
Translate this page into:
Glucose tolerance & insulin secretion & sensitivity characteristics in Indian children with cystic fibrosis: A pilot study
Reprint requests: Dr Vandana Jain, Department of Pediatrics, Division of Pediatric Endocrinology, All India Institute of Medical Sciences, New Delhi 110 029, India e-mail: drvandanajain@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Cystic fibrosis (CF) is a life-limiting genetic condition resulting in chronic respiratory infections, pancreatic enzyme insufficiency and associated complications. This pilot study was undertaken to assess the glucose tolerance and insulin secretion and sensitivity among Indian children with CF.
Methods:
Children with CF under regular follow up at the Paediatric Pulmonology Clinic of a tertiary care hospital in New Delhi, India, were enrolled. Children who had a history of acute exacerbation or intake of systemic steroids within the last two weeks were excluded. Anthropometry, pulmonary function and disease severity (Shwachman) score were assessed. Fasting venous sample was drawn to assess glucose, insulin, haemoglobin and calcium. Oral glucose tolerance test was performed, and blood glucose and insulin were assessed at 30, 60, 90 and 120 min. Insulin secretion and sensitivity indices were calculated.
Results:
Twenty nine patients with a mean age of 11.2±4.1 yr were enrolled. Stunting, thinness, anaemia and hypocalcaemia were present in 31.0, 13.8, 37.0 and 48.3 per cent of the patients, respectively. Abnormal glucose tolerance (AGT) was present in 21.4 per cent. Insulin secretion was similar in individuals with AGT and normal glucose tolerance (NGT), but insulin sensitivity index was lower (0.12±0.02 vs 0.15±0.01, P<0.001) and homeostatic model assessment of insulin resistance higher [1.63 (0.53-1.76) vs 0.83 (0.28-4.43), P<0.05] in individuals with AGT compared to NGT.
Interpretation & conclusions:
AGT was observed in 21.4 per cent of children with CF. The CF patients with AGT had significantly lower insulin sensitivity compared to patients with NGT. Future multicentric studies with a large sample should be conducted to assess insulin secretion and sensitivity indices in CF patients compared to healthy controls.
Keywords
Adolescents
cystic fibrosis related diabetes
glucose intolerance
insulin resistance
insulinopenia

Cystic fibrosis (CF), a disease of exocrine gland function that involves multiple organ systems, is a common inherited disease. Although estimated to affect one in approximately ten to forty thousand children in India, the diagnosis is made in a much smaller fraction due to the paucity of awareness and diagnostic facilities1. The major clinical manifestations of CF are chronic respiratory infections and pancreatic enzyme insufficiency. With the improvement in life expectancy, abnormal glucose homeostasis has emerged as an important co-morbidity, that is associated with worsening of nutritional and pulmonary function status, and increased mortality23.
The published literature regarding impaired glucose tolerance (IGT), CF-related diabetes (CFRD) and the underlying abnormalities in insulin secretion and sensitivity is predominantly from Caucasian population345678, with no data from the Indian subcontinent. However, the profile of CF in India differs from that in the Western countries. The diagnosis is delayed, undernutrition is common at diagnosis, colonization with pseudomonas is high, and therapy is often suboptimal, due to the constraints of cost and availability1. F508del mutation, which is associated with higher risk of CFRD7 occurs at a low frequency in Indian CF patients9. On the other hand, Asian Indian ethnicity lends an increased predisposition to insulin resistance10. All these factors could potentially affect the insulin secretion and sensitivity, and hence glucose tolerance, in Indian CF patients.
This pilot study was conducted to assess the prevalence of abnormal glucose tolerance (AGT), i.e., IGT or CFRD among Indian children with CF; and to compare the insulin secretion and sensitivity profile on oral glucose tolerance test (OGTT) among the patients with normal glucose tolerance (NGT) and AGT. The study also aimed to determine the growth, puberty, nutritional status and pulmonary function among these children, and to assess whether these parameters were different among those with NGT and AGT.
Material & Methods
This cross-sectional pilot study was conducted at Pediatric Pulmonology Clinic, department of Pediatrics, All India Institute of Medical Sciences, New Delhi, India, between January 2011 and December 2013 after approval from Institutional Ethics Committee.
