
Translate this page into:
Addition of power Doppler to grey scale transvaginal ultrasonography for improving the prediction of endometrial pathology in perimenopausal women with abnormal uterine bleeding
For correspondence: Dr P Veena, No. 11, Type DII quarters, JIPMER Campus, Dhanvantari Nagar, Puducherry 605 006, India e-mail: veenup_2001@yahoo.com
-
Received: ,
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Transvaginal ultrasonography (TVS) is a non-invasive procedure and can be used as a screening tool among women with abnormal uterine bleeding (AUB). Power Doppler is useful in depicting the vascular architecture better than the conventional Doppler. Hence, this study was conducted to evaluate whether addition of power Doppler to grey scale TVS can replace invasive hysteroscopy for the prediction of endometrial pathology in perimenopausal women with AUB.
Methods:
One hundred women (>45 yr) with perimenopausal AUB underwent evaluation with TVS, power Doppler and hysteroscopy-guided biopsy after a detailed history and examination. Histopathology was considered as gold standard and other tools such as grey scale TVS with power Doppler and hysteroscopy were compared with it.
Results:
Fifty six per cent women had no vascularity on power Doppler. Among those who had vascularity, the vascular patterns noted were single-vessel in 18 per cent, scattered-vessel in 15 per cent and multiple-vessel in 11 per cent. The sensitivity, specificity, positive predictive value and negative predictive value of TVS-endometrial thickness with power Doppler in detecting hyperplasia were 50, 86.5, 13.3 and 97.6 per cent, respectively, whereas the same for hysteroscopy were 100, 97.6, 88.1 and 100 per cent, respectively.
Interpretation & conclusions:
Addition of power Doppler to grey scale TVS improved the specificity and negative predictive value almost comparable to hysteroscopy for evaluation of AUB, but sensitivity and positive predictive value remained poor.
Keywords
Abnormal uterine bleeding
endometrial carcinoma
endometrial polyp
hysteroscopy
power Doppler
transvaginal ultrasonography

Abnormal uterine bleeding (AUB) at any age in a woman's life is disruptive and worrisome and is more common in perimenopausal age group1. Although anovulation is the most common endometrial cause, endometrial adenomatous polyps, endometrial hyperplasia and carcinoma are the other important causes. Hence, pre- and postmenopausal women with AUB require careful evaluation to rule out endometrial malignancy.
Although postmenopausal bleeding (PMB) is a common complaint2 accounting for up to 69 per cent of postmenopausal women referred to the gynaecological outpatient department1, only 10-15 per cent of them will actually have endometrial carcinoma3. Hence, subjecting the rest of the women whose examination reveals no abnormality on invasive endometrial biopsy becomes questionable. Thus, there is a need for an efficient non-invasive technique that can predict endometrial pathologies.
Transvaginal ultrasonography (TVS) is a non-invasive procedure and can be used as a screening tool. TVS allows visualizing the endomyometrial interface and the entire cavity. TVS measurement of endometrial thickness (ET) has high negative predictive value and can avoid unnecessary biopsies. According to a study by Dijkhuizen et al4, TVS can prevent around 40 per cent of endometrial biopsies. ET when combined with some morphologic parameters and Doppler velocimetry studies can improve the diagnostic accuracy of TVS in patients with PMB5.
Power Doppler is a new technology, based on the amplitude of Doppler signal and not on Doppler frequency shift that makes it more sensitive to low-velocity blood flow. Hence, it is useful in depicting the vascular architecture6 better than the conventional Doppler. There are a few studies which suggested that power Doppler vascular pattern can be used to predict endometrial pathology in postmenopausal women with PMB678.
The present study was aimed to evaluate the role of transvaginal ultrasound with power Doppler studies to predict endometrial pathologies as against gold standard hysteroscopy-guided biopsy in the pre- and postmenopausal women with AUB.
Material & Methods
This prospective study was conducted between December 2013 and May 2015 in Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry, a tertiary care centre in south India. One hundred women with premenopausal AUB (women aged above 45 yr with excessive bleeding or any deviation from normal frequency or cyclicity) or PMB were included in the study after taking informed written consent. The study protocol was approved by the Institute's ethics committee. The study by El-Morsi et al7 noted that the positive predictive value of power Doppler in predicting polyp and hyperplasia was 68 per cent. The sample size was calculated based on this positive predictive value of 68 per cent, expected precision of 10 per cent, alpha error of 0.05 and 10 per cent attrition.
