
Translate this page into:
Comparative antinociceptive effect of arachidonylcyclopropylamide, a cannabinoid 1 receptor agonist & lignocaine, a local anaesthetic agent, following direct intrawound administration in rats
Reprint requests: Dr Subrata Basu Ray, Department of Anatomy, All India Institute of Medical Sciences, New Delhi 110 029, India e-mail: raysb48@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Treatment of inflammatory pain with opioids is accompanied by unpleasant and, at times, life-threatening side effects. Cannabis produces antinociception as well as psychotropic effects. It was hypothesized that peripheral cannabinoid receptors outside the central nervous system could be selectively activated for relief of pain. This study was undertaken to measure the antinociceptive effect of type 1 cannabinoid receptor (CB1r) agonist arachidonylcyclopropylamide (ACPA) in a rat model of inflammatory pain after intrawound administration and the effects were compared with lignocaine.
Methods:
Wounds were produced under controlled conditions by an incision in the right hind paw in rats. ACPA (10, 30 or 100 μg/10 μl) was administered directly into the wound. Antinociception was evaluated by guarding, allodynia and thermal hyperalgesia. This was compared to lignocaine (30 μg/10 μl). Reversal of ACPA (30 μg)-mediated antinociceptive effect was attempted by intrawound AM251 (100 μg), a CB1r antagonist. Antinociception was also evaluated after contralateral administration of ACPA (30 μg). Primary afferent nociceptive input to the spinal cord was investigated by c-Fos expression after ACPA treatment (100 μg).
Results:
ACPA, but not lignocaine, inhibited guarding behaviour, which was locally mediated. Conversely, lignocaine, but not ACPA, inhibited thermal hyperalgesia and mechanical allodynia. ACPA-mediated inhibitory effect was reversible and dose dependent. It was associated with a decreased c-Fos expression. Locomotor activity was unaffected following ACPA (100 μg) treatment.
Interpretation & conclusions:
Lignocaine attenuated evoked pain behaviour whereas ACPA decreased guarding score. This difference was likely due to blockade of sodium ion channels and the activation of peripheral CB1r, respectively. Central side effects were absent after ACPA treatment. Further studies need to be done to assess the effect of ACPA treatment in clinical conditions.
Keywords
Allodynia
antinociception
arachidonylcyclopropylamide
cannabinoid receptor
hyperalgesia
lignocaine
pain
plantar incision
post-operative pain

Opioids are the mainstay in the treatment of moderate-to-severe inflammatory pain although their use is associated with several side effects such as nausea and vomiting, tolerance, dependence, constipation, urinary retention, excessive sedation and at times life-threatening respiratory depression1. Cannabis and its derivatives, such as marijuana, obtained from Cannabis sativa, have been used for medical purpose2. Besides antinociceptive effect, Cannabis also produces remarkable psychotropic effects such as euphoria and relaxation, drowsiness, increased appetite, impairment of memory and decreased motor coordination3. However, tolerance and dependence are generally mild, and instances of respiratory depression are relatively rare except at very high doses.
The pharmacological effect of cannabinoids is mediated by naturally occurring cannabinoid receptors, which are classified into type 1 (CB1r) and 2 (CB2r)4. In the mammalian nervous system, CB1rs are expressed in several sites such as the hippocampus, caudate-putamen, cerebral cortex and dorsal horn of the spinal cord5. These are also expressed in the dorsal root ganglion neurons6 and human peripheral nerve fibres7. In contrast, CB2rs are predominantly noted in immune cells such as splenic macrophages, lymphocytes and microglia5. Activation of peripherally expressed CB1rs resulted in antinociceptive effect in the inflammatory and the neuropathic rodent pain models89. CB2r-mediated antinociception has been reported in pain arising from bone tumour, monosodium iodoacetate-induced arthritis, neuropathy and inflammation10111213. Synthetic cannabinoid derivatives such as nabilone and dronabinol are often used in humans as antiemetics3. Recently, evidence has been presented regarding the use of marijuana for medical treatment of chronic pain14.
Considering the necessity of avoiding undesirable central nervous system-mediated psychotropic effects of cannabinoids, it has been hypothesized that peripherally expressed cannabinoid receptors can be selectively activated for relief of pain15. The antinociceptive effect of a peripherally acting, synthetic CB1r agonist (chromenopyrazole 13 a) has been demonstrated in a rat model of orofacial pain. In another study, inhibition of the enzyme responsible for metabolic breakdown of anandamide in the peripheral tissue resulted in antinociception in rats with inflammatory and neuropathic pain16. Anandamide (N-arachidonoyl ethanolamide) is an endogenously synthesized cannabinoid first identified in 199017. In addition, direct intraplantar injection of anandamide (0.01 ng) attenuated carrageenan-mediated hyperalgesia and oedema in rats18. Knockout of CB1r gene produced hypersensitivity to pain under basal conditions8. These reports indicate that peripheral cannabinoid receptors can not only modulate pain during inflammation but also affect baseline pain sensitivity. However, the role of cannabinoids in attenuating nociception after direct intrawound administration has not been studied. Thus, the objective of the study was to evaluate the antinociceptive effect of the CB1r agonist arachidonylcyclopropylamide (ACPA) following intrawound administration in a rat model of inflammatory pain and to compare its effect with lignocaine.
Material & Methods
The study was done in the department of Anatomy, All India Institute of Medical Sciences, New Delhi, India, between March, 2013 and July, 2014. Male Sprague-Dawley rats (weight: 240-270 g) were randomly allocated to specific experimental groups. Each experimental group had six animals. For this, each of the animals belonging to the batch of three rats, studied at a particular time, were ascribed to different treatment groups such as control, ACPA or lignocaine. Each rat had an equal chance of being ascribed to a specific group. Also, wherever possible, care was taken to select rats from different litter groups. Following incision, rats were kept individually in single cages with clean, soft bedding (Alpha-dri®, Shepherd Speciality Papers, Milford, NJ, USA). The study protocol was approved by the Institutional Animal Ethics Committee.
ACPA, a potent and selective CB1r agonist was purchased as a water-soluble emulsion in Tocrisolve (Tocris Bioscience, UK). It was further diluted in Tocrisolve (soya oil/water mixture emulsified with co-polymer Pluronic F68) to the desired concentration of 10, 30 and 100 μg/10 μl. These doses of ACPA were selected based on preliminary studies on a wide range of doses. AM251 (Tocris Bioscience, UK) is a CB1r antagonist, which was dissolved in 25 per cent dimethylsulphoxide (in normal saline) using sonication. Lignocaine hydrochloride I.P. (Xylocaine® 2%, AstraZeneca, India) was diluted in saline to desired concentration (30 μg/10 μl). Intrawound administration of drugs (ACPA or AM251 or lignocaine) was performed only once in each rat, using an earlier described procedure from our laboratory19. Nociception was evaluated at regular intervals up to day seven.
