
Translate this page into:
A qualitative exploratory study using One Health approach for developing an intervention package for elimination of human anthrax in an endemic district of Odisha, India
For correspondence: Dr Sanghamitra Pati, ICMR-Regional Medical Research Centre, Department of Health Research, Ministry of Health & Family Welfare, Government of India, Chandrasekharpur, Bhubaneswar 751 023, Odisha, India e-mail: sanghamitra.pati@icmr.gov.in
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Anthrax is a zoonotic disease of public health concern in India. One of the key predisposing factors is linked to the behaviour of the community. This study was nested within a baseline survey to understand the risk perception, attitude, socio-cultural and behavioural practices among different communities in an anthrax endemic tribal district of Odisha, India. It was aimed to explore the systemic gaps from the officials of different departments while addressing the animal and human anthrax cases and the knowledge, attitude, and behavioural practices among the tribal communities with regards to both animal and human anthrax signs, symptoms, and transmission from animal to human.
Methods:
A qualitative exploratory study was carried out in the district of Koraput, Odisha. Insights from eight focus group discussions (FGDs) and 42 in-depth-interviews (IDIs) with the stakeholders from health, veterinary, forest, general administrative departments and community were collected and analyzed thematically.
Results:
Major themes that emerged were inter-departmental coordination, livestock vaccination, surveillance network, laboratory facilities, prevention and control strategies with regards to the animal and human anthrax cases. The study also emphasized setting up the surveillance system as per the standard guidelines, and strengthening the diagnostic facilities for timely detection of confirmed cases. It also highlighted the current needs and the gaps among inter-sectoral coordination, collaboration, and sensitization among Health, Veterinary, Forest, Education, Nutrition, and Tribal Welfare Departments at various levels to reduce the prevalence and control the outbreaks of anthrax in the district and State.
Interpretation & conclusions:
The coordination gaps, financial burden, insufficient relevant knowledge and information among the concerned stakeholders were the issues found in this study in addition to non-availability of proper diagnostic facility. The coordination among different departments adapting One Health approach may be one of the best possible ways for the elimination of anthrax cases in an endemic region.
Keywords
Anthrax
endemic regions
FDG
One Health
surveillance
zoonotic disease

Anthrax is an important zoonotic disease caused by spore-forming Bacillus anthracis, which is a Gram-positive, rod-shaped bacterium. It is primarily known as a disease of herbivores as it causes uncontrolled death in cattle, sheep, goats, horses and pigs worldwide12. Infection in humans occurs when there is a contact with carcasses or animal products infected by vegetative bacilli, inhalation of spores and consumption of undercooked infected meat3. Three types of anthrax are found in human beings which are classified according to the route of transmission including cutaneous,gastrointestinal, and inhalational forms of anthrax. Among these, cutaneous anthrax accounts for almost 95 per centof the total human anthrax cases reported. If left untreated, cutaneous anthrax may progress in up to 20per cent of cases to septicaemia with a potentially lethal outcome245.
The annual occurrence of human anthrax cases is estimated between 20,000 and 100,000 globally4. In India, anthrax is enzootic in states like Andhra Pradesh, Jammu and Kashmir, Tamil Nadu, Odisha and Karnataka1. The actual incidence of anthrax in India is not known accurately since many cases go unreported and only a fraction of human cases receives medical attention in a hospital. Many of the tribal areas have poor public health infrastructure which makes the perfect amalgamation and interface of risk factors that are conducive for zoonotic transmission of anthrax to the human population. Hence, the incidence of anthrax in human is likely to be higher than reported in the literature67.
In the last 15 years, 14 out of 30 districts in Odisha, have witnessed outbreaks of anthrax affecting at least 1208 people of which 436 had total outcome6. Koraput district tops the list with more than 300 human cases and more than 10 deaths with confirmed anthrax infection during the last sixyears8. Potential exposure to this zoonotic pathogen combined with limited medical diagnosis facilities and trained personnel in the tribal district inevitably assign substantial responsibility for disease prevention to individuals9. This study was focused on anthrax disease that was occasionally diagnosed from surveillance systems or research projects in humans living in tribal areas. One Health strategy was adopted and various intervention packages were deployed to stop the disease transmission from animals to humans. This study was nested within a baseline survey to understand the risk perception, attitude, socio-cultural and behavioural practices among different communities in an anthrax endemic tribal district of Odisha, India. The perceptions of the tribal community regarding cause, transmission, symptoms, and preventive measures both for human and animal anthrax were also studied.
