |
| Vitamin D level elevation (ng/ml) | 0 (−2, 1) | 0 (−1, 1) |
Values are shown as median (IQR). IPT, intermittent phototherapy; CPT, continuous phototherapy; CFL, compact fluorescent light; NO, nitric oxide; IQR, interquartile range; PT, phototherapy; LED, light-emitting diode
Mothers were satisfied in terms of ease of feeding, bonding with the baby and the opportunity to socialize with other mothers during the off time of IPT. However, the nursing staff reported more difficulty in timekeeping and handling of parents in the IPT group. They reported greater satisfaction with CPT compared with IPT (Table IV).
| Device | Parameter | CPT (n=89) | IPT (n=85) |
|---|---|---|---|
| CFL | Rate of fall of bilirubin (mg/dl/h) | 0.16 (0.12, 0.21) | 0.16 (0.1, 0.22) |
| Duration of PT (h) | 24 (18.5, 27) | 24 (17.7, 27) | |
| Fall in calcium levels (mg/dl) | 1.3 (0.6, 1.9) | 1.6 (0.84, 2.1) | |
| NO level elevation (µM/l) | 0.75 (−1.5, 6.75) | 3.5 (0, 9.5) | |
| Vitamin D level elevation (ng/ml) | 1 (−2, 2) | 1 (−2, 3) | |
| LED | Rate of fall of bilirubin (mg/dl) | 0.17 (0.1, 0.24) | 0.11 (0.07, 0.15) |
| Duration of PT (h) | 24 (17, 36) | 24 (24, 36) | |
| Fall in calcium levels (mg/dl) | 0.1 (−0.8, 0.83) | 0.1 (−0.4, 1) | |
| NO level elevation (µM/l) | 1 (−5.5, 11) | 0 (−7.5, 3) | |
| Vitamin D level elevation (ng/ml) | 0 (−2, 1) | 0 (−1, 1) |
Values are shown as median (IQR). IPT, intermittent phototherapy; CPT, continuous phototherapy; LED, light-emitting diode; CFL, compact fluorescent light; NO, nitric oxide; IQR, interquartile range; PT, phototherapy
Comparing outcomes stratified according to PT device used, none of the outcomes (primary and secondary) was significantly different between the CPT and IPT groups, when both CFL and LED were used for delivering PT.
Discussion
The results of our study showed that IPT was non-inferior to CPT in decreasing bilirubin levels. Even though CPT resulted in a higher rate of fall of bilirubin, the difference along with the 95 per cent CI was within the pre-defined limits of inferiority. Our study partially concurred with the results of a similar study done in India, where Sachdeva et al21 found IPT to be not only non-inferior but also more effective than CPT. They used a longer cycling period of 12 h on and then 12 h off IPT protocol to simulate a day care treatment plan. The mean irradiance delivered was higher in our trial (47 μW/cm2/nm). Although Sachdeva et al21 mentioned that a minimal irradiance of 30 μW/cm2/nm was ensured, but it was difficult to reach irradiance >30 μW/cm2/nm with single CFL devices22. It has been postulated that the higher irradiance delivered in our study, in spite of the shorter PT time, has resulted in the higher but non-significant fall in bilirubin in the CPT group.
Other studies comparing IPT and CPT showed varying results, probably because of the different IPT on–off cycles used232425262728. However, two trials using shorter IPT cycles, like our trial, showed that IPT was non-inferior to CPT2930. The higher rate of fall of bilirubin seen in the CPT group, compared to the IPT group, was primarily driven by the results from the LED strata. None of the previous IPT versus CPT trials used LED devices. Although LED devices are potentially more effective than CFL devices because of the higher luminous intensity, irradiance and narrow wavelength band, studies showed that clinical efficacy of LED was only comparable with CFL2230. Our results were in concordance with other studies using Super LED device with adjusted footprint area3132. However, the higher efficacy of LED in the CPT group compared to IPT group in CFL and LED subgroups, as suggested by our subgroup analysis, could be an inflation of type 1 error and further adequately powered trials testing this hypothesis would be required.
Comparison of biochemical outcomes in our study showed that the alteration in calcium, vitamin D and NO status was not significantly different between the CPT and IPT groups. It was presumed that the lesser duration of PT received in the IPT group could lead to lesser side effects making IPT a better choice. However, our results proved otherwise, possibly suggesting the presence of hitherto unknown factors that could contribute to these outcomes.
Our presumption was that if IPT was non-inferior to CPT, mothers and nurses might favour IPT, due to the more opportunity to feed and bond with the neonate. However, experts have opined that IPT, despite improving maternal satisfaction, could burden the nurses, especially when short on–off cycles are used33.
Limitations of our study were that blinding was not possible and duration of PT could not be precisely assessed as bilirubin was measured at 12-hourly intervals only. The baseline bilirubin levels of our study participants were in the moderately hyperbilirubinaemic range, and preterm infants were not enrolled in the study. Hence, our results cannot be extrapolated to infants with severe jaundice and preterm babies.
In conclusion, our results showed that IPT was non-inferior to CPT and could be offered for treating neonatal jaundice, irrespective of the device used. Mothers found it convenient as it provided more opportunities for feeding and fosters mother–infant bonding. CPT caused a higher but non significant rate of fall in bilirubin levels, especially when LED devices were used. Further trials comparing IPT and CPT using LED devices are required to arrive at any final conclusion.
Treatment thresholds for starting PT used in our study were lower than the standard AAP-PT thresholds. Hence, safety should be established at higher values before recommending for practice.
Acknowledgment:
Authors acknowledge the support of Ms Vimala Devi, department of Allied Health Sciences, CHRI, for helping in analysing serum samples.