Hind paw incision and drug administration: Tissue injury involving skin, fascia and muscle was produced by an earlier procedure20. In brief, a 1 cm long longitudinal midline incision was made along the hind paw starting 0.5 cm from the heel under isoflurane anaesthesia. The underlying flexor digitorum brevis muscle was lifted up and a 0.5 cm long incision was made along its longitudinal axis without damaging the origin or insertion. The muscle was replaced back and the blood/tissue fluid within the incision site was swabbed repeatedly so as to make the wound dry. The drug was administered into the wound after lifting the edges of the incised skin by forceps so as to create a pocket. ACPA dissolved in Tocrisolve to a total volume of 10 μl was directly administered into the wound by a sterile micropipette. After an interval of 30 sec, the incision site was sutured by two mattress sutures (4-0, Ethicon®, USA). The knots were placed on the lateral side. Finally, the rats were transferred to a warm recovery chamber. In the control group, Tocrisolve solution alone was administered into the wound (10 μl). The antinociceptive effect of lignocaine (30 μg/10 μl), a local anaesthetic agent, was also studied.
Behavioural tests for nociception: Nociception was determined by sequential evaluation of guarding behaviour (non-evoked), mechanical allodynia and thermal hyperalgesia (evoked nociception) at two and eight hours after incision and then at the end of every 24 h19. The time intervals corresponded with the beginning of the behavioural tests. Baseline values were obtained one day before the incision. Guarding was represented as cumulative pain score. Thermal hyperalgesia and mechanical allodynia were evaluated up to day seven and expressed as percentage maximum possible effect (%MPE) and 50 per cent withdrawal threshold (g), respectively.
The procedure for the estimation of guarding behaviour was as previously reported2021. Rats were placed over a metal wire mesh platform, and the position of the hind paws was observed from below the wire mesh. This was done for the first one minute period for every five minutes for one hour. A specific score was awarded depending on the position of the paw. The score was two when the incised area was lifted up; one when the paw rested lightly on the mesh and zero if there was full weightbearing on the incised site. Full weightbearing was verified by blanching or distorting the skin. The other paw was also observed at the same time and correspondingly marked. The 12 scores for each paw were added. Finally, the total score of the incised paw was subtracted from that of the non-incised paw to derive the cumulative pain score.
For mechanical allodynia, the rats were allowed to remain over the wire mesh. Allodynia was determined in the peri-incisional area (medial to the incision and near the heel) using the up-down method22. Calibrated von Frey filaments of different sizes (3.61, 3.84, 4.08, 4.31, 4.56, 4.74, 4.93 and 5.18) were applied to the paw in perpendicular manner from below the mesh (North Coast Medical Inc., San Jose, CA, USA). The filament was pressed to the paw until it buckled, and the pressure was maintained for 7-8 sec. The first filament was of size 4.31. If withdrawal occurred, the next lighter filament was applied. If withdrawal was absent, the next heavier filament was applied. An interval of two minutes was maintained between the applications. Testing was continued until four filaments were applied after the first one that produced withdrawal response. The value was expressed as 50 per cent withdrawal threshold (g). If withdrawal was absent in sequential manner up to the heaviest filament, 15 g was recorded. If withdrawal occurred sequentially up to the lightest filament, 0.4 g was recorded. Greater withdrawal threshold values indicate less pain.
Thermal hyperalgesia was determined by the plantar test apparatus (UGO Basile, Italy)18. Rats were kept on a specially designed glass platform. After acclimatization for 15 min, an infrared heat source was directed at the site of incision from below the glass platform. Withdrawal of the paw was detected by a motion sensor, which cuts off the heat source. The latency of paw withdrawal was recorded in seconds (sec). Three consecutive readings were obtained at intervals of two minutes, and the average latency period was calculated. Baseline latency values were between 8 and 10 sec. Cut-off latency time was maintained at 20 sec. The %MPE was calculated as follows: [(drug-induced latency − baseline latency]/[cut-off latency − baseline latency)] × 100. The negative sign for the final value was ignored.
Reversibility of ACPA-induced antinociception: To investigate whether the antinociceptive effect of ACPA was indeed mediated by CB1r, a CB1r antagonist, AM251 (100 μg) was administered before ACPA (30 μg) in 10 μl volume and allowed to remain in the wound for 60 sec. At the end of this period, the remaining solution was aspirated out before the administration of ACPA (30 μg) for 30 sec. Finally, the wound was sutured. In another group of rats, only AM251 was administered and the drug was allowed to remain in the wound for 60 sec. For both these groups, behavioural assessment of nociception was done until day one.
Site of action: To evaluate whether the antinociceptive effect of ACPA was peripherally (locally) mediated following intrawound administration, the behavioural tests for pain were done after administration of ACPA (30 μg/10 μl subcutaneous injection) in the contralateral paw. Vehicle was not added on the ipsilateral side.
c-Fos immunostaining: For c-Fos immunostaining of the spinal cord23, experimental animals (n=12) were divided into two equal groups – vehicle-treated rats and rats treated with ACPA (100 μg). One hour after incision, rats were anaesthetized with pentobarbital (100 mg/kg i.p.) and perfused first with 0.1M phosphate-buffered saline (PBS) through intracardiac route followed by four per cent paraformaldehyde. After laminectomy, part of the lumbar spinal cord corresponding to the lumbar 4-5 segments was dissected out. The primary afferent nerve fibres carrying nociceptive sensation from the incision site end at this site. Following cryopreservation, the tissue was transversely sectioned (20 μm thick at -24°C) in a cryostat (Leica CM 1950, Germany). The sections were collected by free-floating method23 in PBS. c-Fos staining was done by incubating sections in rabbit polyclonal anti-c-Fos antibody (1:250; Abcam, UK). These sections were exposed to biotin-conjugated IgG secondary antibody followed by avidin-biotin complex (Vectastain Elite ABC Kit, Vector Laboratories, Burlingame, USA). Antigen-antibody complex was visualized by 0.25 per cent 3,3’-diaminobenzidine tetrahydrochloride. Finally, sections were transferred to gelatine-coated slides and mounted in DPX (Sigma-Aldrich, USA). Photomicrographs of four sections per animal were obtained using ProgRes image analysis software (Jenoptik, Germany). Image J software (NIH, USA) was utilized to count the number of nuclei stained for c-Fos in the superficial laminae (I-II). The total area of the superficial laminae, using the same user-defined boundary, was also calculated using the software. The value of the calculated area was divided by 104 to obtain a smaller numerical value. Finally, the total number of neurons per unit area, for each tissue section, was calculated.
