
Translate this page into:
Indian Council of Medical Research consensus document on hepatocellular carcinoma
For correspondence: Dr Bhawna Sirohi, Department of Medical Oncology, Apollo Proton Cancer Centre, Chennai 600 028, Tamil Nadu, India e-mail: bhawna.sirohi13@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
This document aims to assist oncologists in making clinical decisions encountered while managing their patients with hepatocellular carcinoma (HCC), specific to Indian practice, based on consensus among experts. Most patients are staged by Barcelona Clinic Liver Cancer (BCLC) staging system which comprises patient performance status, Child-Pugh status, number and size of nodules, portal vein invasion and metastasis. Patients should receive multidisciplinary care. Surgical resection and transplant forms the mainstay of curative treatment. Ablative techniques are used for small tumours (<3 cm) in patients who are not candidates for surgical resection (Child B and C). Patients with advanced (HCC should be assessed on an individual basis to determine whether targeted therapy, interventional radiology procedures or best supportive care should be provided. In advanced HCC, immunotherapy, newer targeted therapies and modern radiation therapy have shown promising results. Patients should be offered regular surveillance after completion of curative resection or treatment of advanced disease.
Keywords
Guidelines
hepatocellular carcinoma
Indian Council of Medical Research
management

There are several international guidelines pertaining to hepatocellular carcinoma (HCC)12, but none have been issued by the Indian Council of Medical Research specific for the Indian setting. The Indian population requires a unique understanding of the incidence and biology of the disease, with a different socio-economic spectrum and accessibility to healthcare resources. These guidelines are aimed to maximize healthcare resources, standardize diagnosis methodology and strengthen the multidisciplinary approach regarding the treatment of HCC in India.
Incidence and risk factors
Globally, HCC is the fifth most common cancer (0.90 million new cases per year) and is the third leading cause of annual deaths due to cancer (0.83 million deaths per year)13. There is a lack of nationally representative data, so we must depend on autopsy studies, national cancer registries and population-based surveillance data to estimate the frequency of HCC in India. A large-scale verbal autopsy study in 2010 reported liver cancer to be the fourth leading cause of cancer-related deaths in men (14,000 deaths), with an age-standardized mortality rate (ASMR) of 6.8/100,000 population. In women, liver cancer was the eighth most common cause of cancer-related deaths (12,000 deaths), with an ASMR of 5.1/100,000 population4. The areas covered by Naharlagun population-based cancer registry (PBCR) reported the highest age-adjusted incidence rate (AAIR) of 38.0 in Papum Pare district in Arunachal Pradesh5.
Risk factors corroborated in Indian studies are cirrhosis, hepatitis B infection, hepatitis C infection, alcohol consumption, aflatoxin exposure, smoking, diabetes, non-alcoholic fatty liver disease and age67. Among cancers as a whole, HCC is particularly amenable to prevention given a detailed understanding of risk factors. The most feasible and cost-effective strategy in the Indian scenario appears to be primary prevention. The most easily applicable modality is the hepatitis B vaccination, which is recommended in newborns and healthcare workers8. For patients with a high viral load in HBV cirrhosis, antiviral therapy assists in preventing HCC development and is, therefore, recommended9. Patients at risk of developing HCC are candidates for regular surveillance if they are eligible for HCC treatment. The recommended surveillance test is a six-monthly ultrasound abdomen by an experienced radiologist10.
Diagnosis and staging
Non-invasive diagnosis can be established by demonstration of the typical HCC radiological hallmark (hyperenhancement on arterial phase and wash out on porto-venous phase) by one of the imaging techniques in nodules >2 cm and by two coincidental techniques with nodules of 1-2 cm in diameter [dynamic computed tomography (CT) or dynamic magnetic resonance imaging (MRI)]. If a suspicious nodule measuring >1 cm fails to show typical enhancement pattern on both dynamic CT and dynamic MRI, image-guided sampling is indicated. The 2017 version of the Liver Imaging Reporting and Data System (LI-RADS) is a useful comprehensive system which incorporates features such as arterial-phase hyperenhancement, observation size, wash out, enhancing capsule and threshold growth11. The CT/MRI LI-RADS requires a CT/MRI with extracellular agents or MRI with hepatobiliary agents.