All eligible and consenting individuals were enrolled during the study period in this pilot study. The CF outpatients (diagnosed on the basis of sweat chloride >60 mmol/l on 2 tests) aged 6-18 yr were enrolled. Patients who were on long-term systemic steroids and those with an acute exacerbation, hospitalization or systemic steroid intake within the last two weeks were excluded. Voluntary informed written consent was taken from parents, and assent from the children. Detailed clinical history (including age at diagnosis, respiratory and gastrointestinal symptoms, frequency of exacerbations, current medication and symptoms of diabetes) was recorded.
Clinical status: The disease severity was assessed by Shwachman and Kulczycki11 score for all individuals. Based on the score, the condition of the patient was categorized as excellent (86-100), good (71-85), average (56-70), poor (41-55) or severe (≥40)11. Exocrine pancreatic insufficiency was considered to be present if the patient was either taking enzyme supplements or had large bulky stools. Lung function [forced expiratory volume in the first second (FEV1) and forced vital capacity (FVC)] was assessed by spirometry (Micromedical, SU 6000, Rochester, UK). Results were expressed as the percentage of predicted values for age, sex, height and ethnic background.
Nutritional status: Weight was measured with an electronic weighing scale with sensitivity of 100 g, and height was measured by a stadiometer with a sensitivity of 0.1 cm. Body mass index (BMI) was calculated as weight (kg)/ height (m)2. For all patients z-scores for age and gender (standard deviation scores) were computed for height and BMI, using Indian growth charts1213. Height for age z-score <-2 was defined as stunting, and BMI for age z-score (BMIZ) <-2 was defined as thinness14. Pubertal status was assessed by Tanner staging.
Oral glucose tolerance test (OGTT) and other biochemical tests: Basal blood sample was drawn at 0800 h after a 12 h fast. This was followed by oral administration of 1.75 g/kg body weight of glucose (maximum 75 g, consumed over less than three minutes) and repeat blood sampling at 30, 60, 90 and 120 min. In the basal sample, haemoglobin, calcium, glucose and insulin were measured, and in all four samples taken after oral glucose administration, glucose and insulin were measured. Plasma glucose was measured by oxidase method and insulin by immunoradiometric assay (IRMA) (Immunotech, Beckman Coulter, France, intra-assay variation 2.3%). The measurements were done in duplicate. Insulin concentration in μU/ml was converted to pmol/l by multiplying by six15. The American Diabetes Association cut-offs for fasting and two hours plasma glucose values were used16.
Indices of insulin secretion: (i) First phase insulin secretion (F1OGTT)=1283+(1.829×Ins30)−(138.7 × Glu30)+(3.772×Ins0) pmol; (ii) Percentage beta cell function (% β)=(Ins0×3.33)/(Glu0-3.5); and (iii) Integrated insulin secretion (IIS)=Area under the curve for insulin after OGTT pmol/l/h.
Indices of insulin sensitivity: (i) Insulin sensitivity index on OGTT (ISI)=0.226-0.0032×BMI-0.0000645×Ins120−0.00375×Glu90 C umol/kg/min/pmol; and (ii) Homeostatic model assessment of insulin resistance (HOMA-IR)=Ins0×Glu0/135. Ins=insulin concentration in pmol/l, Glu=glucose concentration (mmol/l), and the number suffixed indicates the time of measurement during the OGTT.
F1OGTT is derived from the values of glucose and insulin at 0 and 30 min. It represents the release of preformed insulin in response to a glucose load. The decline in F1OGTT is an early marker of reduced beta cell function. The other two indices of insulin secretion are percentage beta and IIS. Percentage beta cell function is based on fasting insulin and glucose levels, while IIS is based on all five values of insulin during the OGTT. For insulin sensitivity, the standard indices, HOMA-IR and ISI were used. These indices have been previously validated against the gold standard methods for estimating insulin secretion and sensitivity i.e. hyperglycaemic euglycaemic clamp1718, as well as the intravenous glucose tolerance test in patients with CF19 and used by other investigators3456720.
Statistical analysis: Descriptive statistics were calculated pertinent to the nature of the studied variables using SPSS statistical package, version 4.1 (SPSS, Chicago, IL, USA). Comparison of the quantitative variables between the NGT and AGT groups was done by t test or Wilcoxon rank sum test. Area under the curve for insulin was calculated. Spearman rank correlation was calculated to study the strength of association of the various parameters.