Healing of wound: The incision site was removed in a block (skin, fascia and muscle) on day eight in vehicle-treated and ACPA (100 μg)-treated groups after inducing deep anaesthesia (100 mg/kg pentobarbital) followed by intracardiac four per cent paraformaldehyde perfusion as described previously. Tissue sections of the paw tissue were obtained in a cryostat and stained with haematoxylin and eosin. Sections were viewed under the microscope and images were captured. Comparative evaluation of healing was done by two different observers blind to the drug treatment.
Motor activity: Horizontal locomotor activity was determined in control and ACPA (30/100 μg)-treated rats at two hours after plantar incision (Metabolic Cage, UGO Basile, Italy)24. This was compared to naïve rats. The activity monitor consisted of two facing infrared arrays of emitter and receiver sensors which recorded the number of beam-breaks for a one hour period. Since the rats became rapidly habituated to the chamber, separate groups of rats (n=6 for each group) were used at each of the time points.
Statistical analysis: The data were analyzed by GraphPad Prism software (version 5, GraphPad Software Inc., La Jolla, California, USA). One-way analysis of variance (ANOVA) followed by Bonferroni multiple comparison test was used to analyze the data of cumulative pain scores and thermal hyperalgesia and also the corresponding values of area under curve (ΔAUC). Two-way ANOVA was used to evaluate data of mechanical allodynia at each time point, assuming non-parametric distribution. ΔAUC for allodynia was evaluated by Kruskal–Wallis test followed by Dunn's multiple range test. Data for reversibility study were tested by repeated measures two-way ANOVA followed by Bonferroni test. Values of locomotor activity were analyzed using one-way ANOVA followed by Bonferroni test. Counts of c-Fos-positive cells were compared by unpaired Student's t test.
Results
Antinociceptive effect of ACPA: Behavioural parameters (guarding represented as cumulative pain score, thermal hyperalgesia as %MPE and allodynia as 50 % withdrawal threshold) showed maximum nociception, immediately after incision (at 2 h) (Fig. 1 A-C). This corresponded to comparatively higher numerical values of cumulative pain score and %MPE and lower values of 50 per cent withdrawal threshold. Subsequently, values of cumulative pain score and %MPE decreased, but that of allodynia increased with time, across the observation period. However, none of these behavioural parameters reached basal levels by the end of the observation period. ΔAUC represents the overall antinociceptive effect of a particular drug or dose of a drug over the entire observation period.
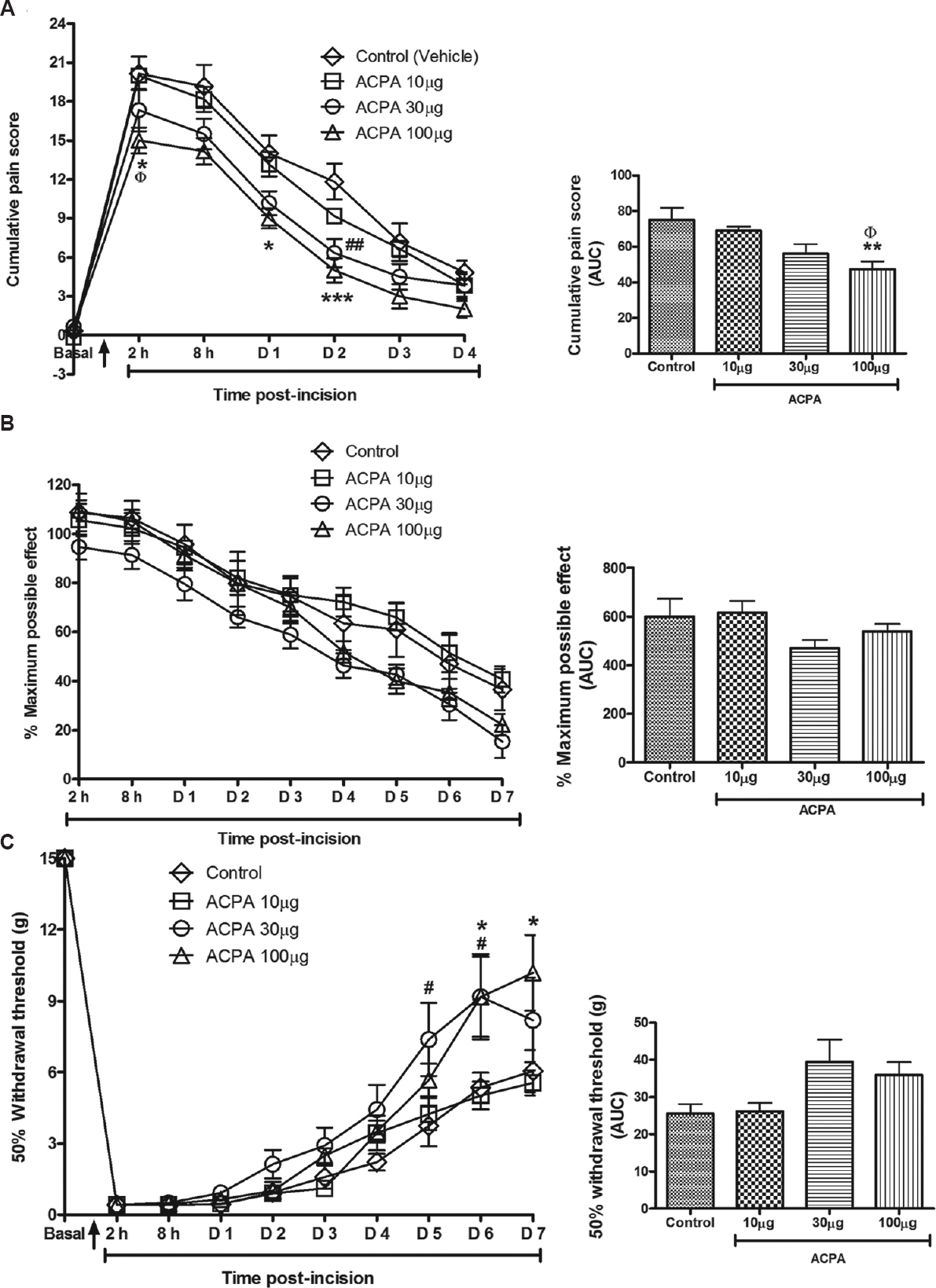
- Effect of arachidonylcyclopropylamide (ACPA) on incision-induced nociception in rats. Nociception was determined by (A) guarding, represented by cumulative pain score (B) thermal hyperalgesia by percentage maximum possible effect (% MPE) and (C) allodynia by 50 per cent withdrawal threshold (g). Overall antinociceptive effect represented by Δ area under curve. ACPA dose dependently inhibited guarding score but not thermal hyperalgesia whereas allodynia was affected relatively late. n=6 rats in each group. Values are mean±SEM. Arrow on the X-axis indicates the time of incision. P*<0.05 **<0.01 ***<0.001 ACPA (100μg) compared to control; ΦP <0.05 ACPA (100 μg) compared to ACPA (10 μg); P#<0.05 ##< 0.01 ACPA (30μg) compared to control.