Women with other apparent causes of AUB which were unlikely to be due to endometrial pathology (women on hormone replacement therapy/anticoagulants, known cases of thyroid dysfunction, chronic renal diseases, chronic liver diseases and haematological diseases and women with clinical evidence of cervical cancer, cervical polyp, fibroid and adenomyosis) were excluded.
A detailed history was taken and a systematic examination was performed. The different clinical parameters noted were age, parity, presenting complaints which included severity and duration, menstrual history that included age at menarche, regularity, duration and severity of flow, age at menopause, presence of inter-menstrual bleeding, dysmenorrhoea, comorbid illness such as diabetes, hypertension, history of surgery or significant illness and family history of malignancy. Examination parameters such as body mass index (BMI), any mass per abdomen, findings of per speculum and vaginal examination (the size of uterus and the presence of adnexal mass) were also noted.
On the same day or within two days of the first visit, TVS was performed using a 7.5 MHz probe of Voluson Pro 730 from GE (General Electric, USA) healthcare, India. Initially, grey scale examination was done to note the uterine length, width, ET, endomyometrial interphase, presence of intra-cavitary fluid and presence of adnexal lesion. Then, power Doppler was activated. The following settings were ensured: pulse repetition frequency between 0.3 and 0.9 KHz (usually 0.6) and wall filter 30-50 Hz. Gain was adjusted such that artefacts were minimal or absent. The vessel pattern was noted.
Within one week of TVS, hysteroscopy-guided biopsy was scheduled as a minor operation theatre procedure. A 5 mm Karl Storz rigid hysteroscope (Karl Storz, Germany) was used. Normal saline (0.9%) was used as the distension medium. The endocervical canal, endometrial cavity, anterior, posterior, lateral walls and fundus of the uterus were also examined systematically. Special attention was paid to the areas where increased vascularity was noted on the TVS. If there was a suspicious growth, biopsy was taken using biopsy forceps which was introduced through the biopsy port. If there was no evidence of focal lesion, a thorough curettage of the endometrial cavity was done. Hysteroscopy was reported as atrophic, normal, focal abnormality such as polyp, myoma and growth or diffuse hyperplasia. Endometrial hyperplasia was classified as hyperplasia without atypia and hyperplasia with atypia according to the WHO classification9 not according to the original Kurman's classification10. The histopathology report was collected.
Statistical analysis: Statistical analysis was done using SPSS software version 13 (IBM Corporation, USA). Continuous data such as age, age at menarche and age at menopause are expressed as mean±standard deviation. Categorical data such as parity, comorbidities and BMI are expressed as median with range. The mean uterine length, width and ET of malignant and premalignant lesions were compared with other benign lesions using independent Student's t test. The predictive power of TVS was determined by calculating the sensitivity, specificity, positive predictive value and negative predictive values using the cross-tabulations. The significance (P) of these data was calculated using Fisher's exact test.
Results
Of the 100 women included, 46 were postmenopausal and the average age at menopause was 52.6±6 yr, the remaining 54 were premenopausal. The mean age of the women included in the study was 50.4±5.48 yr. The median parity of women was 2.5 (range 0-7). Majority of the women were multiparous (94%). The mean BMI was 26.29±4.14 kg/m2. More than half of the women (55%) were obese and around one-fourth (28%) were in the overweight category.
In the postmenopausal group, the median duration of menopause before the presenting symptom was four years (range: 1-25 yr). Most of the women (67.39%) had PMB within five years of menopause (n=31). Around 20 per cent of women had bleeding after five years but before 10 yr of menopause (n=9); only two women had PMB after 15 yr of menopause. Majority of postmenopausal women (74%) presented within three months of symptoms (n=34) as against 24 per cent in the premenopausal group (n=13). It was observed that more than half (51.8%) of premenopausal women approached higher institute after six months of the complaint (n=28).
