
Translate this page into:
ICMR Consensus Guidelines on ‘Do Not Attempt Resuscitation’
For correspondence: Dr Roli Mathur, ICMR Bioethics Unit, ICMR-National Centre for Disease Informatics & Research, Nirmal Bhawan, Poojanhalli, Kannamangala Post, Bengaluru 562 110, Karnataka, India e-mail: rolimath@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Cardiopulmonary resuscitation (CPR) is widely practised by healthcare professionals to revive heart beat and breathing in a patient suffering from cardiac/ respiratory arrest. It is increasingly being recognized that in some patients with specific medical conditions, CPR does not alter the overall outcome of illness, and is likely to increase suffering and further deteriorate the quality of life. Do Not Attempt Resuscitation (DNAR) as an option has been practised in many countries for such cases to avoid futile CPR and maintain dignity of the patient. The decision of DNAR should be taken by the treating physician who is well versed with the patient's medical condition, with information to the patient or her/his surrogate. While ordering DNAR on the patient's medical case record, every effort should be made to treat the underlying disease and continue optimal medical care with compassion. This policy document describes the principles for DNAR, offers an algorithm and format for its implementation, and guidance on frequently asked questions.
Background
Cardiopulmonary resuscitation (CPR) is an emergency procedure performed in an attempt to revive patients suffering from cardiac and/or respiratory arrest. It involves either or all of the following: repeated chest compression; mouth-to-mouth or artificial breathing usually with airway tube in the trachea; electric shock/s on the chest; and injectable drugs. In certain situations however, providing CPR is likely to increase the suffering of patients who have serious often terminal illness and without the prospect of a reasonable quality of life even if they are revived. Doctors and hospitals are regularly faced with the ethical dilemma of whether or not to perform CPR in such patients. Therefore, it is important to provide patients and their relatives adequate information on the disease or medical condition, poor chances of meaningful survival or worsened quality of life enable them to understand the likely benefit or potential harm of CPR in case it is required. Do not attempt resuscitation (DNAR) is an option that may be exercised by the treating physician in such a situation in the best interests of the patient. It would pave the way for arriving at an informed decision on 'DNAR' and its implementation. DNAR relates to CPR only and its limited value in certain situations and not to other forms of treatment. Whenever the treating physician is in doubt on whether to perform DNAR or not, CPR should be performed as the default option.
A core committee of experts from various disciplines was constituted to draft the guidelines, and several other experts were consulted. The guidelines were finalized through a national web based and in person consultative meeting with a wider representative audience.
Purpose
This document aims to guide treating physician(s) on their decision concerning 'DNAR'. It would help treating physician(s) and patient/surrogate(s) in preserving dignity in death and avoid prolonged suffering to the patient through non-beneficial CPR while continuing to provide other potentially curative and supportive care. Open communication and considered decision-making would enhance mutual trust and respect between the treating physician(s) and the patient/surrogate(s).
Scope
-
(i)
DNAR would apply to a patient with a progressive debilitating/incurable/terminal illness where CPR would be inappropriate, non-beneficial and likely to prolong the suffering of the patient in the best judgement of the treating physician(s). While applying this principle, compassionate care is integral to the overall goals of medical treatment.
-
(ii)
DNAR is distinct from withdrawal or withholding of other life-supporting treatments and advance directives which do not come under the purview of this document.
Instructions
The treating physician(s) should initiate discussions with the patient/surrogate and explain in detail about (i)the patient's disease and its prognosis, and (ii)the benefits and harms of CPR under the given medical circumstances in case the patient develops cardiac or respiratory arrest.
Procedure
-
The document is intended to facilitate the process of decision-making on DNAR, which that is respectful of patient's autonomy and is in the best interests of the patient by the treating physician(s) on a case-to-case basis (Figure).
-
There should be adequate opportunity, time and space to discuss with the patient and family in private and facilitate clear understanding of DNAR and its implications. Thus, it should be done in anticipation of an impending cardiorespiratory arrest, during the current hospitalization of the patient. This will allow better communication and understanding between the treating physician(s) and patient/surrogate(s)/caregiver.
-
Teamwork and good communication are of crucial importance in decision-making and the delivery of care.