Material & Methods
This study was conducted in the anthrax endemic Koraput district of Odisha, India. The district was selected purposively for demonstration of the intervention package developed by using One Health approach for elimination of human anthrax and was carried in coordination with Saheed Laxman Narayan Medical College and Department of Public Health, Koraput. The district is divided among 2028 villages, 240 Gram panchayats, and 14 blocks administratively. All the 14 blocks were covered during the study for in-depth interviews (IDIs) and focussed group discussions (FGDs) (Figure).
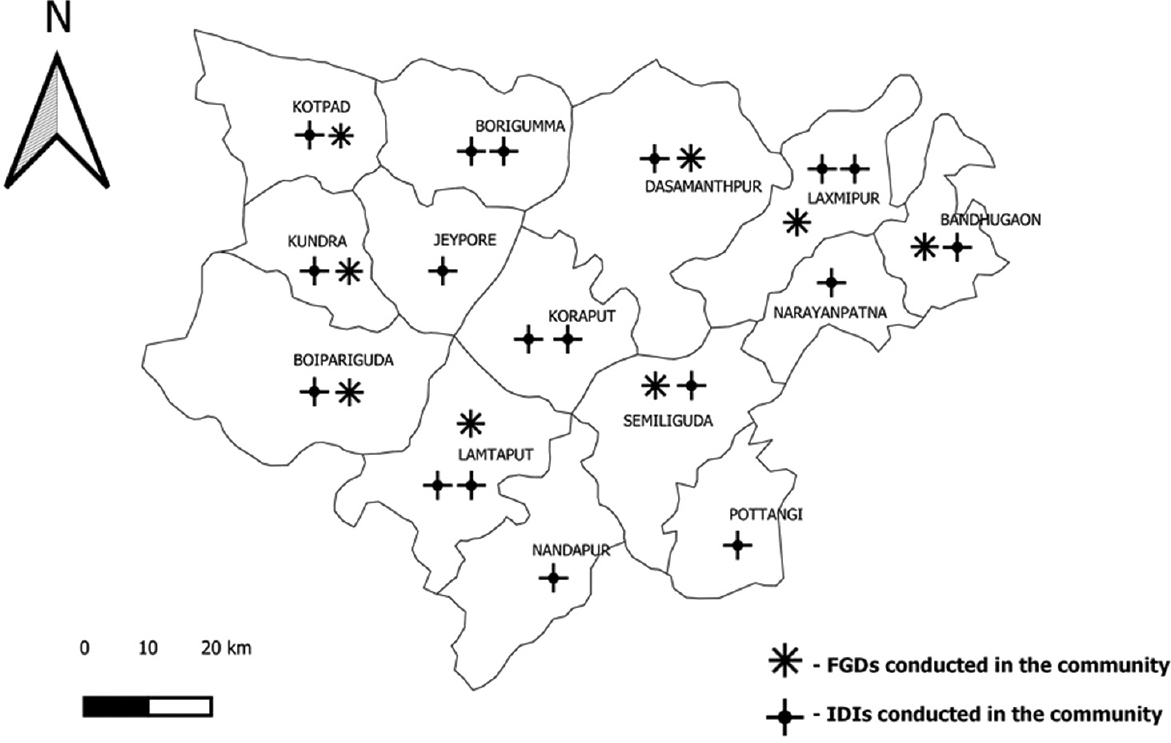
- Focussed group discussions (FGDs) and in-depth interviews (IDIs) conducted in different blocks of Koraput district, Odisha. (QGIS v3.10, GIS mapping software used to generate map).
