
Translate this page into:
Initial trends of individual donation nucleic acid testing in voluntary & replacement donors from a tertiary care centre in north India
For correspondence: Dr Neelam Marwaha, Department of Transfusion Medicine, Postgraduate Institute of Medical Education & Research, Sector-12, Chandigarh 160 012, India e-mail: neelam2918@yahoo.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Individual donation nucleic acid testing (ID-NAT) is considered as sensitive technology to assess blood safety from viral transfusion-transmissible infections (TTIs) in blood donors. The present study was aimed to analyze the results of ID-NAT for three years (2013-2015) with special reference to different types of donors and their age ranges in a tertiary care centre in north India.
Methods:
The results of ID-NAT for three years were retrospectively analyzed at our centre. A total of 168,433 donations were tested with ID-NAT, of which 10,467 were tested with Procleix® Ultrio® reagents and 157,966 were tested with Procleix® UltrioPlus® reagents, and the results were compared with those of serology to calculate the NAT yield in voluntary, replacement, first-time and repeat donors.
Results:
A combined NAT yield was observed as one in 1031 out of 167,069 seronegative donations with HBV yield as one in 1465, HCV yield as one in 3885 and HIV-1 as one in 167,069. Yield for co-infection (HCV and HBV) was one in 41,767. A high NAT yield was observed in replacement donors (1 in 498) as compared to voluntary donors (1 in 1320).
Interpretation & conclusions:
Addition of NAT to serology improved the blood safety in our centre interdicting possibility of 150 TTIs annually. It has also reemphasized the safety of voluntary over replacement donors. The results also highlight the need of proper counselling, notification and referral guidelines of NAT yield donors in our country and other countries which lack them.
Keywords
First-time donor
individual donation nucleic acid testing
nucleic acid testing yield
repeat donors
replacement donor
voluntary donor

Nucleic acid amplification technology [nucleic acid testing (NAT)] for transfusion-transmissible viral infections (TTVIs) has added a highly sensitive additional layer of safety to the blood supply. It was first introduced in Germany for hepatitis C virus (HCV) infection on whole-blood and apheresis donations1 initially on voluntary basis followed by mandatory NAT screening for hepatitis C virus (HCV) and human immunodeficiency virus-1 (HIV-1) infections. Several other developed countries across the world started NAT for HCV and HIV-1. Hepatitis B virus (HBV) screening by NAT came into global use almost a decade after HCV and HIV-1 due to concerns about sensitivity of the initial in-house assays and subsequent development of commercial multiplex test platforms23.
In India, as per the Drugs and Cosmetics Act, 1940 and the rules therein4, it is mandatory to test each donated whole blood using immunoassays for HBV surface antigen (HBsAg), anti-HCV and anti-HIV1 and 2, blood smear for the presence of malarial parasite and venereal disease research laboratory (VDRL) test for syphilis. The seroprevalence for these TTVIs in the general population in India is 0.26 per cent (0.22-0.32%) for HIV5, one per cent for HCV and 3.7 per cent for HBV6, and the average prevalence in blood donors is 0.136, 0.326 and 0.939 per cent, respectively7, though there are regional variations within the country for HIV (0-0.53%), HCV (0.03-1.40%) and HBV (0-2.57%)7. The first multicentre study8 from India highlighted this high prevalence, with a NAT yield much higher than those reported from developed countries. This has been substantiated by a few more studies from north India91011.
In the present study, the results of individual donation (ID)-NAT were analysed over a period of three years (2013-2015) with special reference to different types of donors (voluntary first-time, voluntary repeat, replacement first-time and replacement repeat donors) and in varying age ranges to understand the NAT yields and its implications for blood safety in Indian population.