These women were subjected to TVS with power Doppler, hysteroscopy and guided biopsy/thorough endometrial curettage. The histopathological report was considered as the gold standard and the predictive power of various diagnostic tools was evaluated. The diagnostic tools assessed in the study were grey scale transvaginal ultrasound, power Doppler pattern and hysteroscopy. Table I depicts the distribution of various histopathological diagnoses of AUB in post- and premenopausal groups.
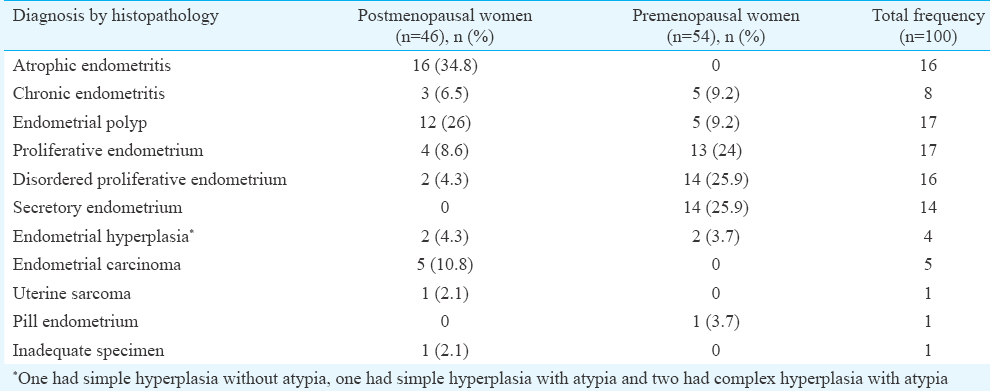
Transvaginal ultrasound: The most important parameter in grey scale ultrasound is ET. ET is commonly expressed in millimetre (mm). ET of >4 mm in the postmenopausal women and >8 mm in the premenopausal women was considered as thick endometrium. Twenty six per cent of women in premenopausal group (n=14) and 61 per cent in postmenopausal group (n=28) had thick endometrium. Apart from ET, other parameters measured were uterine height and width; other findings such as the intra-uterine fluid collection, myoma and endometrial polyps were also noted. The mean uterine length, width and ET were higher in women with hyperplasia and carcinoma when compared to others. The difference was significant only for uterine width (5.1±0.95 cm vs. 4.5±0.73 cm, P=0.01).
Endometrial polyps were observed in three per cent, intrauterine fluid collection in three per cent myoma in five per cent. Among three patients who had intrauterine fluid collection, the final diagnosis was uterine sarcoma, endometrial carcinoma and atrophic endometrium. The distribution of ET in various histopathological reports is depicted in Fig. 1.
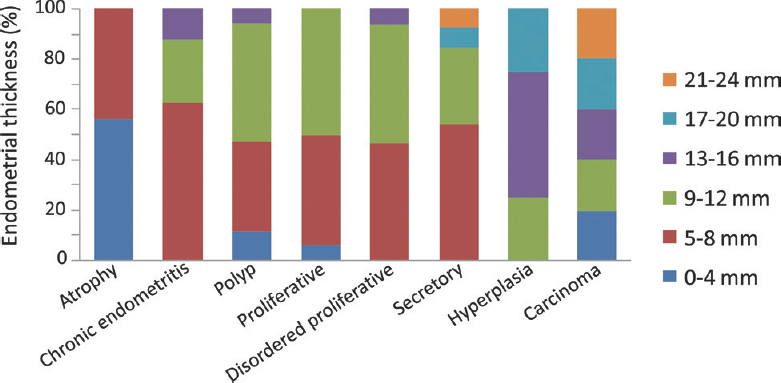
- Distribution of endometrial thickness in various histopathological diagnoses.
Twenty six per cent of women in the premenopausal and 61 per cent in the postmenopausal group had thickened endometrium. Except one case, all other women with endometrial carcinoma had ET ≥4 mm. All cases of endometrial hyperplasia had abnormal ET. Considering the cut-off as ≥4 mm, the predictive power of TVS was calculated (Table II). Among premenopausal women with AUB, there is no consensus on the ET cut-off. Hence, different cut-offs were used and predictive power of ET was calculated. The cut-offs used were ≥8 and ≥12 mm (Table II). There were only two cases of hyperplasia in the premenopausal group. It was evident from Table II that if the cut-off was increased to ≥12 mm, it had a higher specificity without altering the sensitivity.