Study design: The FGDs and IDIs were carried out with all the key stakeholders (Table I). A total of eight FGDs and 42 IDIs were conducted among the stakeholders from the Health Department, Veterinary Department, Forest Department, general administrative departments, and participants from the community. Four FGDs were conducted with the community from the four blocks of Koraput i.e. Dasmanthpur, Boipariguda, Lamtaput and Laxmipur having reported anthrax cases in the last three years and other four FGDs were carried out in the blocks of Kundra, Semiliguda, Kotpad and Bandhuga on with no anthrax cases in the recent past. The consolidated criteria for reporting qualitative research (COREQ) guidelines and triangulation methods were followed while carrying out this qualitative study.
| Study level | Health Department (n=6) | Veterinary Department (n=6) | Forest Department (n=6) | General Administration (n=6) | Community (n=26) |
|---|---|---|---|---|---|
| IDIs (n=42) | Medical Officer (n=3) | Livestock Inspector (n=2) | Forest Guard (n=2) | Education Officer (n=1) | 18 Individuals |
| District Medical Officer (n=1) | Block Veterinary Officer (n=3) | Forest Range Officer (n=3) | Block Development Officer (n=2) | ||
| Epidemiologist (n=1) | District Veterinary Officer (n=1) | Assistant Conservator of Forest (n=1) | Tribal Welfare Department (n=1) | ||
| Public Health Education Officer (n=1) | PRI (n=2) | ||||
| FGDs (n=8) | 8 Communities |
IDI, in-depth interview; FDG, focussed group discussion
Sampling and participant selection: Purposive and convenient sampling was used for the selection of participants for FGDs and IDIs. About 9-12 participants were taken for each FGD, and 24 IDIs were carried out with officials from the four departments and 18 IDIs were carried out with the key participants from the communities. The demographic characteristics of IDIs and FGD participants are provided in the (Tables I & II). All the participants were contacted before and prior meeting appointment was scheduled. For focus group discussions key persons were identified from the communities in consultation with ASHA worker and invited participants with representation of youths, elders, and women with a balanced gender ration. A designated place was chosen to carry out FGDs, all the participants were intimated before carrying out the discussions.
| Block Name | Gender | Mean age (95% CI) in years |
|---|---|---|
| Dasmanthpur (n=10) | M (n=6), F (n=4) | 37.9 (29.47-46.33) |
| Boiparigiuda (n=9) | M (n=6), F (n=3) | 32.89 (26.93-38.85) |
| Lamtaput (n=10) | M (n=5), F (n=5) | 35.1 (29.25-40.95) |
| Laxmipur (n=10) | M (n=7), F (n=3) | 39.3 (30.6-48.0) |
| Kundara (n=10) | M (n=5), F (n=5) | 39.5 (28.79-50.21) |
| Semliguda (n=11) | M (n=5), F (n=6) | 40.73 (33.52-47.93) |
| Bandhugaon (n=10) | M (n=5), F (n=5) | 43.8 (37.85-49.75) |
| Kotpad (n=12) | M (n=5), F (n=7) | 39.18 (30.52-47.83) |
| Total (n=82) | M (n=44), F (n=38) | 38.55 (30.86-46.23) |
M, male; F, female
This study was ethically approved by the Institutional Ethics Committee of ICMR - Regional Medical Research Centre, Bhubaneswar. Before the interview, the purpose of the study was explained to the interviewees and they were being informed about their right to withdraw participation from the study at any point of time. Informed written consent was obtained from each participant, prior to participation.
Data collection: FGD and IDI questionnaire guide was developed for the study. The interview guide consisted of open-ended questions and probes as per requirement. Socio-demographic questions such as age, gender, occupation, and other related questions were included. Information regarding livestock animals, food habits and vaccination of animals was enquired. The guide was developed to assess the knowledge and awareness about the anthrax disease, its sign and symptoms, attitudinal and behavioural practices and prevention among the communities and perceptions about the disease from the participants. An audio recorder was used for recording the interviews. All participants were intimated before interviews. Each interview was for a duration of 30-40 minutes. The data were subjected to content analysis. Initially, meaning units were extracted from the original transcripts and were condensed to form codes. The meaning units which were selected were linked to the aim of the study. Related codes were grouped to make the themes which demonstrated the core meanings of the texts, were identified.