Material & Methods
The present study was conducted in the department of Transfusion Medicine, Post Graduate Institute of Medical Education and Research, Chandigarh, over a period of three years (January 2013 to December 2015), during which 168,433 whole-blood donations were collected and tested for transfusion-transmissible infections (TTIs) by both serology (third-generation ELISA) and ID-NAT (Grifols Diagnostics Solution, USA) for HBV, HCV and HIV-1, based on transcription-mediated amplification (TMA) technology with analytical sensitivity of 27.6 (21.7-39.5) IU/ml for HIV-1 RNA, 3.1 (2.4-4.6) IU/ml for HCV RNA and 2.1 (1.7-3.0) IU/ml for HBV DNA12. Informed written consent of each blood donor for TTI testing was obtained. Of the total 168,433 collected donations, 10,467 samples were tested with Procleix® Ultrio® reagents (for ID-NAT) initially, and later with the availability of second-generation reagents, 157,966 donations were tested with Procleix® Ultrio Plus® reagents (Hologic, Inc., San Diego, CA, USA). NAT initial reactive (IR) samples were subjected to discriminatory testing. Serology negative and NAT-IR (potential NAT yields) which discriminated were classified as true NAT yields (discriminated NAT yield). NAT non-reactive and serology reactive samples were classified as seroyield. The NAT protocol which was followed is shown in Fig. 1.
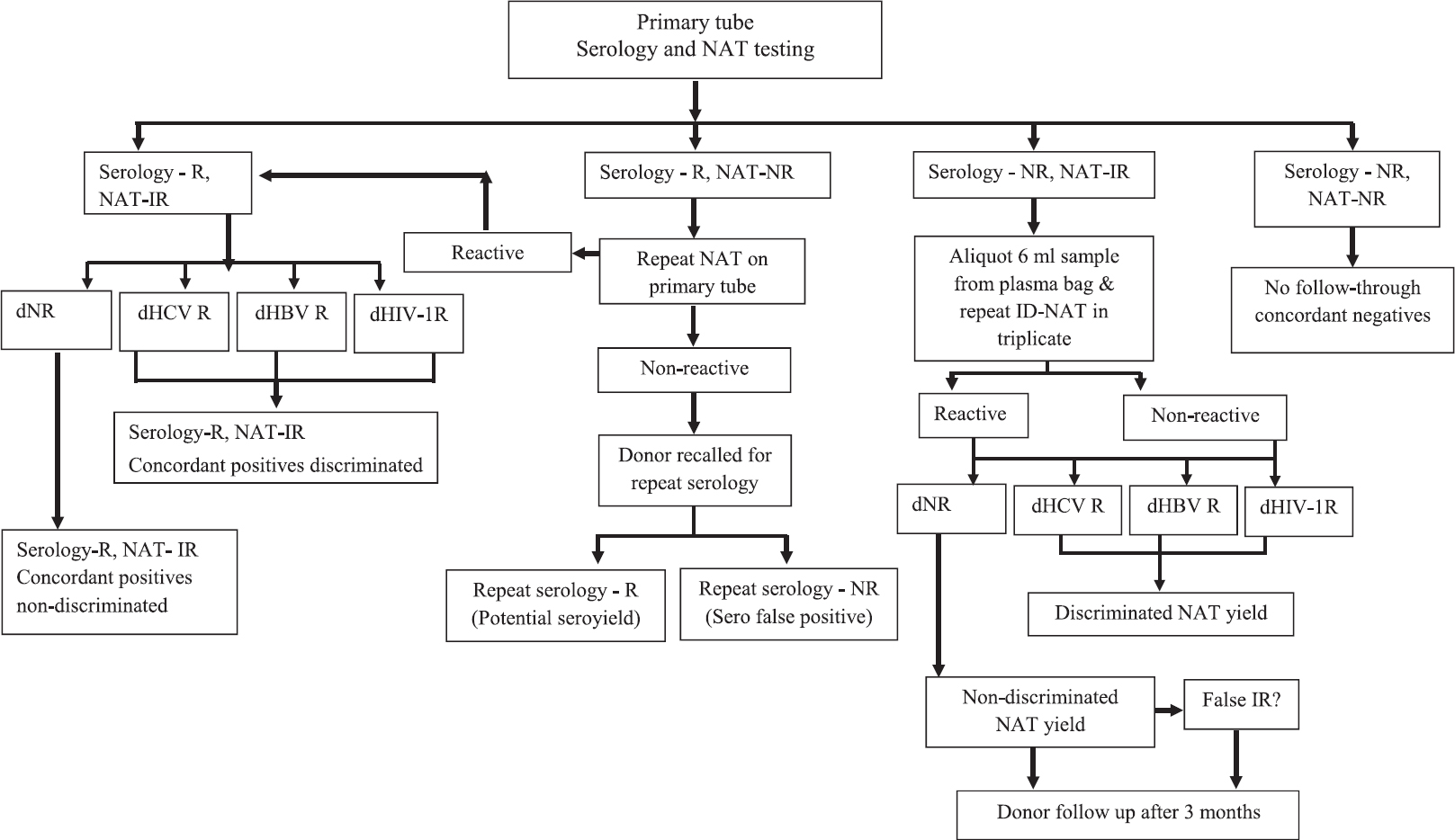
- Nucleic acid testing algorithm. IR, initial reactive; NR, non-reactive; R, reactive; d, discriminatory.