Immunohistochemical markers useful for diagnosing HCC include glypican-3, glutamine synthase, arginase 1, HepPar1, alpha foetoprotein (AFP) and heat shock protein-7012.
Small nodules (<1 cm) in cirrhotic livers should be subjected to a 3-6-monthly follow up using the same technique, which detected the nodule, for a period of two years. Evaluation by gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid (Gd-EOB-DTPA) - enhanced MRI scan, or a SonoVue contrast-enhanced ultrasound, is an alternative strategy. Gadobenate dimeglumine MRI is also available in India and is particularly useful for lesions not displaying the characteristic radiological features of HCC as well for detecting high-grade dysplastic nodules13. A PET (positron emission tomography) scan is not routinely recommended14. AFP estimation is no longer part of the diagnostic algorithm of HCC15.
In India, the BCLC (Barcelona Clinic Liver Cancer) staging system is commonly used and includes patient performance, Child-Pugh status, number and size of nodules, portal vein invasion and metastasis, and is most commonly used for prognostic information and treatment allocation16. Stage 0 is very early, stage A is early, stage B intermediate, stage C advanced and stage D is terminal stage HCC.
Multidisciplinary treatment for early disease
All new cases should be discussed at the tumour board or in multidisciplinary team meetings, and the treatment strategy should be confirmed. Surgery (resection/transplant) forms the mainstay of definitive treatment. Surgical resection is advocated only in early-stage disease in patients with preserved liver function (Child-Pugh A) without evidence of portal hypertension or vascular invasion. Resection can be anatomical versus non-anatomical and open versus laparoscopic. In patients with decompensated liver disease or portal hypertension, liver transplant (from a living donor or cadaveric) is the treatment of choice as it not only treats the tumour but also the underlying predisposing liver pathology1718.
Small tumours (<3 cm) in patients who are not candidates for surgical resection (Child B) can be offered ablative techniques. The percutaneous ablative therapies have role in the very early (BCLC-0) and early stage (BCLC-A), while the transarterial therapies are (generally) indicated in the intermediate stage (BCLC-B, C) of HCC. Radiofrequency ablation (RFA) is indicated when the lesion in not suitable for resection, the size of the lesion is up to 3 cm and number of lesions are three or less19. The BCLC guidelines also support the use of image-guided ablation in very early HCC, which conforms to the criteria and for patients on waiting list for transplant20.
Transarterial chemoembolization (TACE) is usually offered as palliative treatment; however, it also has a role as a bridge to transplant in the patients who are on the waiting list. This is a minimally invasive modality of treatment which has shown definitive survival benefits, especially in those who can be categorized as intermediate BCLC B patients21. In the presence of portal vein thrombosis, transarterial radioembolization (TARE) in usually preferred22. Various forms of radiation therapy have also been used with promising results in small tumours as well as a bridge to transplantation23.
Multidisciplinary treatment for advanced disease
Unfortunately, most patients present with advanced disease, not amenable to curative treatment. Several Phase II studies have shown benefit of image-guided radiotherapy in local control and overall survival (OS) for patients with locally advanced HCC unsuitable for standard locoregional therapies2425. Three-dimensional conformal radiotherapy (3D-CRT), intensity-modulated radiation therapy (IMRT) and stereotactic body radiotherapy (SBRT) make high-dose radiation to HCC possible with sparing of the surrounding non-tumour liver parenchyma. External beam radiation therapy (EBRT) in these various forms has also been shown to increase the chances of performing a TACE. EBRT has been reported to reduce tumour size, decrease pain and also improve survival in certain studies. It has also been used as an adjunctive therapy after resection or TACE with survival benefit232627.