Intrawound ACPA treatment resulted in a dose-dependent attenuation of cumulative pain score (10 < 30 < 100) compared to the control group (Fig. 1A). The 30 μg dose showed a significant decrease compared to the control group on day two. The 100 μg-treated group showed decrease compared to the control group at two hours and on days one and two. In addition, this group showed lower pain score compared to 10 μg at 2 h. Comparison of ΔAUC revealed that the 100 μg dose showed a significant decrease compared to the control group (P<0.01) and also to the ACPA 10 μg (P<0.05)-treated groups. Thermal hyperalgesia was not significantly affected (Fig. 1B). Interestingly, the 30 μg dose resulted in greater antinociceptive effect than the other doses. Treatment with 30 and 100 μg ACPA significantly decreased allodynia compared to the control group on days 5-6 and days 6-7, respectively (Fig. 1C). Again, comparison of ΔAUC showed that the 30 μg dose produced relatively greater antinociception.
Reversal of ACPA-mediated antinociceptive effect by AM251: The inhibition of cumulative pain score by ACPA alone was significantly reversed at eight hours and on day one by prior administration of CB1r antagonist AM251 (Fig. 2A). Administration of only AM251 further reversed the inhibition of guarding behaviour compared to AM251 + ACPA-treated group, on day one. In addition, on day one, this was significantly different than the control group. AM251 alone significantly reversed thermal hyperalgesia compared to the ACPA + AM251-treated group from two hours to day one and also to ACPA-treated group on day one (Fig. 2B). Allodynia was not significantly affected (Fig. 2C). DMSO (25%; vehicle for AM251) did not result in an antinociceptive effect (data not shown).
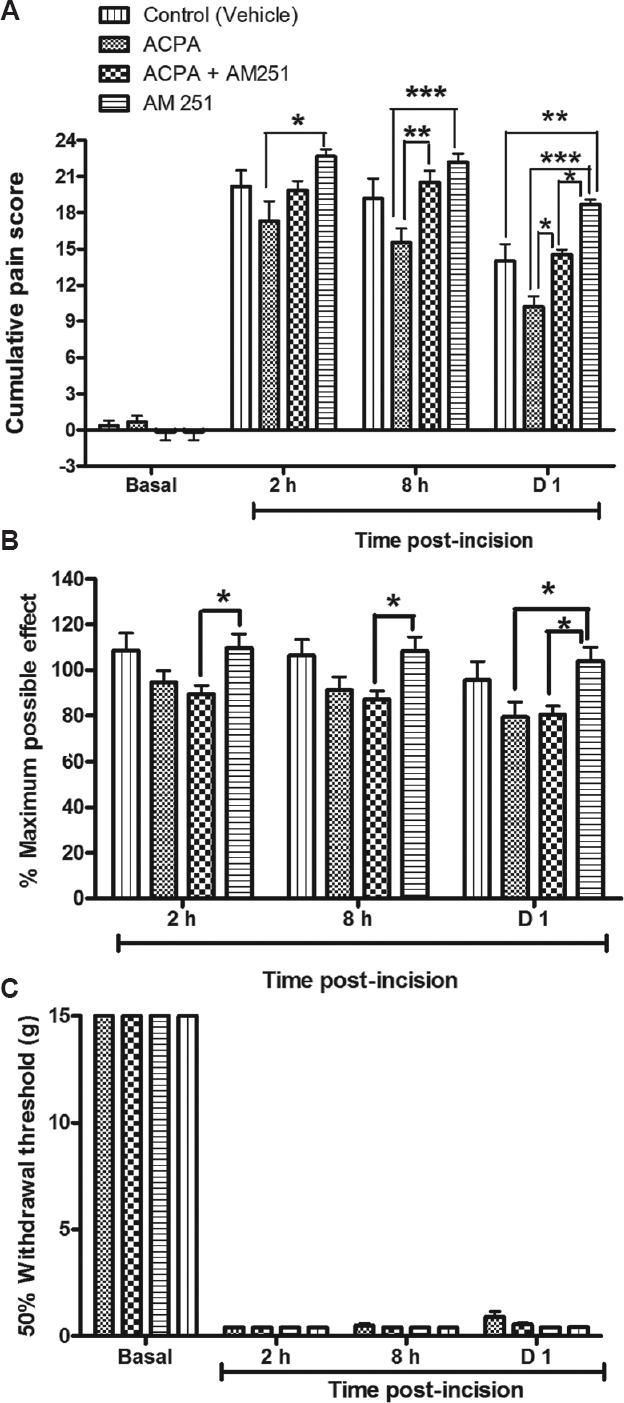
- Effect of AM251, a cannabinoid type 1 receptor antagonist, on arachidonylcyclopropylamide (ACPA)-mediated antinociception. AM251 significantly reversed ACPA-induced antinociceptive effect on (A) guarding score (eight hours and day one) but not thermal hyperalgesia or mechanical allodynia (B and C). AM251 treatment alone further reversed guarding compared to ACPA-treated group (two hours and day one) and AM251 + ACPA-treated group (day one). Also, AM251 reversed thermal hyperalgesia (two hours to day one) compared to AM251 + ACPA (two hours and day one) and to ACPA-treated group (day one). n=6 rats in each group. Values are mean±SEM. P*<0.05 **<0.01 ***<0.001.
Absence of antinociceptive effect after contralateral administration of ACPA: Contralateral administration of ACPA (30 μg s.c.) did not show an antinociceptive effect (Fig. 3A-C). For example, guarding was significantly higher at all the time intervals (P<0.001). Thermal hyperalgesia and allodynia were not affected.