Statistical analysis was carried out using the Statistical Package for the Social Sciences version 18 (SPSS Inc., Chicago, IL, USA). Chi-square test and Fisher's exact test were applied. Odds ratio (OR) with 95 per cent confidence interval (CI) and P value were calculated.
Results
The mean annual blood collection at our centre over a period of three years was 55,102. Most of the donations were collected from the volunteers in the outdoor camps comprising 83 per cent of the total annual donations. The details of voluntary and replacement donations are given in Table I. Total numbers of donors were 157,518 for males and 10,915 for females, with a ratio of 14:1. Mean age of the donors was 28±8.7 yr (range 18-65 yr). The maximum donations were in age group of 26-35 yr.
| Type of donor | First-time donor, n (%) | Repeat donor, n (%) | Total donors, n (%) |
|---|---|---|---|
| Voluntary donor | 47,735 (34.2) | 91,718 (65.8) | 139,453 (83) |
| Replacement donor | 14,576 (50.3) | 14,404 (49.7) | 28,980 (17) |
| Total donors | 62,311 (37) | 106,122 (63) | 168,433 (100) |
NAT with different generation of reagents: Initially, Procleix® Ultrio® reagents were used and 6.2 per cent of donations were tested with these reagents whereas rest of the donations were tested with Procleix® Ultrio Plus® reagents, and the difference in means of the donations discriminated amongst the IR with Procleix® Ultrio® and Ultrio Plus® reagents was found to be significant (P<0.01) (Table II).
| Reagents | NAT-IR | NAT-discriminated (%) |
|---|---|---|
| Procleix® Ultrio® reagents | 29/10,467 (2.77 per 1000) | 4/29 (13.79) |
| Procleix® Ultrio Plus® reagents | 362/157,966 (2.29 per 1000) | 158/362 (44) |
| P | 0.32 | <0.01 |
| OR (95% CI) | 1.21 (0.82-1.76) | 0.207 (0.071-0.606) |
*OR, odds ratio; CI, confidence interval; IR, initial reactive
NAT initial reactive (IR) and discriminatory positive: Of the 168,433 donations tested over a period of three years, 1755 were NAT-IR and 391 samples which were seronegative were potential NAT yields. Of these 391 potential yields, 162 discriminated on discriminatory testing (discriminated NAT yield/true NAT yield). Hence, the combined discriminated NAT yield was 0.09 per cent (1 in 1031) out of all 167,069 seronegative donations. HBV yield was one in 1465, HCV yield was one in 3885 and HIV-1 as one in 167,069. Yield for co-infection (HCV and HBV) was one in 41,767 (Table III).