In the absence of trials showing a distinct benefit, the use of systemic chemotherapy in the management of HCC is not recommended outside of clinical trials7. Systemic chemotherapy may be an option for patients who progress on sorafenib and are in good physical health (BCLC stage C).
In the recent past, the only drugs with proven survival benefit were sorafenib and regorafenib in the first- and second-line therapy, respectively2829. The landscape for the treatment of advanced HCC is rapidly changing with emerging newer therapies. Atezolizumab and bevacizumab combination resulted in better OS and PFS (progression-free survical) compared to sorafenib in first-line setting and has changed practice30. Immune checkpoint inhibitors (CPI) offer promise, and the stage seems set for CPIs to become the mainstay of treatment for advanced HCC and may be also in the adjuvant setting313233. However, pembrolizumab Phase 3 trial in HCC in second-line setting did not meet its primary end point (OS and PFS)32. Sorafenib and lenvatinib have been demonstrated to be equally effective as a first-line therapy2834. Regorafenib, cabozantinib (for sorafenib-intolerant patients) and ramucirumab have shown an OS benefit in the second-line33. Supportive care involves providing support at all stages of a person's experience with cancer. Systemic therapies and their benefits are concisely shown in the Table28293032343536. This includes treatment of any underlying hepatitis, pain management, nutrition build-up, management of ascites, bleeding control and psychological support. Treatment algorithm is shown in the Figure.
| Agent | Trial | n | Comparator arm | Study population | Median OS (months) | HR | Remarks and recommendation |
|---|---|---|---|---|---|---|---|
| First-line | |||||||
| Sorafenib | SHARP trial28 Phase III | 602 | Placebo BSC | Not eligible or progressed after surgical or locoregional therapies. >90% - Child-Pugh A. 70% had microvascular invasion, extrahepatic spread or both. | 10.7 vs. 7.9 | 0.69 | One-year survival rate was 44 vs. 33%. Response rate was low, only two patients had PR with sorafenib. Recommended |
| Sorafenib | Asia-Pacific study35 Phase III | 226 (2:1) | BSC | Patients were young. Rest similar to SHARP trial | 6.5 vs. 4.2 | 0.68 | |
