
Translate this page into:
Pancreatico-pleural fistula: An unusual cause of chronic cough
*For correspondence: shasthry@gmail.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
A 57 yr old alcoholic male† presented to the Hepatology department of the Institute of Liver and Biliary Sciences, New Delhi, India in July 2017 with chronic cough and nagging sensation on the left side of the chest for the last three months. He had already received antitubercular drugs for three months for suspected tubercular pleural effusion but without any symptomatic benefit. Computed tomography imaging of chest revealed left-sided pleural effusion (Figure A). Pleural fluid analysis showed high amylase of 2186 U/l with normal cell count, protein and negative malignant cytology. Serum amylase was normal (71 U/l). In view of the history of alcohol intake with pleural fluid analysis showing high amylase, a provisional diagnosis of pleural effusion secondary to pancreatitis was made. Computed tomographic scan of the abdomen and chest showed features suggestive of chronic calcific pancreatitis (Figure B) with massive left-sided pleural effusion. Endoscopic retrograde pancreatogram was done which demonstrated contrast leaking from the duct into the pleura (Figure C), and a stent was placed in the pancreatic duct (Figure D). The patient improved symptomatically, and cough subsided completely. Repeat endoscopic retrograde pancreatogram after three months did not show any contrast leak, and chest X-ray showed complete resolution of the pleural effusion (Figure E and F). Reactive left-sided pleural effusion is well known in acute pancreatitis, but pancreatico-pleural fistula is a rare complication of pancreatitis. Pancreatico-pleural fistula is a consequence of either leak from incompletely formed or ruptured pancreatic pseudocyst or due to direct pancreatic duct leakage. Endoscopic retrograde cholangiopancreatography with stenting helps achieve adequate pancreatic drainage and simultaneously bridges the site of ductal disruption and allows time for fistulae to close spontaneously.
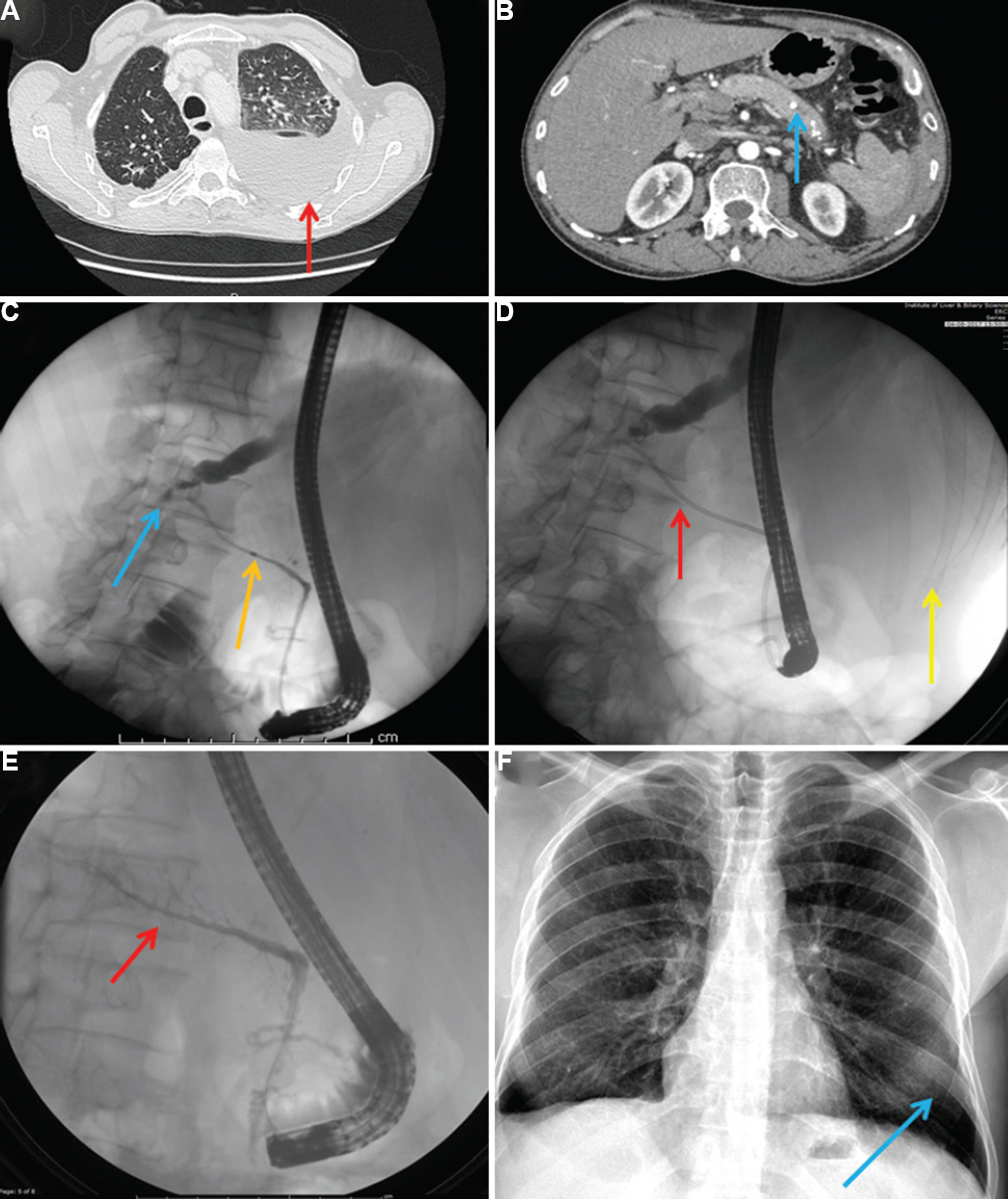
- (A and B) Computed tomographic image of chest and abdomen showing left-sided pleural effusion (red arrow in panel A) and features of chronic calcific pancreatitis (blue arrow in panel B), (C) Endoscopic retrograde pancreatogram showing leak of contrast from the main pancreatic duct (yellow arrow showing the pancreatic duct and blue arrow showing the leak), (D) Endoscopic retrograde pancreatogram showing a stent placed in the pancreatic duct (red arrow), with the patient lying in left lateral position (yellow arrow shows the ribs with the underlying lung parenchyma), (E) Endoscopic retrograde pancreatogram showing absence of leak from the main pancreatic duct (red arrow), (F) Chest X-ray showing clearance of the pleural effusion (blue arrow).
Acknowledgment
Authors thank Prof. S.K. Sarin for the technical and administrative support.
Conflicts of Interest: None.