-
Combined decision may be taken with the help of another physician, a psychologist or social worker or a counsellor or the hospital administrator, particularly in some settings, such as rural hospitals, where other types of personnel may not be available. This should be applicable in case the treating physician is unsure about the futility of CPR, or there is no consensus between the physician and the patient/surrogate. All such discussions must be noted in the patient's case records and the DNAR form.
-
While communicating, the treating physician(s) should explain that the patient would continue to be provided all treatments intended for potentially curable conditions or to reverse potentially reversible conditions and to provide supportive care. Moreover, DNAR does not mean withdrawal or withholding of other life-supporting treatments. The treating physician(s) should understand the social/cultural perspective of the patient.
-
DNAR forms should be available in the language understood by the patient/surrogate(s) and should be signed, timed and dated by patient/surrogate(s) and the treating physician(s). In case the patient/surrogate(s) does/do not sign the DNAR form, the same should be recorded.
-
Hospital administration should make efforts to sensitize their healthcare professionals on all issues related to DNAR.
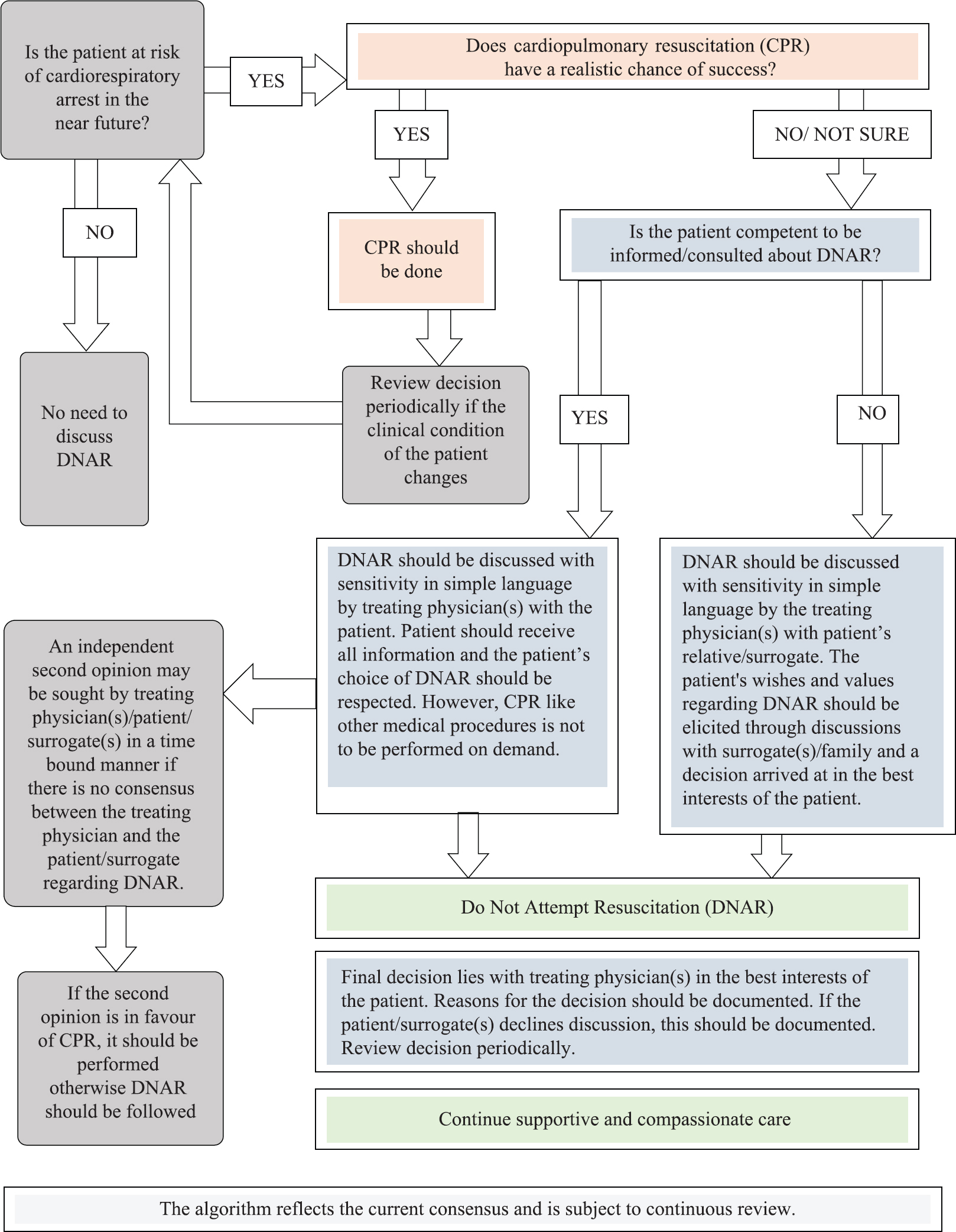
- Algorithm for Do Not Attempt Resuscitation (DNAR) decision-making.