| Atezolizumab + Bevacizumab | IMbrave trial30 Phase III |
501 | Sorafenib | unresectable hepatocellular carcinoma who had not previously received systemic treatment, Child Pugh A ECOG PS <=1 | Not reached vs 13.2 mo | 0.58 | 1-y OS was 67.2% (95% CI, 61.3 to 73.1) with atezolizumab-bevacizumab and 54.6% (95% CI, 45.2 to 64.0) with sorafenib. Approved for first-line therapy |
| Lenvatinib | REFLECT trial34 Phase III Noninferiority |
954 | Sorafenib | Asia-pacific, Europe, North-America. ECOG PS 0, 1 Child-Pugh A | 12.3 vs. 13.6 | 0.92 | Approved for first-line therapy (previous systemic therapy was not allowed in the trial) |
| Second-line post sorafenib | |||||||
| Regorafenib | RESORCE29 Phase III trial | 573 | Placebo | Child-Pugh A | 10.6 vs. 7.8 | 0.63 | Response rate with regorafenib was 11%; 7 deaths due to regorafenib. Recommended for postsorafenib |
| Ramucirumab | REACH36 Phase III |
292 | Placebo BSC | AFP ≥400 ng/ml | 8.5 vs. 7.3 | 0.71 | Pooled analysis from REACH and REACH-2 - OS 8.1 vs. 5 months |
| Nivolumab | Phase I/II32 | 48/214 | - | 13.2 | Six month OS rate - 75%* |
Cabozantinib is approved in second-line setting (not available in India at the time of writing this manuscript). *Recommendation of nivolumab in second-line is based on Phase 2 trial. However, pembrolizumab Phase 3 trial in this setting is negative. OS, overall survival; HR, hazard ratio; BSC, best supportive care; ECOG PS, Eastern Cooperative Oncology Group performance status; AFP, alpha foetoprotein
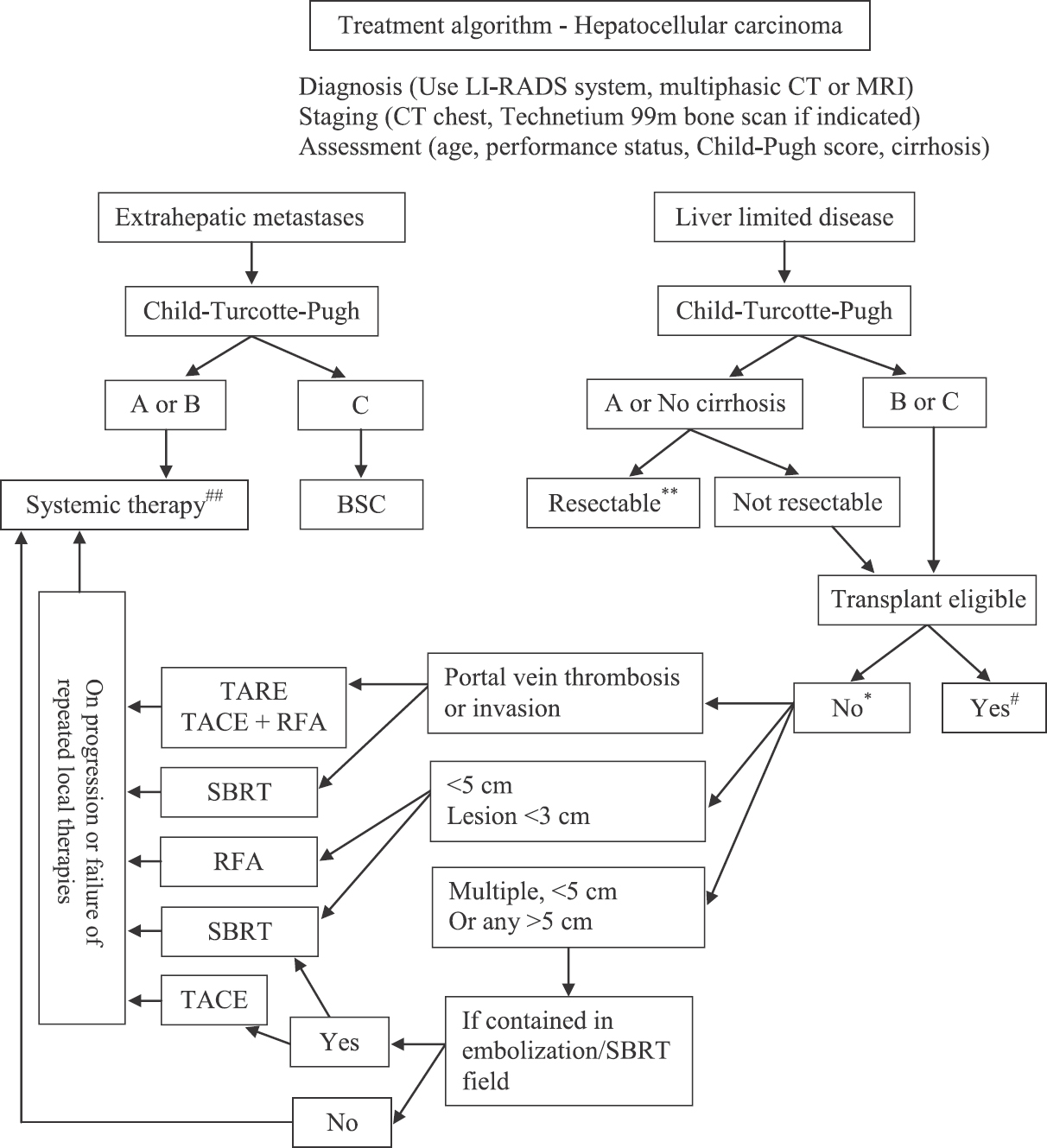
- Algorithm for the management of hepatocellular carcinoma (HCC). Local ablative therapies. RFA, radiofrequency ablation, TARE, transarterial radio embolization; TACE, transarterial chemoembolization; SBRT, stereotactic body radiotherapy. Local therapies are preferred as per institutional practices and expertise. Repeated local therapies are advocated in select cases. *For Child-Pugh C - Best supportive care (BSC) is an option. **Future liver remnant (FLR) to be ascertained. #Transplant eligible - Milan criteria to be fulfilled18. Cost, donor availability and institutional experience are other factors to be taken into consideration. ##Systemic therapies and principles of it are depicted in the Table.