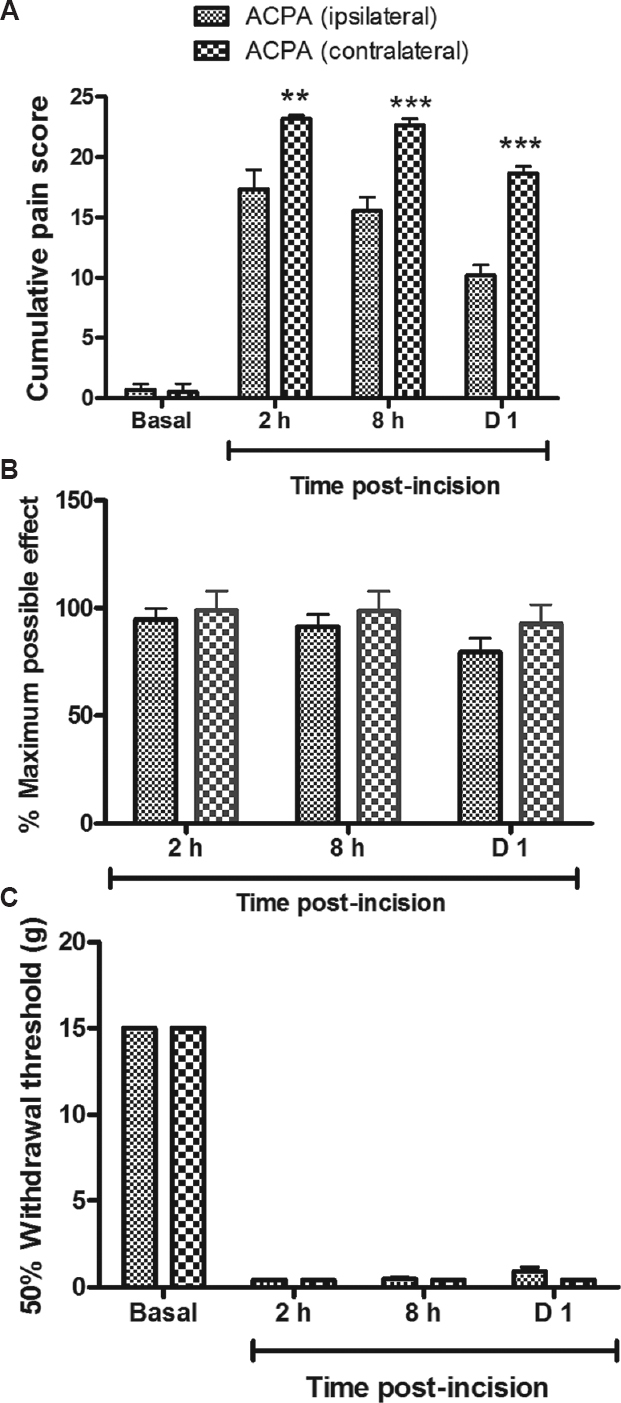
- Evaluation of the site of antinociceptive effect of arachidonylcyclopropylamide (ACPA). Comparison of antinociceptive effect of ACPA (30 μg) following ipsilateral versus contralateral administration. (A) Guarding score was significantly decreased after ipsilateral but not after contralateral administration (two hours to day one). (B) Thermal hyperalgesia and (C) mechanical allodynia were not significantly affected. n=6 in each group. Values are mean±SEM. P**<0.01 ***<0.001 compared to ACPA ipsilateral.
Comparison of antinociceptive effect of ACPA and lignocaine: Antinociceptive effect of ACPA and lignocaine (30 μg each) was compared (Fig. 4). ACPA treatment decreased cumulative pain score compared to control and the lignocaine-treated group across all time points. Significant decrease from lignocaine group was noted at eight hours (P<0.01). Significant decrease was also noted on day two in comparison to the control group (P<0.05). Comparison of ΔAUC showed that ACPA treatment resulted in lower pain scores than the other groups but these were not significantly different (Fig. 4A). On comparative analysis of ΔAUC for thermal hyperalgesia, lignocaine treatment produced significant reduction of nociception than the control group (P<0.01). This was also lower than ACPA-treated group though the values were not significantly different (Fig. 4B). Comparison of the time course of the antinociceptive effect showed that lignocaine treatment resulted in significant decrease (day 1, days 3-7) with reference to the control group and to ACPA-treated group (day 3). Values of 50 per cent withdrawal threshold (g) for the lignocaine-treated group were higher than the control group (days 3-7), indicating lower nociception (Fig. 4C). For ACPA-treated group, significantly higher values were observed on days 5-6 in comparison to the control group. ΔAUC analysis demonstrated significantly different value for lignocaine-treated group compared to the control group (P<0.05), again indicating lower nociception.
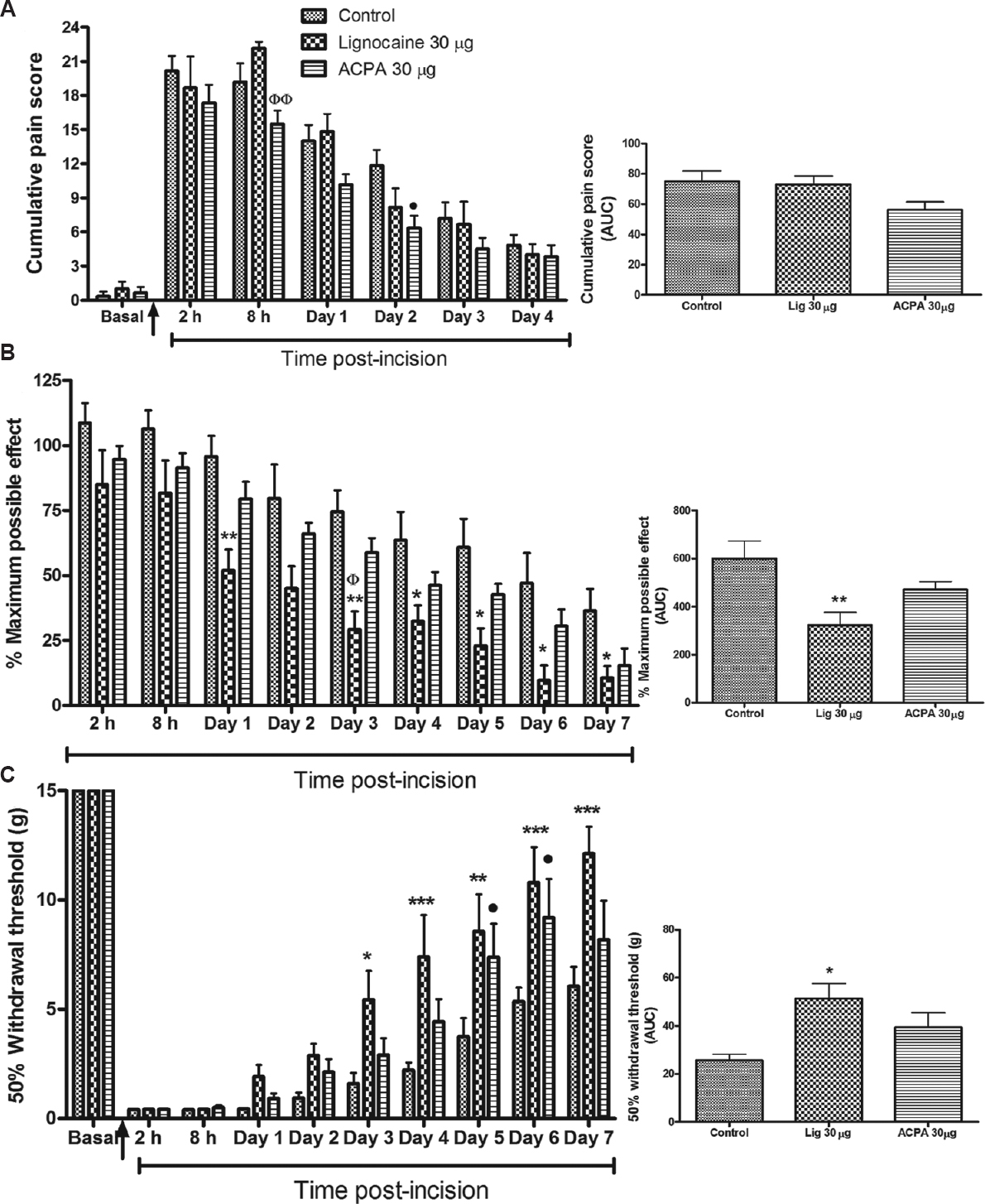