| NAT yield | Voluntary donors | P¥ | OR (95% CI) | Replacement donors | P¥ | OR (95% CI) | Total (n=167,069) | ||
|---|---|---|---|---|---|---|---|---|---|
| First time (n=47,146) | Repeat (n=91,521) | First time (n=14,485) | Repeat (n=13,917) | ||||||
| HBV | 38 (1 in 1241) | 34 (1 in 2692) | 0.001* | 2.17 (1.36-3.44) | 22 (1 in 658) | 20 (1 in 695) | 0.86 | 1.05 (0.57-1.93) | 114 (1 in 1465) |
| HCV | 11 (1 in 4286) | 20 (1 in 4576) | 0.86 | 1.06 (0.51-2.22) | 8 (1 in 1811) | 4 (1 in 3479) | 0.28 | 1.92 (0.57-6.38) | 43 (1 in 3885) |
| HIV | - | - | NA | NA | 1 (1 in 14,485) | - | 1.00$ | NA | 1 (1 in 167,069) |
| HBV + HCV (co-infection) | - | 2 (1 in 45,760) | 0.87$ | NA | - | 2 (1 in 6959) | 0.48$ | NA | 4 (1 in 41,767) |
| Total (voluntary vs. replacement donors) | 105/138, 667 (1 in 1320) | 57/28,402 (1 in 498) | 0.001♯ | 0.38 (0.27-0.52) | |||||
P value by Chi-square test, $Fisher’s exact test. NAT yields were calculated taking seronegative donations as denominator; ¥P value of first-time versus repeat voluntary and replacement donors; *HBV yield in first-time voluntary donors was significantly high than repeat voluntary donors. HIV-1 yield was only observed in first-time replacement donor and co-infection was observed in only repeat voluntary and replacement donors; ♯P value of total voluntary versus replacement donors. P value of total first time versus repeat donors=0.47 with OR of 0.87 (0.60-1.26). NA, not applicable; OR, odds ratio; CI, confidence interval
NAT yield in voluntary versus replacement and repeat versus first-time donors for HBV, HCV and HIV-1: A high combined NAT yield was observed in replacement donors (1 in 498, P<0.001) as compared to voluntary donors (1 in 1320) as shown in Table III. When comparison was done on the basis of donation status, there was no significant difference observed in NAT yield between total first-time NAT yield donors and total repeat NAT yield donors. However, HBV NAT yield in voluntary donors was significantly high in first time (P<0.001) as compared to repeat donors (Table III).
Gender and age differences in discriminated NAT yield: Of the total 157,518 male donors, NAT yield was observed in 159 (0.1%) males whereas there were three NAT yield female donors out of 10,915 total female donors (0.02%) (P<0.05). Male-to-female ratio of discriminated NAT yield was observed as 53:1 (Fig. 2).
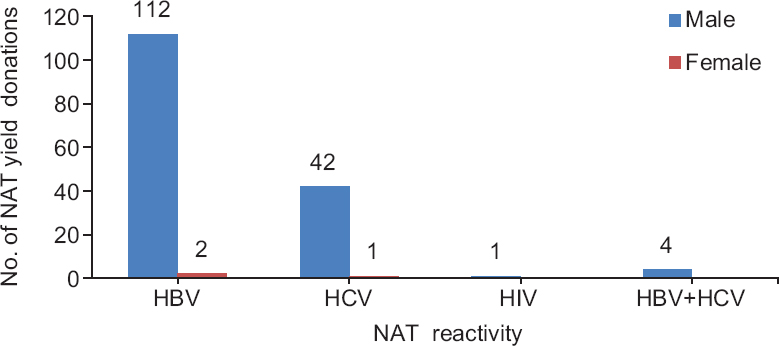
- Gender distribution of nucleic acid testing (NAT) yield donors for hepatitis B virus (HBV), hepatitis C virus (HCV) and human immunodeficiency virus-1 (HIV1).
Majority of NAT yields were observed in young donors in the age group of 26-35 yr. The yield was higher in replacement donors of all age groups as compared to voluntary donors of same group; this difference was significant in all age groups except in age group between 56-65yr (Table IV).
| Age group (yr) | NAT yield in seronegative VD | NAT yield in seronegative RD | P | OR (95% CI) |
|---|---|---|---|---|
| 18-25 | 32/44,401 (1 in 1387) | 13/8907 (1 in 685) | 0.02 | 0.49 (0.25-0.94) |
| 26-35 | 38/49,948 (1 in 1314) | 26/10,044 (1 in 401) | 0.001 | 0.29 (0.17-0.48) |
| 36-45 | 22/29,148 (1 in 1324) | 11/6066 (1 in 551) | 0.01 | 0.41 (0.20-0.85) |
| 46-55 | 8/12,369 (1 in 1546) | 7/2658 (1 in 380) | 0.01* | 0.24 (0.08-0.67) |
| 56-65 | 5/2801 (1 in 560) | Nil/727 | 0.63* | |
| Total | 105/138,667 (1 in 1320) | 57/28,402 (1 in 498) | 0.001 | 0.37 (0.27-0.52) |
P value is calculated applying Chi-square test. *Fisher’s exact test from seronegative donations. VD, voluntary donor; RD, replacement donors; NA, not applicable; OR, odds ratio; CI, confidence interval
Signal-to-cut off (S/CO) ratio of discriminated and non-discriminated NAT yields: During the three years, 391 samples were potential NAT yields, of which 162 (41%) samples discriminated (discriminated NAT yield). Of the remaining 229 samples (non-discriminated), only 101 samples (44.1%) were repeated in triplicate from fresh frozen plasma and all were repeat non-reactive. The signal-to-cut off (S/CO) ratio for discriminated samples ranged from 3.38 to 31.60, with a mean of 12.20±3.86 on initial testing (combined testing for HBV, HCV and HIV-1). Further, the mean S/CO ratios of initial NAT for samples discriminated as HBV, HCV and HIV-1 were observed as 13.16±3.31, 8.90±1.40 and 14, respectively, whereas for non-discriminated NAT yield samples, S/CO ratio of initial NAT ranged from 1.01 to 15.2, 5 with a mean of 6.94±4.70 and 128 (56%) of non-discriminated samples had S/CO ratio less than 8.9±1.40 (minimum mean discriminated S/CO value amongst the three viruses).