Results
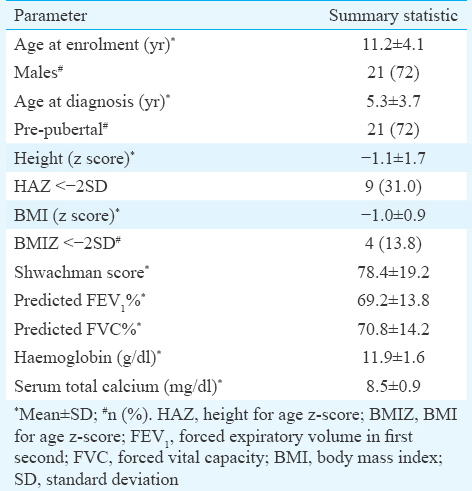
The study was conducted in 29 children with CF (21 boys and 8 girls) with a mean age 11.2±4.1 yr. None of the patients had previously been investigated for CFRD or IGT. The clinical profile of these individuals is provided in Table I. The age at diagnosis of CF was 5.3±3.7 yr. Exocrine pancreatic insufficiency was present in all. Stunting and thinness were seen in 31 and 13.8 per cent patients, respectively (Table I). Puberty was delayed in five of the ten individuals older than 13 yr. Anaemia was present in 10 (37.0%) patients, using age-appropriate WHO cut-offs for haemoglobin. Hypocalcaemia (total serum calcium <8.5 mg/dl) was present in 14 (48.3%) patients. BMIZ showed a positive correlation with percentage of predicted FEV1 and FVC (r=0.39, P<0.05; and r=0.41, P<0.05, respectively) and height z-score was positively correlated with Shwachman score (r=0.42, P<0.05).
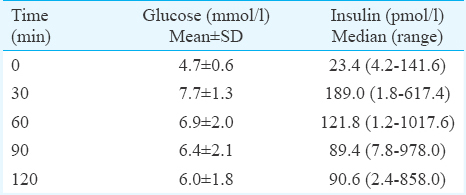
The summary statistics for glucose and insulin during OGTT are presented in Table II. None of the patients had fasting hyperglycaemia or impaired fasting glucose. At 120 min after glucose load, plasma glucose level was >11.1 mmol/l (CFRD) in one patient, and between 7.8 and 11.1 mmol/l (IGT) in five. Thus, AGT (CFRD or IGT) was present in 21.4 per cent (95% CI 8.0-40.0%) patients. On comparison of age, gender, age at diagnosis, pubertal status, pulmonary function, nutritional parameters and Shwachman-Kulczycki score between the individuals with NGT (n=23) and AGT (n=6), no significant differences were found (Table III). The patient diagnosed with CFRD was an 18 yr old boy, with height z-score of -2.7, BMI z-score of -1.3 and delayed puberty.
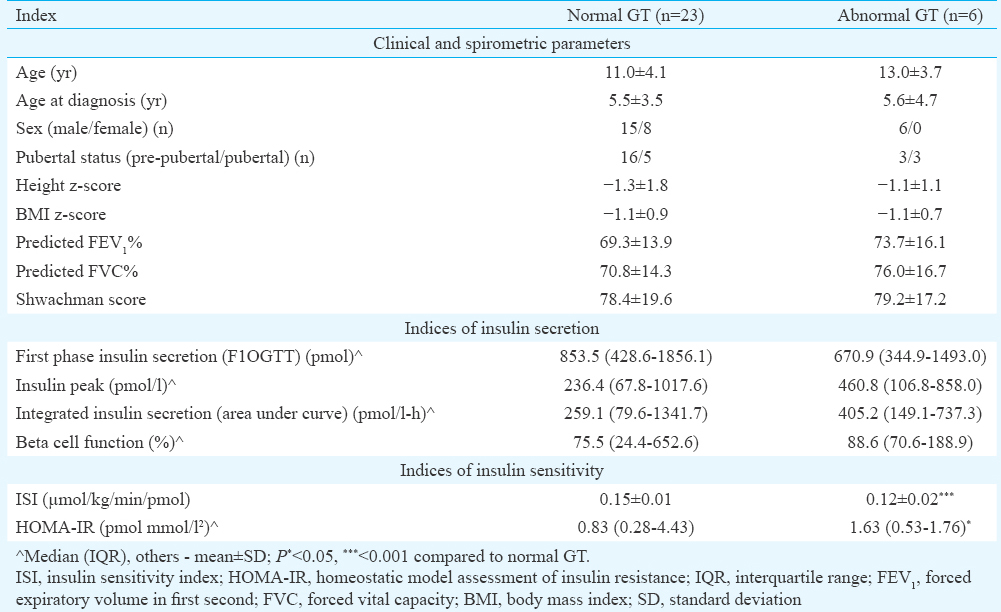
The comparison of indices of insulin secretion and sensitivity between the individuals with NGT and AGT is presented in Table III. No significant difference was observed in the indices of insulin secretion. However, insulin sensitivity index was lower and HOMA-IR higher in the group with AGT. A positive correlation of first phase insulin secretion with BMI (r=0. 41, P<0.05) was observed. A direct correlation was also observed between fasting insulin levels and FVC (r=0.36, P=0.07), although not significant.