Decision and review of decisions on DNAR
-
Since CPR is a form of treatment to be provided by the treating physician the responsibility for the final decision regarding DNAR rests with the treating physician(s), which is taken in consultation with the patient/surrogate(s), empowered with the required information. Often the patient's relatives/surrogates may face an ethical dilemma to take the decision regarding DNAR. To provide them psychological support and help them overcome any feeling of guilt, the treating physician(s) should explain to them the futility of CPR and the harm it might cause to the patient.
-
In case of conflict of opinion, an independent second opinion from a qualified medical practitioner belonging to the relevant specialty may be sought by the treating physician/patient/surrogate(s) in a timely manner.
-
Any decision taken contrary to patient's expressed wishes should based on be robust criteria, accounted for and documented in the hospital records.
Storage of DNAR forms
-
The resuscitation plans and completed DNAR forms should be easily accessible to all the medical professionals to respond appropriately in the event of cardiorespiratory arrest of the patient concerned.
-
It is recommended to attach a copy of the DNAR form to the patient's case records and to be integrated with the electronic health records, if available.
-
All the case reports along with the DNAR forms should be archived for future reference.
Acknowledgment
Authors acknowledge all stakeholders who participated in the National Consultation Meeting or provided their comments during public consultation which helped in the finalization of this Consensus Guidelines.
Conflicts of Interest: None.
References (for additional reading)
- Definition of terms used in limitation of treatment and providing palliative care at the end of life. 2018. ICMR. Available from: http://www.ncdirindia.org/Download/EOLC.pdf
- [Google Scholar]
- National Ethical Guidelines for Biomedical and Health Research Involving Human Participants. 2017. ICMR. Available from: http://ethics.ncdirindia.org//asset/pdf/ICMR_National_Ethical_Guidelines.pdf
- [Google Scholar]
- Decisions relating to Cardiopulmonary Resuscitation (3rd edition - 1st revision) Guidance from the British Medical Association, the Resuscitation Council (UK), and the Royal College of Nursing 2016
- [Google Scholar]
- DNACPR Form, Nottingham University Hospitals, National Health Service. Available from: http://dnar.co.uk/wp-content/uploads/2016/10/DNACPR-form-NUH-2014.pdf
- When and how to discuss “do not resuscitate” decisions with patients. BMJ. 2015;350:h2640.
- [Google Scholar]
- Honourable Supreme Court Judgement on Advance Directives. “Writ Petition (Civil) No. 215 of 2005”. Available from: https://main.sci.gov.in/supremecourt/2005/9123/9123_2005_Judgement_09-Mar-2018.pdf
- Ethics and medico legal aspects of “not for resuscitation”. Indian J Palliat Care. 2010;16:66-9.
- [Google Scholar]
- Limiting life-prolonging interventions and providing palliative care towards the end-of-life in Indian intensive care units. Indian J Crit Care Med. 2005;2:96-107.
- [Google Scholar]
- End-of-life care: Consensus statement by Indian Academy of Pediatrics. Indian Pediatr. 2017;54:851-9.
- [Google Scholar]
- DNR (Do Not Resuscitate) Guidelinesfor Medical ID Wearers. Available from: https://www.americanmedical-id.com/dnr
- The Scottish Government. Do Not Attempt CardiopulmonaryResuscitation (DNACPR) - Integrated Adult Policy: Guidance. The Scottish Government; May, 2010. Available from: https://www.gov.scot/publications/attempt-cardiopulmonary-resu scitation-dnacpr-integrated-adult-policy-decision-making-communication/pages/15/