Concordance of NAT results with serology and seroyield: There was 71 per cent concordance of NAT results with serology; 79 per cent in HBV, 63 per cent in HCV and 71 per cent in HIV-1. Our seroyield was 0.2 per cent, highest for anti HCV followed by HBsAg as shown in Table V.
| Reactivity | Voluntary donors | P | OR (95% CI) | Total VD (n=139,453) | Replacement donors | P | OR (95% CI) | Total RD (n=28,980) | Total (VD + RD) (%) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| First time (n=47,735) | Repeat (n=91,718) | First time (n=14,576) | Repeat (n=14,404) | ||||||||
| HBsAg | 17 (1 in 2808) | 20 (1 in 4586) | 0.13 | 1.63 (0.85-3.11) | 37 (1 in 3769) | 11 (1 in 1325) | 9 (1 in 1601) | 0.67 | 1.20 (0.50-2.91) | 20 (1 in 1449) | 57 (16.91) |
| Anti-HCV | 58 (1 in 823) | 121 (1 in 758) | 0.60 | 0.92 (0.67-1.25) | 179 (1 in 779) | 32 (1 in 456) | 40 (1 in 360) | 0.32 | 0.79 (0.49-1.25) | 72 (1 in 402) | 251 (74.48) |
| Anti HIV1/2 | 6 (1 in 7956) | 13 (1 in 7055) | 0.80 | 0.88 (0.33-2.33) | 19 (1 in 7340) | 5 (1 in 2915) | 4 (1 in 3601) | 0.99* | 1.23 (0.33-4.60) | 9 (1 in 3220) | 28 (8.3) |
| Co-infection (anti HCV and HBsAg)# | 1 (1 in 47735) | - | 0.99* | - | - | - | - | - | - | 1 (0.29) | |
P value by Chi-square test, *Fisher’s exact test. #Co-infection was observed in first-time voluntary donor only. VD, voluntary donors; RD, replacement donors; NA, not applicable; CI, confidence interval; OR, odds ratio; HBsAg, hepatitis B virus surface antigen; HCV, hepatitis C virus
Discussion
The previous studies from India reported NAT yields from predominantly replacement donors; however, the present study reflected NAT yields in a predominantly voluntary donor population as well as donation status ( first-time versus repeat donors) and age range of the donors. In a review13, the authors compiled all the published studies on NAT from India and showed that NAT data were available on a total of 389,367 units, whereas our study (over a period of 3 years) from a single centre contributed NAT data of 168,433 units. A combined NAT yield of 0.09 per cent (1 in 1031) was observed in our study which indicated that around 50 donations annually were missed by serology alone. Thus, with addition of NAT, we could save 150 patients annually from the risk of TTIs as we have 100 per cent component preparation policy at our centre. This yield was higher when compared with reported yield from other countries as shown in Table VI. Our observed NAT yield was higher than most of the previously reported NAT yields in different studies from India (Table VII). The highest NAT yield (1 in 610) was reported by Agarwal et al11 which was higher than the NAT yields reported in different Indian studies (Table VII).