- Comparative antinociceptive effect of arachidonylcyclopropylamide (ACPA) and lignocaine. Overall antinociceptive effect represented by area under curve (AUC). (A) ACPA relieved guarding behaviour at 8 h compared to lignocaine treated group (Φ) and at day two compared to control group (•). (B) Lignocaine treatment significantly decreased thermal hyperalgesia (days 1 and 3-7) compared to control (*) and to ACPA treated group (Φ) (day 3). AUC was significantly decreased compared to control group (*) (C) Mechanical allodynia showed significant attenuation as evident from an increase in the withdrawal threshold following lignocaine treatment on days 3-7 compared to control group (*). ACPA also increased threshold compared to control group on days 5-6 (•). •P<0.05 ACPA compared to control; P Ф<0.05 ФФ<0.01 ACPA compared to lignocaine; P*<0.05 **<0.01 ***<0.001 lignocaine compared to control.
Immunostaining for c-Fos in spinal cord: The number of c-Fos-stained nuclei per unit area within the superficial laminae was significantly less for the 100 μg ACPA-treated group with reference to the control group (Fig. 5).
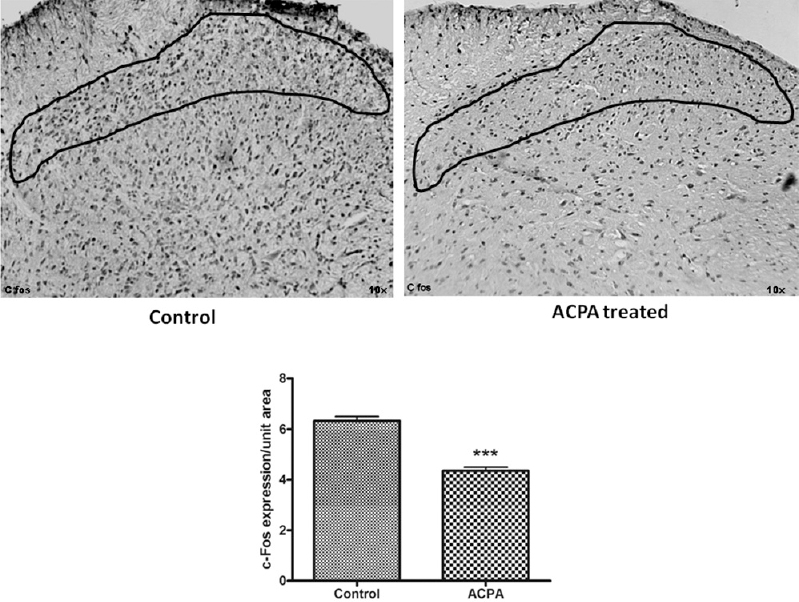
- c-Fos immunostaining in the spinal cord. It was significantly reduced following arachidonylcyclopropylamide (ACPA) treatment. n=6 rats in each group. Values are mean±SEM. ***P<0.001 compared to control.
Evaluation of incision site for healing process: Healing of the incised area in the ACPA-treated group was comparable to the control animals (Fig. 6). There was resolution of the inflammatory process with re-establishment of continuity of epithelial cells across the incision site on day eight.
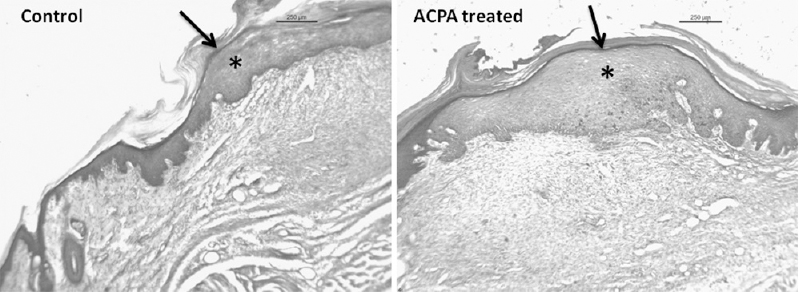
- Histological evaluation of the wound after arachidonylcyclopropylamide (ACPA) treatment. There is comparable repair with re-establishment of continuity of the layers of the skin. Dermis (*) was thicker in the arachidonylcyclopropylamide-treated group. Site of incision indicated with an arrow. n=6 rats in each group. Bar - 250 μm.
Motor activity after ACPA treatment: Following tissue injury, there was decreased locomotor activity at two hours, but this was not significantly different from that of the control group (Fig. 7). Intrawound ACPA (30 and 100 μg)-treated groups showed increased activity, which was dose-dependent. Furthermore, the higher dose normalized movements to those in the control group though significant difference was absent.