Power Doppler: The vascularity of endometrium was assessed using power Doppler. More than half of the women (56%) had no vascularity. Among women who had vascularity, 18 per cent had single-vessel, 15 per cent had scattered-vessel and 11 per cent had multiple-vessel pattern. Of the 18 women who had single-vessel pattern (Fig. 2), nine had polyp. The other diagnoses were atrophy (1), proliferative endometrium (2), disordered proliferative endometrium (3), secretory endometrium (1) and endometrial carcinoma (2). In 15 women who had scattered-vessel pattern, the final diagnoses were disordered proliferative endometrium (4), proliferative endometrium (3), secretory endometrium (3), uterine sarcoma (1), chronic endometritis (2) and endometrial hyperplasia (2). In those who had multiple-vessel pattern (Fig. 3), the final histopathological diagnoses were proliferative endometrium (4), disordered proliferative endometrium (2), hyperplasia (1), carcinoma (3) and chronic endometritis (1).
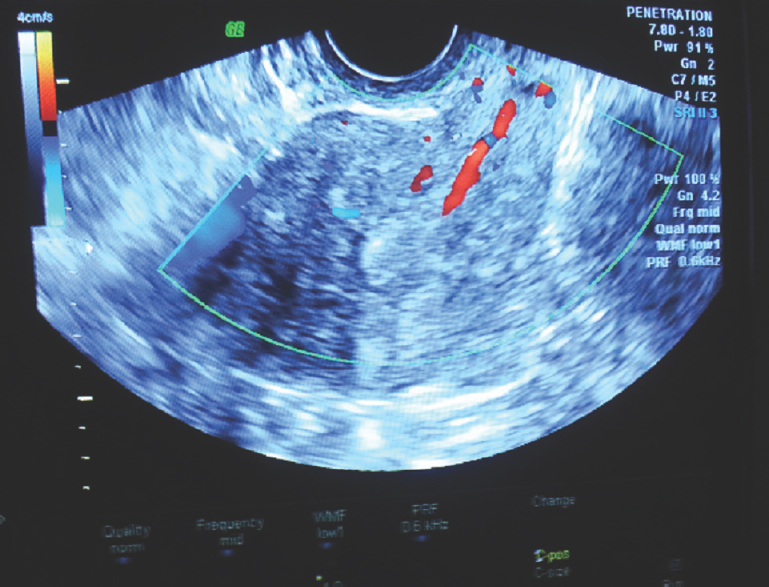
- Single-vessel pattern.
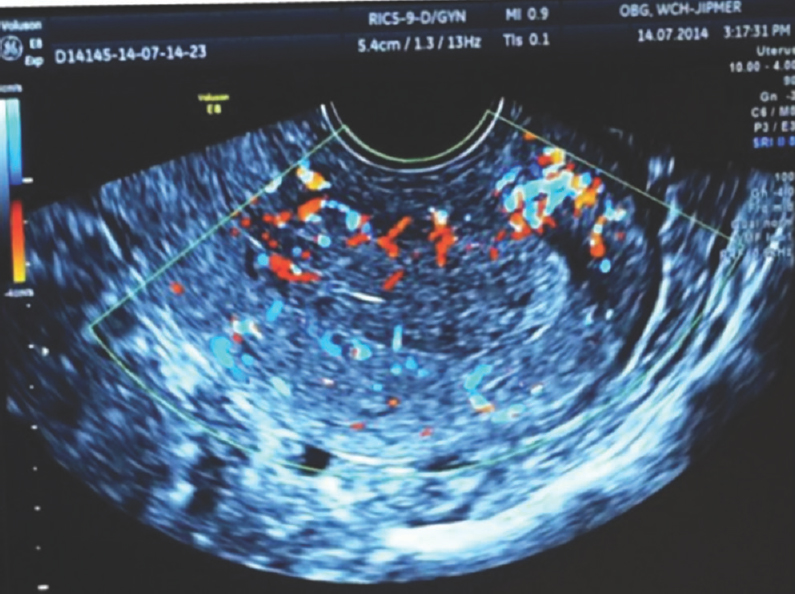
- Multiple-vessel pattern.