Statistical analysis: All Tape-recorded IDIs and FGDs with different participants were transcribed in Odiya (local language) and later translated to English for analysis. Translated transcripts were analyzed thematically for both qualitative and quantitative research.
Results
After transcribing and translation the responses and narratives from 42 IDIs and eight FGDs, there were analyzed thematically, and major themes were as follows:
Inter-departmental coordination: Of the 24 stakeholders 20 perceived that improper coordination among the different departments led to the greater number of anthrax cases in the district and caused its transmission from animals to humans. The management of anthrax cases was possible through the coordination between different departments (Health, Veterinary, Forest, other general administrative departments) for timely action by the respective department. Five of the six stakeholders from Veterinary Department responded that reporting of animal anthrax was done at a later stage, and people in the community consumed the meat of the affected animal which ultimately resulted into the outbreak of human anthrax.
Officials from different Departments had responded that lack of communication between the grassroot level workers of Health, Veterinary, Forest, ICDS (Integrated Child Development Services), Education departments, and PRI (Panchayati Raj Institutions) workers. Health department stated that spread of anthrax disease from animal to human could have been prevented if it was identified and reported early in animals, which was possible with a proper surveillance network and involvement of community workers.
Veterinary official told that most of the ground level staffs were not even aware of the anthrax disease and due to this most case went unreported from the hard-to-reach communities. However, Forest officials stated that they did share the information about suspected wild animal anthrax cases with Veterinary Department. They also shared that it was tough to vaccinate wild animals but still they would try for maximum coverage. Veterinary Department officials also said that there wasa need of manpower for the proper surveillance and reporting of the disease. Livestock inspectors (LI) in position were having high workload since it was extremely difficult to manage 3-4 villages by one LI and due to that the vaccination coverage was not as expected.
Livestock vaccination: Vaccination was given free of cost in the village's endemic blocks in the district and in the non-endemic areas the vaccination was provided with the minimal fixed cost as per the type of livestock. However, the coverage of vaccination was not as expected in both endemic and non-endemic blocks defined by the district based on cases and outbreaks in the recent past.
There was a belief among the villagers that their animals would be sick after vaccination. The villagers were ready to support the vaccination drive in the village and many of them were aware of benefit of vaccination and wanted their livestock to get vaccinated. Apart from misconceptions and beliefs, there were potential barriers in achieving the maximum vaccination coverage. Veterinary Department also found it difficult to organize vaccination camps in remote areas. The travel distance between villages was more which also affected the vaccination coverage. Presumption about the cost of vaccination and medicine was another issue.
Laboratory facilities: Anthrax diagnostic facility for early diagnosis of animal and human samples was not available at the district level, so the samples were such and therefore they do send the samples to the State level laboratories which was a time consuming process. Laboratory facility for testing of samples from suspected animals should be strengthened at district level for early diagnosis and confirmation. Stakeholders from Health Department expressed their concern about the lack of laboratory support at the regional level in providing test reports in time.
Four officials from Health Department responded that there was a lack of guidance and training among laboratory personnel and sample collectors on safety measures; they stressed periodic diagnostic technique orientation and training including safety measures. Also, these was no designated laboratory staff for diagnosis of anthrax which was one of the reasons for delay in testing of suspected animal anthrax samples.
Surveillance network: No proper surveillance system was functional in the villages for early reporting and detection of animal anthrax cases. Eating the meat and blood of dead animals was observed as a common practice among the villagers in the district.
”As this disease has happened in our village only, we have become more aware and that is why we do not eat the meat and blood of dead animals.” (Community participant).
Five of the six veterinary officials opined that there was a lack of routine surveillance in livestock. There is no proper reporting channel for suspected animal cases. Active surveillance network was not in place even though the Koraput is an endemic district for anthrax. There was no active or routine surveillance for livestock by the Veterinary Department.