Discussion
In the present study conducted in relatively young patients (mean age 11.2±4.1 yr, 72% pre-pubertal), CF was found in one and IGT in five patients. None of the patients had fasting hyperglycaemia or impaired fasting glucose, indicating that fasting blood glucose alone has poor sensitivity as a screening tool for AGT in CF patients.
On comparison of insulin secretion and sensitivity parameters on OGTT between the CF patients with NGT and AGT, insulin secretion was similar among the two groups, but insulin sensitivity was significantly lower among the AGT group. This suggests that insulin resistance may be the predominant mechanism for AGT in our patients. However, this finding will need to be confirmed in an adequately powered study.
Previous studies, mostly from Caucasian CF patients, have reported that insulin secretion is decreased and delayed in CF patients with AGT compared to those with NGT6721. Insulin resistance has not been observed to play a significant role in the pathogenesis of AGT among CF patients by several investigators367, while others521 have noted that insulin secretion is diminished in all CF patients in comparison to controls, and additional development of insulin resistance tilts the balance towards AGT.
Due to ethical considerations, insulin secretion and sensitivity could not be measured in age matched healthy children as controls. Therefore, it could not be assessed whether CF patients as a group had insulinopenia in comparison to age-matched healthy children. This was a limitation of our study. However, area under the insulin curve and beta cell function were noted to be higher in the AGT group as compared to NGT group. This indicated that CF patients with AGT were secreting greater amount of insulin but still had hyperglycaemia in response to oral glucose load due to their impaired insulin sensitivity.
The median beta cell function in our CF patients with NGT and AGT was 75.5 and 88.6 per cent, respectively, compared to mean values of 35.1 and 24.9 per cent among the patients with NGT and IGT in a study in Spanish CF patients20 (n=50, age 20.7±7.0 yr). Similarly, the median insulin peaks of 236.4 and 460.8 pmol/l, respectively, in our CF patients with NGT and AGT were much higher in comparison to the mean insulin peaks of 58.6 and 48.9 pmol/l, respectively, reported in the same study20. The median first phase insulin secretion in our patients with NGT and IGT of 853.5 and 670.9 pmol was also higher than the corresponding mean values of 450±291 and 309±254 reported by Anzeneder et al4 among adult CF patients (n=34) and was closer to the value of 950±388 reported among the healthy adult controls in the study4. Thus, in our patients, impaired insulin sensitivity rather than absolute insulinopenia was probably the more important factor in the development of AGT.
Previous studies have suggested that CF patients with AGT have poorer nutritional, clinical and pulmonary function status as compared to those with NGT20222324. However, we did not find a significant difference in any of these parameters between the children with NGT or AGT. This could be due to the absence of significant insulinopenia in our patients with AGT. Also, fasting serum insulin was directly correlated with FVC and indices of insulin secretion were correlated with BMI, suggesting that insulinopenia might have a causative role in the decline in nutritional status and pulmonary function.
The prevalence of thinness, stunting and pubertal delay in our patients was similar to that reported in CF patients from other countries252627. Positive correlation between BMI z-score and pulmonary function test, and between height z-score and Shwachman score, as noted in our study has been reported in previous studies as well2526. Anaemia and hypocalcaemia were also noted in a sizeable number of our patients. These are probably related to deficiency of iron and vitamin D, respectively and may reflect suboptimal pancreatic enzyme supplementation, and chronic inflammation2829.
In conclusion, AGT was present in more than a fifth of our patients, and insulin resistance rather than insulinopenia appeared to play a dominant role in its development. A larger, preferably multicentric study to evaluate the insulin secretion and sensitivity indices in Indian patients with CF, in comparison to healthy controls should be conducted. Future studies should also assess the aetiology of insulin resistance, including levels of markers of inflammation; and the best therapeutic modalities for the management of AGT and CFRD in Indian CF patients, which may be different from those recommended in Western literature.