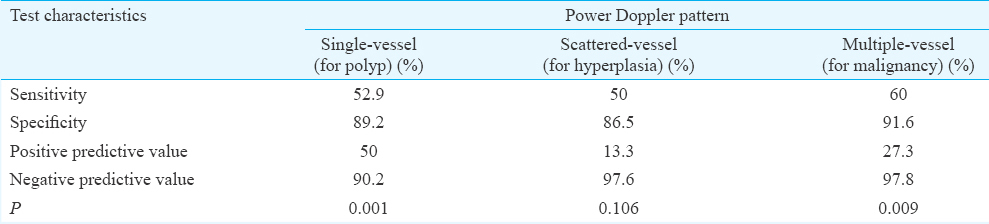
Taking hysteroscopic-guided biopsy as gold standard, the efficacy of power Doppler patterns was compared. Single-vessel, scattered-vessel and multiple-vessel patterns could predict polyp, hyperplasia and carcinoma, respectively (Table III). The negative predictive values were more than 90 per cent, which implied that the presence of pathology in the absence of vascularity was less likely. The positive predictive values of detecting hyperplasia and carcinoma based on the vascularity were low because of the lesser number of cases. There were only four cases of hyperplasia and five cases of carcinoma. If abnormal ET and power Doppler pattern were combined, the specificity of detecting hyperplasia increased to 89.6 per cent and the specificity of detecting carcinoma increased to 92.6 per cent.
Hysteroscopy: Hysteroscopic observations were recorded as atrophy, normal, focal or diffuse abnormality. The classic description of chronic endometritis is micro polyps, stromal oedema and increased vascularity. This finding was noted in three of eight women who had chronic endometritis on histopathological examination. Predictive values for hysteroscopy are mentioned in Table IV.

Irrespective of the diagnosis, hysteroscopy had high negative predictive value. The sensitivity was 100 per cent in diagnosing atrophy, polyp (Fig. 4) and hyperplasia (Fig. 5). The sensitivity of detecting carcinoma was 60 per cent because there was one case (out of four) who had malignancy in the polyp. The positive predictive value for hyperplasia was less (26.7%). Of the 15 patients who had hyperplasia on hysteroscopy, only four had hyperplasia eventually on histopathology. Five patients had proliferative endometrium, three had disordered proliferative, two had secretory endometrium and one had endometrial carcinoma.
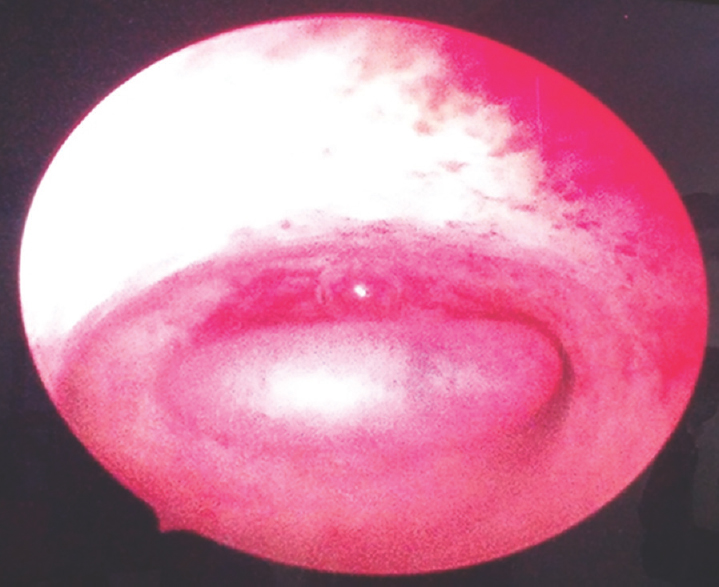
- Hysteroscopic view of endometrial polyp.