The follow up of patients is recommended every three months with monitoring of AFP levels and imaging to check whether there are signs/symptoms of progression.
The following are the brief indications for various modalities for the management of HCC (to be decided after multidisciplinary consensus):
-
(i)
Liver resection: Non-cirrhotic/Child A with no or mild portal hypertension, resectable tumour with adequate FLR, BCLC A/B
-
(ii)
Liver transplantation: Cirrhosis (any Child score) with or without portal hypertension, BCLC A/B, fitting into liver transplantation criteria
-
(iii)
RFA: Up to 3 cm tumours, poor-risk surgical patients
-
(iv)
TACE: No portal venous thrombosis, BCLC B, Child A/B, outside liver transplantation criteria37
-
(v)
TARE: BCLC B, Child A/B, with portal venous thrombosis
-
(vi)
Targeted therapy: BCLC C, Child A/B
-
(vii)
Best supportive care: BCLC D (poor performance status, Child C)
Conflicts of Interest: None.
References
- EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J Hepatol. 2012;56:908-43.
- [Google Scholar]
- Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with intermediate and advanced/relapsed hepatocellular carcinoma: A TOS-ESMO initiative endorsed by CSCO, ISMPO, JSMO, KSMO, MOS and SSO. Ann Oncol. 2020;31:334-51.
- [Google Scholar]
- 2020. Liver: Globocan. Available from: https://gco.iarc.fr/today/data/factsheets/cancers/11-Liver-fact-sheet.pdf
- Cancer mortality in India: A nationally representative survey. Lancet. 2012;379:1807-16.
- [Google Scholar]
- National Centre for Disease Informatics and Research, Bengaluru. Available from: http://ncrpindia.org
- Profile of hepatocellular carcinoma in India: An insight into the possible etiologic associations. J Gastroenterol Hepatol. 2001;16:666-73.
- [Google Scholar]
- The Indian National Association for Study of the Liver (INASL) consensus on prevention, diagnosis and management of hepatocellular carcinoma in India: The Puri recommendations. J Clin Exp Hepatol. 2014;4(Suppl 3):S3-26.
- [Google Scholar]
- Economic evaluation of a surveillance program of hepatocellular carcinoma (HCC) in India. Hepatol Int. 2008;2:231-6.
- [Google Scholar]
- Antiviral therapy reduces risk of hepatocellular carcinoma in patients with hepatitis C virus-related cirrhosis. Clin Gastroenterol Hepatol. 2010;8:192-9.
- [Google Scholar]
- Utility of an immunohistochemical panel consisting of glypican-3, heat-shock protein-70, and glutamine synthetase in the distinction of low-grade hepatocellular carcinoma from hepatocellular adenoma. Appl Immunohistochem Mol Morphol. 2013;21:170-6.
- [Google Scholar]
- EASL clinical practice guidelines: Management of hepatocellular carcinoma. J Hepatol. 2018;69:182-236.