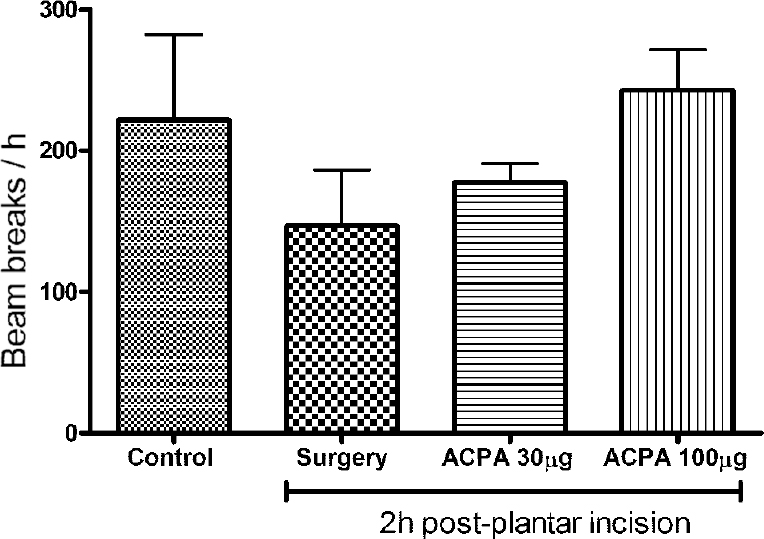
- Effect of arachidonylcyclopropylamide (ACPA) on horizontal locomotor activity in rats. ACPA (30 and 100 μg) treatment progressively increased locomotor activity in the rats though these were not significantly different. n=6 rats in each group. Values are mean±SEM.
Discussion
The results indicated that ACPA, particularly the 100 μg dose, attenuated guarding behaviour by binding to local CB1r, expressed by the nociceptors. The antinociceptive effect was reversed by AM251. The findings of this study provide evidence regarding the possibility of treating inflammatory pain arising from surgery by local administration of a CB1r agonist. Moreover, CB1r expression has been noted to increase 1-2 days after inflammation25, which would then further increase the antinociceptive effect. In our study, a significant inhibition of guarding score was observed between days one and two in comparison to control group. Several studies have demonstrated antinociception following activation of peripherally expressed cannabinoid receptors in rodents89151626, monkeys27 and humans28. The advantages of intrawound drug administration are that the drug acts locally at the site of tissue damage, relatively low doses are effective and lesser chances of untoward systemic side effects.
Rodents’ guarding behaviour has been suggested to represent pain at rest following surgery2021. It is possibly due to spontaneous activity of nociceptors at the injury site21 and is attenuated by morphine at doses equivalent to that in humans29. Guarding was also found to increase after damage to deeper tissues compared to just superficial injuries to the skin22. In contrast, thermal hyperalgesia was unaffected whereas allodynia was significantly decreased from days 5-7. This indicates that the underlying molecular basis for guarding could be different from other pain-related behaviours. The transient receptor potential vanilloid 1 (TRPV1) ion channels are expressed by nociceptors and are responsible for thermal hyperalgesia following hind paw incision30. However, endocannabinoids such as anandamide can activate TRPV1 receptors at high doses and even induce nocifensive behaviour after intraplantar injection3132. In our study, thermal hyperalgesia was worsened by the 100 μg dose compared to the 30 μg dose, though not significantly. It is likely that ACPA activated the TRPV1 receptors at the higher dosage. Allodynia was also worsened by this dose.
Inhibition of guarding by 30 μg ACPA alone was significantly reversed by AM251 (between 8 h and day 1) and AM251 alone further reversed the inhibition of guarding. This was despite the fact that ACPA 30 μg alone did not produce significant antinociception at this time point. AM251 is an inverse agonist which is well documented and it is likely that this property could have played a role in the greater reversal of antinociceptive effect than that expected32. In our study, guarding was worsened after administration of AM251 in comparison to the control group, on day one. Thermal hyperalgesia was also reversed by AM251.
Lignocaine (30 μg/10 μl) did not significantly inhibit guarding behaviour under similar experimental conditions to ACPA. It is an extensively used local anaesthetic with a prompt onset of action that lasts for up to one hour in its plain form33. Both thermal hyperalgesia and mechanical allodynia were significantly inhibited by lignocaine in contrast to ACPA. The precise reason needs to be investigated. Our observations were corroborated by a previous study in rats, wherein 4 mg of 2 per cent lidocaine, a more than 100-fold increase compared to our dose, injected beneath the epineurium of sciatic nerve had minimum antinociceptive effect (decreased allodynia only on days 6-7) after tissue damage34.
Lesser expression of c-Fos in the ACPA-treated spinal cord suggests a decrease in the noxious afferent input to the spinal cord from the site of tissue damage35. In an earlier study, preemptive nerve block along with intraplantar infiltration with two per cent lignocaine suppressed c-Fos expression in the spinal cord36. In this study, maximum c-Fos expression was noted one hour after tissue damage. Hence, this time point was used in our study. Previously, peripheral administration of WIN 55212-2 (a combined CB1 and 2 receptor agonist) suppressed c-Fos activation in the spinal cord following intraplantar carrageenan injection37. These evidences point towards decreased activation of nociceptors following peripheral ACPA administration. Lignocaine-treated rats were not processed for c-Fos staining because the corresponding antinociceptive effect was not significantly different from the control group at the earliest time point examined (2 h). In addition, at 8 h, guarding behaviour was increased compared to the control group.
Healing of the wound was found to be within normal limits. This was in agreement with a previous study where wound granulation tissue was observed to express cannabinoid receptors38. Blocking these receptors had a deleterious effect on the healing process39.
One of the important findings of this study was the prolonged antinociceptive effect of ACPA. A reasonable explanation could be that ACPA binds to the CB1r expressed on the nociceptors, after intrawound administration. Immediately after tissue damage within the first few hours, there is an explosive burst in the release of inflammatory mediators. Subsequently, this release gradually decreases. During the initial period, inflammatory mediators produce maximum peripheral sensitization after binding to appropriate receptors in the nociceptors. We hypothesized that concurrent binding of ACPA to CB1r did not allow the peripheral sensitization to progress as much as it would in naive animals. Notably, peripheral and not central sensitization has been noted previously to have a key role in incision-induced guarding behaviour20.
In conclusion, our results showed that intrawound administration of ACPA relieved guarding behaviour, while lignocaine attenuated thermal hyperalgesia and mechanical allodynia. It may be due to their different mechanisms of antinociceptive action (sodium ion channels for lignocaine versus CB1r for ACPA). This effect of ACPA may have clinical relevance in the treatment of pain associated with burn injury, trauma and surgical operation. Further studies are required to explore this novel antinociceptive effect in clinical conditions.