| Study | Country | Donations | NAT yield |
|---|---|---|---|
| Hourfar et al, 20081 | Germany | 31,524,571 | 1 in 10.88 million (HCV) |
| 1 in 4.30 million (HIV) | |||
| 1 in 360,000 (HBV) | |||
| Ohnuma et al, 200114 | Japan | 6,805,010 | 1 in 2,722,000 (HCV) |
| 1 in 1,701,253 (HIV) | |||
| 1 in 60,759 (HBV) | |||
| Zou et al, 201015 | USA | 66 million | 1 in 1,149,000 (HCV) |
| 1 in 1,467,000 (HIV) | |||
| Kalibatas and Kalibatienė 201416 | Lithuania | 300,773 | 33.94 in 100,000 (HBV) or (1 in 2946) |
| 21.51 in 100,000 (HCV) or (1 in 4649) | |||
| El Ekiaby et al, 200917 | Egypt | 15,655 | 1:3100 (Combined yield for all 3 viruses) |
| Dong et al, 201418 | China | 178,447 | 1 in 1056 (HBV) |
| Naizi et al, 201519 | Pakistan | 56,772 | 1 in 2016 (Combined yield for all 3 viruses) |
| 1 in 2367 (HBV) | |||
| 1 in 13,609 (HCV) | |||
| Present study | India | 168,433 | 1 in 1031 (Combined yield for all 3 viruses) |
HBV, hepatitis B virus; HCV, hepatitis C Virus; HIV, human immunodeficiency virus
| Study, year | Number of donations tested | . | NAT format | Types of donors (%) | % NAT yield |
|---|---|---|---|---|---|
| Makroo et al, 20088 | 12,224 | ID-NAT | Replacement donors (74) | 0.065 (1 in 1528) | |
| Jain et al, 20129 | 23,779 | MP-NAT | Voluntary donors (84.65) | 0.034 (1 in 2972) | |
| Chatterjee et al, 201210 | 18,354 | ID-NAT | Replacement donors (50) | 0.038 (1 in 2622) | |
| Agarwal et al, 201311 | 73,898 | ID-NAT | Replacement donors (67) | 1.49 (1 in 610) | |
| Pathak & Chandrashekhar, 201321 | 6587 | MP-NAT | Not specified | 0.045 (1 in 2195) | |
| Chigurupati & Murthy, 201520 | 15,000 | MP-NAT | Not specified | 0.05 (1 in 2000) | |
| Present study | 168,433 | ID-NAT | Voluntary donors (83) | 0.09 (1 in 1031) |
ID-NAT, individual donation nucleic acid testing; MP-NAT, minipool nucleic acid testing
Most of our donations were from male donors; therefore, high NAT yield was observed in young males. Further, the yield was high in 25-35 yr age group as majority of donations were from donors of this age group, which has implications for blood safety in India in the coming decades when this population will constitute major base for blood donation. Lower NAT yield was observed in higher age group because of small number of donations in that group. Previous studies from our region also showed high seroprevalence of TTIs in young males which could be attributed to high injectable drug users in the region (16.6% HIV, 17.8% HBV and 33.7% HCV)2223.
The NAT yield in study by Agarwal et al11 was higher than that of our study as majority of their donations (62.5%) were from replacement donors, whereas in our study, 83 per cent donations were from voluntary donors. However, in the present study, we also observed a high NAT yield in replacement donors as compared to voluntary donors. The NAT yield for HBV was high in our study (more in first-time donors) which could reflect the ability of ID-NAT to pick up donors in the serological window period of third-generation ELISA testing for HBsAg or donors with occult hepatitis B in our donor population. In addition, a few of these could actually represent the ability of NAT to pick up serosilent blood donors and either HBV vaccine escape mutants or mutants of immune pressure24. With the introduction of second-generation reagents (Procleix® UltrioPlus®) for NAT, HBV yield had increased in our study as compared to previous Indian studies where first-generation reagents were used for testing.
In the present study, we observed high anti-HCV seroyield (74.48%), NAT was again repeated on these samples at three months of follow up and the results were still non-reactive. As per the CDC USA recommendations25, at least six months follow up is required. Hence, the reason for high anti-HCV seroyield could not be ascertained whether this was a false positivity due to ELISA kits as suggested by Tulsiani et al26. In our study, the NAT was on TMA platform, and repeat testing could not be done on a PCR system which was a limitation of the study.