- [Google Scholar]
- Detection of hepatocellular carcinoma with PET/CT: A prospective comparison of 18F-fluorocholine and 18F-FDG in patients with cirrhosis or chronic liver disease. J Nucl Med. 2010;51:1699-706.
- [Google Scholar]
- Serum alpha-fetoprotein for diagnosis of hepatocellular carcinoma in patients with chronic liver disease: Influence of HbsAg and anti-HCV status. J Hepatol. 2001;34:570-5.
- [Google Scholar]
- EASL Panel of Experts on HCC. Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol. 2001;35:421-30.
- [Google Scholar]
- The Barcelona approach: Diagnosis, staging, and treatment of hepatocellular carcinoma. Liver Transpl. 2004;10:S115-20.
- [Google Scholar]
- Milan criteria in liver transplantation for hepatocellular carcinoma: an evidence-based analysis of 15 years of experience. Liver Transpl. 2011;17(Suppl 2):S44-57.
- [Google Scholar]
- Novel advancements in the management of hepatocellular carcinoma in 2008. J Hepatol. 2008;48(Suppl 1):S20-37.
- [Google Scholar]
- Randomized control trial of Transarterial Lipiodol chemoembolisation for unresectable hepatocellular carcinoma. Hepatology. 2002;35:1164-71.
- [Google Scholar]
- Radioembolization results in longer time-to-progression and reduced toxicity compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology. 2011;140:497-507.
- [Google Scholar]
- Efficacy and safety of external-beam radiation therapy for hepatocellular carcinoma: An overview of current evidence according to the different target population. Biosci Trends. 2019;13:10-22.
- [Google Scholar]
- Phase II study of radiotherapy employing proton beam for hepatocellular carcinoma. J Clin Oncol. 2005;23:1839-46.
- [Google Scholar]
- A comparison of treatment combinations with and without radiotherapy for hepatocellular carcinoma with portal vein and/or inferior vena cava tumor thrombus. Int J Radiat Oncol Biol Phys. 2005;61:432-43.
- [Google Scholar]
- Stereotactic body radiotherapy based treatment for hepatocellular carcinoma with extensive portal vein tumor thrombosis. Radiat Oncol. 2018;13:188.
- [Google Scholar]
- Should transarterial chemoembolization be given before or after intensity-modulated radiotherapy to treat patients with hepatocellular carcinoma with portal vein tumor thrombus? a propensity score matching study. Oncotarget. 2018;9:24537-47.
- [Google Scholar]
- Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): A randomised, double-bling, placebo-controlled, phase 3 trial. Lancet. 2017;389:56-66.
- [Google Scholar]
- Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382:1894-905.
- [Google Scholar]
- Systemic therapy for intermediate and advanced hepatocellular carcinoma: Sorafenib and beyond. Cancer Treat Rev. 2018;68:16-24.
- [Google Scholar]
- Immune checkpoint inhibitors in hepatocellular carcinoma: Opportunities and challenges. Oncologist. 2019;24:S3-10.
- [Google Scholar]
- Second-line treatments of advanced hepatocellular carcinoma: Systematic review and network meta-analysis of randomized controlled trials. J Clin Gastroenterol. 2019;53:251-61.
- [Google Scholar]
- Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomized phase 3 non-inferiority trial. Lancet. 2018;391:1163-73.
- [Google Scholar]
- Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10:25-34.
- [Google Scholar]
- Ramucirumab versus placebo as second-line treatment in patients with advanced hepatocellular carcinoma following first-line therapy with sorafenib (REACH): A randomised, double-blind, multicentre, phase 3 trial. Lancet Oncol. 2015;16:859-70.
- [Google Scholar]
- Liver transplantation for hepatocellular carcinoma: Comparison of the proposed UCSF criteria with the Milan criteria and the Pittsburgh modified TNM criteria. Liver Transpl. 2002;8:765-74.
- [Google Scholar]