Acknowledgment
The authors acknowledge the Department of Biotechnology and the Indian Council of Medical Research, New Delhi, for financial support.
Conflicts of Interest: None.
References
- Opioids, analgesia and pain management. In: Brunton LL, ed. Goodman and Gilman's the pharmacological basis of therapeutics. New York: McGraw-Hill; 2011. p. :481-525.
- [Google Scholar]
- Marijuana and the cannabinoids. In: Meyer JS, Quenzer LF, eds. Psychopharmacology: drugs, the brain and behaviour. Massachusetts: Sinauer Associates Inc; 2005. p. :328-45.
- [Google Scholar]
- Psychopharmacology. In: Satoskar RS, Rege NN, Bhandarkar SD, eds. Pharmacology and pharmacotherapeutics. Mumbai: Popular Prakashan Private Limited; 2013. p. :193-229.
- [Google Scholar]
- International union of pharmacology. XXVII. Classification of cannabinoid receptors. Pharmacol Rev. 2002;54:161-202.
- [Google Scholar]
- Site-specific increases in peripheral cannabinoid receptors and their endogenous ligands in a model of neuropathic pain. Pain. 2006;126:102-14.
- [Google Scholar]
- Distribution of cannabinoid receptor 1 (CB1) and 2 (CB2) on sensory nerve fibers and adnexal structures in human skin. J Dermatol Sci. 2005;38:177-88.
- [Google Scholar]
- Cannabinoids mediate analgesia largely via peripheral type 1 cannabinoid receptors in nociceptors. Nat Neurosci. 2007;10:870-9.
- [Google Scholar]
- A peripherally restricted cannabinoid receptor agonist produces robust anti-nociceptive effects in rodent models of inflammatory and neuropathic pain. Pain. 2010;151:337-44.
- [Google Scholar]
- Antinociceptive effect of intrathecal cannabinoid receptor agonist WIN 55,212-2 in a rat bone tumor pain model. Neurosci Lett. 2011;493:67-71.
- [Google Scholar]
- Central and peripheral sites of action for CB2 receptor mediated analgesic activity in chronic inflammatory and neuropathic pain models in rats. Br J Pharmacol. 2011;162:428-40.
- [Google Scholar]
- Tonic modulation of spinal hyperexcitability by the endocannabinoid receptor system in a rat model of osteoarthritis pain. Arthritis Rheum. 2010;62:3666-76.
- [Google Scholar]
- Role of CB1 and CB2 cannabinoid receptors in the development of joint pain induced by monosodium iodoacetate. Pain. 2013;154:160-74.
- [Google Scholar]
- Medical marijuana for treatment of chronic pain and other medical and psychiatric problems: a clinical review. JAMA. 2015;313:2474-83.
- [Google Scholar]
- Chromenopyrazoles: non-psychoactive and selective CB1 cannabinoid agonists with peripheral antinociceptive properties. ChemMedChem. 2012;7:452-63.
- [Google Scholar]
- Anandamide suppresses pain initiation through a peripheral endocannabinoid mechanism. Nat Neurosci. 2010;13:1265-70.
- [Google Scholar]
- Structure of a cannabinoid receptor and functional expression of the cloned cDNA. Nature. 1990;346:561-4.
- [Google Scholar]
- Cannabinoids reduce hyperalgesia and inflammation via interaction with peripheral CB1 receptors. Pain. 1998;75:111-9.
- [Google Scholar]
- Locally mediated analgesic effect of bradykinin type 2 receptor antagonist HOE 140 during acute inflammatory pain in rats. J Burn Care Res. 2014;35:e391-8.
- [Google Scholar]
- Guarding pain and spontaneous activity of nociceptors after skin versus skin plus deep tissue incision. Anesthesiology. 2010;112:153-64.
- [Google Scholar]
- Quantitative assessment of tactile allodynia in the rat paw. J Neurosci Methods. 1994;53:55-63.
- [Google Scholar]
- Induction of c-fos-like protein in spinal cord neurons following sensory stimulation. Nature. 1987;328:632-4.
- [Google Scholar]
- Antinociceptive effects of curcumin in a rat model of postoperative pain. Sci Rep. 2014;4:4932.
- [Google Scholar]
- Induction of CB1 cannabinoid receptor by inflammation in primary afferent neurons facilitates antihyperalgesic effect of peripheral CB1 agonist. Pain. 2006;124:175-83.
- [Google Scholar]
- Topical cannabinoid antinociception: synergy with spinal sites. Pain. 2003;105:11-6.
- [Google Scholar]
- Local administration of delta9-tetrahydrocannabinol attenuates capsaicin-induced thermal nociception in rhesus monkeys: a peripheral cannabinoid action. Psychopharmacology (Berl). 1999;143:322-6.
- [Google Scholar]
- Cannabinoid agonists attenuate capsaicin-induced responses in human skin. Pain. 2003;102:283-8.
- [Google Scholar]
- Ketoprofen produces modality-specific inhibition of pain behaviors in rats after plantar incision. Anesth Analg. 2009;109:1992-9.
- [Google Scholar]
- Effect of AMG0347, a transient receptor potential type V1 receptor antagonist, and morphine on pain behavior after plantar incision. Anesthesiology. 2008;108:1100-8.
- [Google Scholar]
- Excitation of cutaneous C nociceptors by intraplantar administration of anandamide. Brain Res. 2009;1268:38-47.
- [Google Scholar]
- Lignocaine toxicity; a complication of local anaesthesia administered in the community. Emerg Med J. 2004;21:249-50.
- [Google Scholar]
- Prolonged suppression of postincisional pain by a slow-release formulation of lidocaine. Anesthesiology. 2011;114:135-49.
- [Google Scholar]
- Cannabinoid receptor agonists inhibit glutamatergic synaptic transmission in rat hippocampal cultures. J Neurosci. 1996;16:4322-34.
- [Google Scholar]
- The effects of pretreatment with lidocaine or bupivacaine on the spatial and temporal expression of c-fos protein in the spinal cord caused by plantar incision in the rat. Anesth Analg. 2004;98:1093-8.
- [Google Scholar]
- A peripheral cannabinoid mechanism suppresses spinal fos protein expression and pain behavior in a rat model of inflammation. Neuroscience. 2003;117:659-70.
- [Google Scholar]
- Involvement of the endocannabinoid system in periodontal healing. Biochem Biophys Res Commun. 2010;394:928-33.
- [Google Scholar]
- CB1 cannabinoid receptor-mediated cell migration. J Pharmacol Exp Ther. 2000;294:204-9.
- [Google Scholar]