Acknowledgment
The study was funded by an intramural research grant to VJ from All India Institute of Medical Sciences, New Delhi.
Conflicts of Interest: None.
References
- Clinical importance of cystic fibrosis-related diabetes. J Cyst Fibros. 2004;3:209-22.
- [Google Scholar]
- Glucose tolerance and insulin secretion, morbidity, and death in patients with cystic fibrosis. J Pediatr. 2008;152:540-5. 545.e1
- [Google Scholar]
- Kinetics of insulin secretion and glucose intolerance in adult patients with cystic fibrosis. Horm Metab Res. 2011;43:355-60.
- [Google Scholar]
- Glucose tolerance, insulin secretion, and insulin sensitivity in children and adolescents with cystic fibrosis and no prior history of diabetes. J Pediatr. 2007;151:653-8.
- [Google Scholar]
- Glucose homeostasis and genotype-phenotype interplay in cystic fibrosis patients with CFTR gene deltaF508 mutation. Diabetes Care. 2007;30:1187-92.
- [Google Scholar]
- Cystic fibrosis-related diabetes: The role of peripheral insulin resistance and beta-cell dysfunction. Diabet Med. 2002;19:221-6.
- [Google Scholar]
- Characterisation of mutations and genotype-phenotype correlation in cystic fibrosis: Experience from India. J Cyst Fibros. 2008;7:110-5.
- [Google Scholar]
- Obesity-related non-communicable diseases: South Asians vs. White Caucasians. Int J Obes (Lond). 2011;35:167-87.
- [Google Scholar]
- Long-term study of one hundred five patients with cystic fibrosis; studies made over a five- to fourteen-year period. AMA J Dis Child. 1958;96:6-15.
- [Google Scholar]
- Physical and sexual growth pattern of affluent Indian children from 5 to 18 years of age. Indian Pediatr. 1992;29:1203-82.
- [Google Scholar]
- Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007;85:660-7.
- [Google Scholar]
- Insulin assay standardization: Leading to measures of insulin sensitivity and secretion for practical clinical care: Response to Staten et al. Diabetes Care. 2010;33:e83.
- [Google Scholar]
- Validation of surrogate estimates of insulin sensitivity and insulin secretion in children and adolescents. J Pediatr. 2004;144:47-55.
- [Google Scholar]
- Comparative evaluation of simple insulin sensitivity methods based on the oral glucose tolerance test. Diabetologia. 2005;48:748-51.
- [Google Scholar]
- Validation of insulin secretion indices in cystic fibrosis patients. J Cyst Fibros. 2009;8:378-81.
- [Google Scholar]
- Insulin-secretion abnormalities and clinical deterioration related to impaired glucose tolerance in cystic fibrosis. Eur J Endocrinol. 2005;152:241-7.
- [Google Scholar]
- Early detection of impaired glucose tolerance in patients with cystic fibrosis and predisposition factors. J Pediatr Endocrinol Metab. 2001;14:53-60.
- [Google Scholar]
- Increased glucose excursion in cystic fibrosis and its association with a worse clinical status. J Cyst Fibros. 2007;6:376-83.
- [Google Scholar]
- Abnormal glucose tolerance in prepubertal patients with cystic fibrosis. An Pediatr (Barc). 2012;77:339-43.
- [Google Scholar]
- Glucose intolerance in patients with cystic fibrosis: Sex-based differences in clinical score, pulmonary function, radiograph score, and 6-minute walk test. Respir Care. 2011;56:290-7.
- [Google Scholar]
- Prevalence of malnutrition and obesity among cystic fibrosis patients. Pediatr Int. 2014;56:89-94.
- [Google Scholar]
- Growth and pulmonary function in Chilean children and adolescents with cystic fibrosis. Rev Med Chil. 2011;139:977-84.
- [Google Scholar]
- Pubertal growth and development in cystic fibrosis: A retrospective review. Acta Paediatr. 2003;92:1029-32.
- [Google Scholar]
- Iron deficiency occurs frequently in children with cystic fibrosis. Pediatr Pulmonol. 2014;49:458-62.
- [Google Scholar]
- Vitamin D status in children with cystic fibrosis.Associations with inflammation and bacterial colonization. Ann Am Thorac Soc. 2014;11:205-10.
- [Google Scholar]