Community attitude and behavioural practices: Sixty seven of the 82 participants from the tribal communities expressed that there were no awareness activities conducted by the Veterinary or Health Departments in the villages with anthrax cases in the recent past. In addition, they were not being explained about the transmission or signs and symptoms of the disease. However, the participants from only a few communities reported that burial activities of dead animals were done in the village after informing the LI, also medicines were provided to suspected human cases, and healthcare worker followed up in the village. Respondents understood the common signs of the disease and transmission route of anthrax. Only 30 respondents were able to identify signs of cutaneous anthrax, but they were unable to respond about gastrointestinal or inhalational anthrax. The participants from the communities which had cases in the recent past (last 3 years) stated that they came to know about anthrax when it affected someone in their villages and nearby villages. Communities which did not have cases in the recent past or had cases before three years, did not have much knowledge on the diseases.
Current practices in communities: While asking about the practices of eating the meat and blood of dead animals, the participants told that the meat of the dead animal was one of the resources for them. Five of the six veterinary officials opined that the IEC (Information Education Communication) material prepared for enhancement of knowledge, awareness and to bring the changes in the current practices among the villagers was not effective as there was high illiteracy among the tribal communities. There were no behaviour change communication (BCC) strategies in place in the district to change the behavioural practices of communities.
Discussion
In the last few years, anthrax outbreaks have been reported many times in Odisha where both humans and animals have been affected by the disease10. The prevalence of anthrax is higher among the tribal districts of Odisha like Koraput where a majority of the population rely on animal products for their livelihood and food requirement110. Major challenges for controlling anthrax were poor veterinary services with lack of manpower, inadequate healthcare workforce, vaccine shortage, delayed outbreak reporting and response211. For the prevention of a zoonotic disease like anthrax, robust laboratory facilities and effective surveillance system are important and One Health concept to the healthcare workforce is the need of the hour1213. Studies have shown that proper and timely diagnosis is one of the major attributes for prevention, control and treatment of human and animal anthrax and controlling epidemics. Studies conducted in Ethiopia have highlighted the importance of early diagnosis and care for controlling disease and preventing the spread of undiagnosed cases1415. Capacity building and training for staffs for the identification of clinical cases is important especially in remote areas. Most of the laboratory facilities are situated far away from the endemic area, making it difficult to transport the samples for analysis due to limited transport facilities in those areas116. Studies in Georgia has highlighted the importance of supervision during carcasses disposal, monitoring by service providers, training sessions for surveillance system strengthening and inter-sectoral coordination as key strategies to prevent anthrax1718.
Routine vaccination policy is one of the key strategies for preventing and controlling any infectious disease like anthrax but still, it is difficult to implement vaccination policy including ring vaccination in endemic regions181920. Vaccination needs to be provided for free in endemic districts and still, it seems difficult to cover fully due to unavoidable social and cultural barriers. A study in Bangladesh showed lack of staffs as one of the reasons for poor vaccination of livestock21. One Health strategy focusses on collaborative and multisectoral approach for understanding the animal-environment-human inter-relationships and plays important role in outbreak response and helps in disease-related activities222324.
Though this study was conducted in the Koraput district of Odisha but the outcomes from the study could be helpful in addressing the anthrax and other zoonotic diseases in India. These findings would be useful to develop the strategies and interventions for eliminations of human anthrax cases in endemic regions. The findings from this study suggests that the intervention may be implemented with joint efforts of the Health, Veterinary, Forest, Education, Panchayati Raj Institution, and other administrative departments for effective implementation to combat the disease at district level. The One Health strategy may be adapted as one of the best possible ways for elimination of human anthrax cases from endemic regions in India and other countries. Important areas for addressing such disease include IEC (Information Education Communication)/BCC (Behaviour Change Communication) activities in the community for building awareness among the tribal communities with regards to the diseases, signs, symptoms and transmission modes. Capacity building and sensitization of stakeholders, advocacy for regular livestock vaccination and maximizing the coverage of vaccination, inter-departmental co-ordination may be established for identification, early reporting and management of suspected cases. Establishment or strengthening of laboratory and surveillance networks is also important for timely diagnosis and tracking the suspected cases.