The seroyield for HBsAg was 16 per cent in our study. Allain et al27 explained the reason of non-concordant hepatitis B seropositive samples as the considerable difference between the release of viral structural proteins and the formation of full virions released in the circulation. They have mentioned that non-encapsidated viral DNA tends to be rapidly destroyed; whereas in the absence of anti-HBs, surface antigen produced by either infected cells or integrated viral genome may remain in circulation for prolonged periods of time leading to HBsAg seroyield.
In our study, only discriminated samples were considered as true NAT yield excluding samples which were IR but did not discriminate; however, these donation units were removed from the inventory as done by Makroo et al8. In a five-year experience of NAT, Chatterjee et al28 mentioned 13.04 per cent NAT-IR units to be non-reactive with the primary pilot tube itself on repeat testing and 0.71 per cent NAT-IR units were found to have at least one repeat reactive result, even then 6.98 per cent NAT-IR units in their study could not be discriminated. In our study, 59 per cent samples were NAT-IR but not discriminated, of which 44 per cent samples were repeated in triplicate from plasma bag after thawing which were repeat non-reactive, remaining could not be repeated from plasma bags because those were discarded before sampling for repeat NAT. There was difference between our NAT algorithm and algorithm of Chatterjee et al28 as they did discriminatory testing in triplicate whereas we performed discriminatory test for single time. Previous studies from India (Table VII) did not mention their NAT protocol so could not be compared with our algorithm.
A total of 128 non-discriminated samples in our study had initial S/CO below the value of discriminated samples, suggesting false positivity or sampling error or Poisson effect; however, this could not be proved as samples were not repeat tested in triplicate or confirmed by PCR which was another limitation of the study. Furthermore, most of the donors could not be followed up for repeat sampling and testing at an interval of 3-6 months because of difficulty in convincing these donors to come for repeat sampling and testing. Some of these donors came back with non-reactive repeat test results from private laboratories by ELISA method and did not consent for repeat sampling. Moreover, our national blood policy does not have any guidelines of recalling donors whose donation sample was seronegative but NAT-IR, this was also highlighted by Chaurasia et al29. Keeping this issue in view and large number of unsolved non-discriminated NAT yields, it can be proposed to perform discriminatory runs in triplicate from the plasma bag samples of NAT yield and to repeat reactive samples so as to counter the Poisson effect or sampling error or false positivity due to primary tube contamination.
Thus, addition of NAT with serology testing in our setup improved the blood safety by picking up 50 donations/year which were missed by serological method and thus interdicting possibility of 150 TTIs annually. This study highlights the need for adapting uniform testing algorithms throughout the country to have uniform reporting. Second, it addresses the issue of high NAT yield in young donors who can be potential repeat donors in the future and the need to formulate national guidelines for notification and counselling of NAT yield donors with proper referral to further decrease the prevalence of TTVIs and helping donors with timely medical care. Third, our study also adds substantially to NAT yield data in the country where around 11-12 million blood units are collected annually and total published NAT data is available for only around 0.4 million blood units13 tested for NAT.
Financial support & sponsorship: None.
Conflicts of Interest: None.
References
- Experience of German Red Cross blood donor services with nucleic acid testing: Results of screening more than 30 million blood donations for human immunodeficiency virus-1, hepatitis C virus, and hepatitis B virus. Transfusion. 2008;48:1558-66.
- [Google Scholar]
- 2008. Patients for Patient Safety News No. 11. Available from: http://www.who.int/patientsafety/patients_for_patient/news/PFPS_News_No11_April_2008.pdf
- Part XIIB. The Drugs and Cosmetics Act, 1940 and the Drugs and Cosmetics Rules, 1945. Government of India, Ministry of Health and Family Welfare, Department of Health. 2005. :326. Available from: http://www.cdsco.nic.in/Drugs&CosmeticAct.pdf
- [Google Scholar]
- Annual report 2015-2016. National AIDS Control Organisation, Ministry of Health and Family Welfare, Government of India. Available from: http://www.naco.gov.in/NACO/Quick_Links/Publication/Annual_Report/NACO_Annual_Report/Annual_Report_NACO_2015-16_English/
- Hepatitis in India – National Centre for Disease Control. Available from: http://www.ncdc.gov.in/writereaddata/linkimages/NewsLtr0103_20146480274026.pdf
- Assessment of NACO Supported Blood Banks – A Preliminary Report 2016. Government of India, Ministry of Health and Family Welfare. Available from: http://www.naco.gov.in/sites/default/files/Assessment%20of%20NACO%20supported%20BBs%20in%20India.pdf
- Multicenter evaluation of individual donor nucleic acid testing (NAT) for simultaneous detection of human immunodeficiency virus -1 & hepatitis B & C viruses in Indian blood donors. Indian J Med Res. 2008;127:140-7.