Financial support & sponsorship: None.
Conflicts of Interest: None.
References
- Jaundice, terminating breast-feeding, and the vulnerable child. Pediatrics. 1989;84:773-8.
- [Google Scholar]
- Hospital routines in infants with hyperbilirubinemia influence the duration of breast feeding. Acta Paediatr Scand. 1986;75:708-12.
- [Google Scholar]
- The side effects of phototherapy for neonatal jaundice: What do we know? What should we do? Eur J Pediatr. 2011;170:1247-55.
- [Google Scholar]
- Body temperature changes of newborns under fluorescent versus LED phototherapy. Indian J Pediatr. 2014;81:751-4.
- [Google Scholar]
- Phototherapy-induced Purpuric Eruption in a Neonate. J Clin Aesthet Dermatol. 2015;8:46-8.
- [Google Scholar]
- Diarrhoea in jaundiced neonates treated with phototherapy: Role of intestinal secretion. Arch Dis Child. 1989;64:1161-4.
- [Google Scholar]
- Phototherapy-induced hypocalcemia in icteric newborns. Iran J Med Sci. 2002;27:169-71.
- [Google Scholar]
- Cardiac output changes in newborns with hyperbilirubinemia treated with phototherapy. Pediatrics. 1985;76:918-21.
- [Google Scholar]
- Effect of phototherapy on blood endothelin and nitric oxide levels: Clinical significance in preterm infants. World J Pediatr. 2008;4:31-5.
- [Google Scholar]
- Effect of phototherapy on neonatal heart rate variability and complexity. Neonatology. 2009;95:41-6.
- [Google Scholar]
- Effect of phototherapy on plasma 25(OH)-vitamin D in neonates. Biol Neonate. 1984;45:225-7.
- [Google Scholar]
- Serum vitamin D metabolites in normal subjects after phototherapy. Scand J Clin Lab Invest. 1984;44:53-6.
- [Google Scholar]
- Phototherapy for neonatal hyperbilirubinemia: Efficacy, mechanism and toxicity. Adv Pediatr. 1980;27:341-89.
- [Google Scholar]
- Early isomerization of bilirubin in phototherapy of neonatal jaundice. Pediatr Res. 2010;67:656-9.
- [Google Scholar]
- Management of hyperbilirubinemia in the newborn infant 35 or more weeks of gestation. American Academy of Pediatrics Subcommittee on Hyperbilirubinemia. Pediatrics. 2004;114:297-316.
- [Google Scholar]
- Maternal satisfaction with a novel filtered-sunlight phototherapy for newborn jaundice in Southwest Nigeria. BMC Pediatr. 2014;14:180.
- [Google Scholar]
- [Vereinfachte photometrische methoden zur bestimmung des blut bilirubins] Biochem Z. 1938;297:81-9.
- [Google Scholar]
- Nitrite and nitrate measurement by Griess reagent in human plasma: evaluation of interferences and standardization. Methods Enzymol. 2008;440:361-80.
- [Google Scholar]
- The colorimetric estimation of calcium in serum with o-cresolphthalein complexone. Clinica Chimica Acta. 1957;2:576-80.
- [Google Scholar]
- Measurement of circulating 25-hydroxy vitamin d using three commercial enzyme-linked immunosorbent assay kits with comparison to liquid chromatography: tandem mass spectrometry method. ISRN Nutr. 2013;2013:723139.
- [Google Scholar]
- Intermittent versus continuous phototherapy for the treatment of neonatal non-hemolytic moderate hyperbilirubinemia in infants more than 34 weeks of gestational age: A randomized controlled trial. Eur J Pediatr. 2015;174:177-81.
- [Google Scholar]
- Light emitting diodes versus compact fluorescent tubes for phototherapy in neonatal jaundice: A multi center randomized controlled trial. Indian Pediatr. 2010;47:131-7.
- [Google Scholar]
- Alternate phototherapy in neonatal hyperbilirubinemia. Biol Neonate. 1974;25:283-8.
- [Google Scholar]
- Clinical application of phototherapy in neonatal jaundice. Birth Defects Orig Artic Ser. 1976;12:3-10.
- [Google Scholar]
- Controlled trial comparing agar, intermittent phototherapy, and continuous phototherapy for reducing neonatal hyperbilirubinemia. J Pediatr. 1973;82:73-6.
- [Google Scholar]
- Intermediate phototherapy in the treatment of jaundice in the premature infant. J Pediatr. 1978;92:627-30.
- [Google Scholar]
- Serum bilirubin kinetics in intermittent phototherapy of physiological jaundice. Arch Dis Child. 1984;59:892-4.
- [Google Scholar]
- Intermittent versus continuous phototherapy for reducing neonatal hyperbilirubinemia. Iran J Pediatr. 2008;18:251-6.
- [Google Scholar]
- Comparison of continuous with intermittent phototherapy in the treatment of neonatal jaundice. J Postgrad Med Inst. 2016;30:173-6.
- [Google Scholar]
- Comparison of the effect of intermittent versus continuous phototherapy for reducing neonatal hyperbilirubinemia. J Urmia Univ Med Sci. 2012;23:363-7.
- [Google Scholar]
- Efficacy of new microprocessed phototherapy system with five high intensity light emitting diodes (Super LED) J Pediatr (Rio J). 2007;83:253-8.
- [Google Scholar]
- Light-emitting diodes versus compact fluorescent tubes for phototherapy in neonatal jaundice: A randomised control trial. Int J Pediatr Res. 2014;1:72-9.
- [Google Scholar]