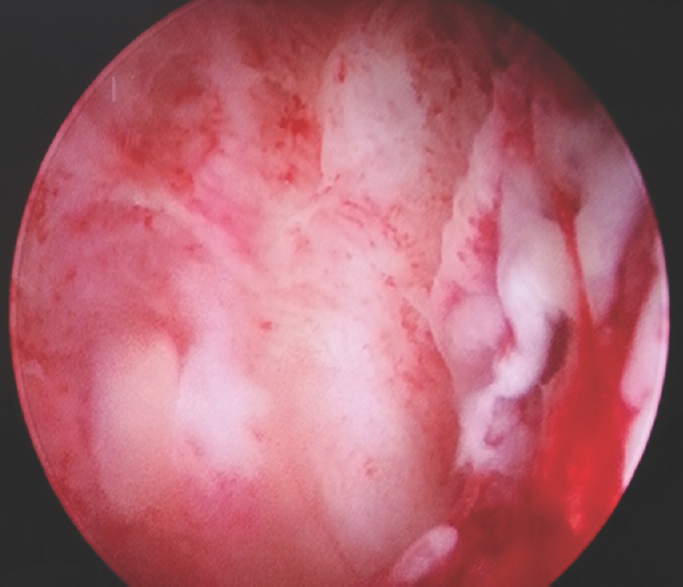
- Hysteroscopic view of endometrial hyperplasia.
Discussion
AUB is an important symptom which requires careful evaluation, more so among perimenopausal women. Although various diagnostic tools are available, there is a need for an effective non-invasive technique which can predict the endometrial pathology. Commonly used non-invasive tool to predict endometrial pathology is grey scale TVS, mainly ET. In the present study, the sensitivity and specificity of TVS in detecting endometrial hyperplasia/carcinoma were 85.7 and 33.3 per cent, respectively. Schramm et al11 evaluated the use of TVS in diagnosing endometrial carcinoma alone, and noted a sensitivity of 62 per cent and specificity of 50 per cent. In the present study, the negative predictive value of ET in predicting premalignant and malignant condition was 92.9 per cent. Similar observations were made by others1213 who showed a negative predictive value of 100 per cent. A multicentre study by Karlsson et al14 included 1168 postmenopausal women and concluded that if a cut-off of ≤4 mm was used, the negative predictive value of TVS-ET was 100 per cent. Among premenopausal women with AUB, there is no consensus on the ET cut-off. Some researchers have used a cut-off of 8 mm, while others have used a cut-off of 12 mm151617.
To overcome the shortcomings of TVS-ET alone, vessel pattern on power Doppler is studied. The vessel pattern can predict the pathology67818. Single-vessel pattern predicts endometrial polyp, scattered-vessel pattern predicts hyperplasia and multiple-vessel pattern can predict endometrial carcinoma.
In the present study, the negative predictive value of various power Doppler patterns was more than 90 per cent, implying that the presence of pathology in the absence of vascularity was less likely. The positive predictive value for detecting hyperplasia and carcinoma based on the vascularity was low because of small sample.
There were seven cases where ET was less than 4 mm but had increased vascularity. Of these seven patients, one had endometrial carcinoma and one had uterine sarcoma. If biopsy was not performed in these seven patients considering the ET as normal, two cases of malignancy would have been missed. Hence, irrespective of ET, the presence of vascularity is a significant predictive factor. If abnormal ET and power Doppler pattern were combined, the specificity of detecting hyperplasia increased to 89.6 per cent and specificity of detecting carcinoma increased to 92.6 per cent.
In the present study, the specificity, positive predictive value and negative predictive value of hysteroscopy in detecting endometrial carcinoma were 100, 100 and 97.6 per cent, respectively. These results were in accordance with various other studies. In a study by El-Morsi et al7, the specificity was 95.89 per cent, positive predictive value was 62.5 per cent and negative predictive value of 97.2 per cent. The specificity of detecting endometrial carcinoma was 87.5 per cent in a study by Tandulwadkar et al19 and 100 per cent in the study by Loverro et al20.
There was one patient whose TVS, power Doppler and hysteroscopy suggested a polyp which turned out to be an endometrial adenocarcinoma on histopathology. This is likely to alter the results as there were only five patients with endometrial carcinoma including this patient.