Acknowledgment:
Authors acknowledge all study participants for sharing the information and time, and also the efforts of field staff including Biren Kumar Padhy, Padma Mohan Pradhan, Subrat Kumar Sahoo who had worked tirelessly to complete all the IDIs and FGDs with the support district and block level officials.
Financial support & sponsorship: The financial grant for this study was provided by the Indian Council of Medical Research, New Delhi (vide letter no: ZON/33/1/2018-ECD-II).
Conflicts of Interest: The authors declare that they have no competing interests.
References
- A cutaneous anthrax outbreak in Koraput district of Odisha-India 2015. BMC Public Health. 2019;19:470.
- [Google Scholar]
- Anthrax in humans and animals (4th ed). Geneva: WHO; 2008.
- Essentials of veterinary bacteriology and mycology (6th ed). Iowa: Iowa State Press; 2004.
- Anthrax: public health risk in India and socio-environmental determinants. Indian J Community Med. 2010;35:189-90.
- [Google Scholar]
- An outbreak of cutaneous anthrax in a tribal area of Visakhapatnam district, Andhra Pradesh. J NTR Univ Health Sci. 2018;7:49.
- [Google Scholar]
- How can anthrax outbreaks be prevented in Odisha?. Available from: https://icmr.nic.in/content/policy-brief
- Lay perceptions, beliefs and practices linked to the persistence of anthrax outbreaks in cattle in the Western Province of Zambia. Onderstepoort J Vet Res. 2018;85:e1-e8.
- [Google Scholar]
- The landscape of anthrax prevention and control: stakeholders’ perceptive in Odisha, India. Int J Environ Res Public Health. 2020;17:3094.
- [Google Scholar]
- Outbreak of cutaneous anthrax in Musalimadugu village, Chittoor district, Andhra Pradesh, India, July-August 2011. J Infect Dev Ctries. 2012;6:695-9.
- [Google Scholar]
- Factors associated with repeated outbreak of anthrax in Bangladesh: Qualitative and quantitative study. J Adv Vet Anim Res. 2015;2:158-64.
- [Google Scholar]
- Health care providers’ knowledge and practice gap towards joint zoonotic disease surveillance system: challenges and opportunities, Gomma District, Southwest Ethiopia. Bio Med Res Int. 2016;2016:3942672.
- [Google Scholar]
- Diagnosis of cutaneous anthrax in resource-poor settings in west Arsi Province, Ethiopia. Ann Agric Environ Med. 2017;24:712-15.
- [Google Scholar]
- Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nurs Health Sci. 2013;15:398-405.
- [Google Scholar]
- Risk factors associated with the occurrence of anthrax outbreaks in livestock in the country of Georgia: A case-control investigation 2013-2015. PLoS One. 2019;14:e0215228.
- [Google Scholar]
- Rates and risk factors for human cutaneous anthrax in the country of Georgia: National surveillance data, 2008-2015. PLoS One. 2018;13:e0192031.
- [Google Scholar]
- Anthrax outbreaks in the humans - livestock and wildlife interface areas of Northern Tanzania: a retrospective record review 2006-2016. BMC Public Health. 2018;18:106.
- [Google Scholar]
- Knowledge, attitudes, and practices related to anthrax and animal care: A case-control study in Georgia. PLoS One. 2019;14:e0224176.
- [Google Scholar]
- Enhancing surveillance and diagnostics in anthrax-endemic countries. Emerg Infect Dis. 2017;23:S147-53.
- [Google Scholar]
- Livestock vaccine adoption among poor farmers in Bolivia: remembering innovation diffusion theory. Vaccine. 2008;26:2433-42.
- [Google Scholar]
- Use of anthrax vaccine in the United States: recommendations of the advisory committee on immunization practices, 2019. MMWR Recomm Rep. 2019;68:1-14.
- [Google Scholar]
- Centers for Disease Control and Prevention. Framework for Enhancing Anthrax Prevention & Control. Atlanta, USA: CDC; 2016.