- [Google Scholar]
- Need for nucleic acid testing in countries with high prevalence of transfusion-transmitted infections. ISRN Hematol. 2012;2012:718671.
- [Google Scholar]
- Individual donor nucleic acid testing for blood safety against HIV-1 and hepatitis B and C viruses in a tertiary care hospital. Natl Med J India. 2012;25:207-9.
- [Google Scholar]
- Nucleic acid testing for blood banks: An experience from a tertiary care centre in New Delhi, India. Transfus Apher Sci. 2013;49:482-4.
- [Google Scholar]
- Procleix Ultrio plus assay-complete Nucleic Acid Testing. Available from: http://www.novartisdx.com/products/procleixassays/ultrio-plus.shtml
- Nucleic acid amplification testing in Indian blood banks: A review with perspectives. Indian J Pathol Microbiol. 2017;60:313-8.
- [Google Scholar]
- The first large-scale nucleic acid amplification testing (NAT) of donated blood using multiplex reagent for simultaneous detection of HBV, HCV, and HIV-1 and significance of NAT for HBV. Microbiol Immunol. 2001;45:667-72.
- [Google Scholar]
- Prevalence, incidence, and residual risk of human immunodeficiency virus and hepatitis C virus infections among United States blood donors since the introduction of nucleic acid testing. Transfusion. 2010;50:1495-504.
- [Google Scholar]
- The results of nucleic acid testing in remunerated and non-remunerated blood donors in Lithuania. Blood Transfus. 2014;12(Suppl 1):s58-62.
- [Google Scholar]
- The impact of different HCV blood screening technologies on the reduction of transfusion transmitted HCV infection risk in Egypt. Vox Sang. 2009;96(Suppl 2C-S08-03):23-4.
- [Google Scholar]
- A pilot study on screening blood donors with individual-donation nucleic acid testing in China. Blood Transfus. 2014;12:172-9.
- [Google Scholar]
- Impact of nucleic acid amplification test on screening of blood donors in Northern Pakistan. Transfusion. 2015;55:1803-11.
- [Google Scholar]
- Automated nucleic acid amplification testing in blood banks: An additional layer of blood safety. Asian J Transfus Sci. 2015;9:9-11.
- [Google Scholar]
- Transfusion transmittable infections – Seroprevalence among blood donors in a tertiary care hospital of Delhi. Asian J Transfus Sci. 2013;7:116-8.
- [Google Scholar]
- Prevalence of human immunodeficiency virus (HIV), hepatitis B virus, and hepatitis C virus in three groups of populations at high risk of HIV infection in Amritsar (Punjab), Northern India. Jpn J Infect Dis. 2008;61:79-81.
- [Google Scholar]
- Epidemiological profile of seropositive blood donors at a tertiary care hospital in North India. CHRISMED J Health Res. 2014;2:91-4.
- [Google Scholar]
- Hepatitis B virus (HBV) and s-escape mutants: From the beginning until now. J Hum Virol Retrovirol. 2015;2:00046.
- [Google Scholar]
- Blood donor counselling Implementation guidelines. Available from: https://www.who.int/bloodsafety/voluntary_donation/Blooddonorcounselling.pdf
- True positivity of anti-hepatitis C virus enzyme-linked immunosorbent assay reactive blood donors: A prospective study done in Western India. Asian J Transfus Sci. 2012;6:165-8.
- [Google Scholar]
- Lack of correlation between hepatitis B surface antigen and hepatitis B virus DNA levels in blood donors. Transfusion. 2005;45:1039-40.
- [Google Scholar]
- Five years of experience with ID-NAT at a tertiary care centre in North India: An interdictory step in preventing the transfusion-transmitted infections. ISBT Sci Ser. 2016;11:38-44.
- [Google Scholar]
- Screening donated blood for transfusion transmitted infections by serology along with NAT and response rate to notification of reactive results: An Indian experience. J Blood Transfus. 2014;2014:412105.
- [Google Scholar]