The strengths of our study were use of all the available methods for the assessment of endometrial pathology which led to meaningful comparisons and women with other apparent causes of AUB which were unlikely to be due to endometrial pathology were excluded. The limitations of the study were small number of women with endometrial carcinoma which led to poor sensitivity and positive predictive value of the evaluation methods. Transvaginal ultrasound, power Doppler and hysteroscopy for all the patients were not done by the same observer due to logistic reasons which could have led to inter-observer variations.
It was noticed that postmenopausal women approached the health facility earlier when compared to premenopausal women with AUB. Our results showed that for evaluation of AUB, addition of power Doppler to grey scale TVS improved the specificity and negative predictive value almost comparable to hysteroscopy. However, the sensitivity and positive predictive value did not improve probably owing to small number of endometrial hyperplasia/carcinoma (9 of 100) in the study.
Financial support & sponsorship: None.
Conflicts of Interest: None.
References
- A randomised controlled trial comparing transvaginal ultrasound, outpatient hysteroscopy and endometrial biopsy with inpatient hysteroscopy and curettage. Br J Obstet Gynaecol. 1999;106:1259-64.
- [Google Scholar]
- Evaluation of different transvaginal sonographic diagnostic parameters in women with postmenopausal bleeding. Ultrasound Obstet Gynecol. 1998;12:265-70.
- [Google Scholar]
- The accuracy of transvaginal ultrasonography in the diagnosis of endometrial abnormalities. Obstet Gynecol. 1996;87:345-9.
- [Google Scholar]
- Accuracy of color Doppler and transvaginal sonography in detecting endometrial abnormalities in women with premenopausal and postmenopausal bleeding. El Minia Med Buli. 2000;11:43-53.
- [Google Scholar]
- Endometrial blood flow mapping using transvaginal power Doppler sonography in women with postmenopausal bleeding and thickened endometrium. Ultrasound Obstet Gynecol. 2003;21:583-8.
- [Google Scholar]
- Transvaginal power Doppler sonography can discriminate between benign and malignant endometrial conditions in women with postmenopausal bleeding. Middle East Fertil Soc J. 2012;17:22-9.
- [Google Scholar]
- Three-dimensional ultrasound imaging for discrimination between benign and malignant endometrium in women with postmenopausal bleeding and sonographic endometrial thickness of at least 4.5 mm. Ultrasound Obstet Gynecol. 2010;35:94-102.
- [Google Scholar]
- New WHO classification of endometrial hyperplasias. Geburtshilfe Frauenheilkd. 2015;75:135-6.
- [Google Scholar]
- The behavior of endometrial hyperplasia. A long-term study of “untreated” hyperplasia in 170 patients. Cancer. 1985;56:403-12.
- [Google Scholar]
- Endometrial carcinoma and vaginal ultrasound: Studies of the diagnostic validity. Geburtshilfe Frauenheilkd. 1995;55:65-72.
- [Google Scholar]
- Comparative study of transvaginal sonography and hysteroscopy for the detection of pathologic endometrial lesions in women with postmenopausal bleeding. J Ultrasound Med. 1994;13:757-62.
- [Google Scholar]
- Vaginosonography for early detection of endometrial carcinoma? Lancet. 1990;335:1569-71.
- [Google Scholar]
- Transvaginal ultrasonography of the endometrium in women with postmenopausal bleeding-a nordic multicenter study. Am J Obstet Gynecol. 1995;172:1488-94.
- [Google Scholar]
- Endometrial thickness screening in premenopausal women with abnormal uterine bleeding. J Obstet Gynaecol Res. 2006;32:588-92.
- [Google Scholar]
- Sonographic depiction of the endometrium during normal cycles. Ultrasound Med Biol. 1986;12:271-7.
- [Google Scholar]
- Ultrasonography-based triage for perimenopausal patients with abnormal uterine bleeding. Am J Obstet Gynecol. 1997;177:102-8.
- [Google Scholar]
- Role of transvaginal sonography, power Doppler and hysteroscopy in women with abnormal uterine bleeding: A comparative study. IOSR J Dent Med Sci. 2014;13:82-9.
- [Google Scholar]
- Transvaginal sonography and hysteroscopy in postmenopausal uterine bleeding. Maturitas. 1999;33:139-44.
- [Google Scholar]




