
Translate this page into:
Fats & fatty acids in Indian diets: Time for serious introspection
Reprint requests: Dr Indu Mani, Department of Physiology, Division of Nutrition, St. John's Medical College, Bengaluru 560 034, Karnataka, India e-mail: indu2004@gmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Recommended dietary allowances for fat and fatty acid (FA) intakes are set on global standards aimed at prevention of lifestyle diseases. Yet, the fat composition of a diet is both ethnic/region specific as well as income dependent. Indian diets are predominantly vegetarian and relatively low in fat. Furthermore, the main sources of fat are of plant origin rather than animal origin. This results in a diet that is relatively low in saturated FA, high in n-6 polyunsaturated fatty acids (PUFA), and very low in n-3 PUFA. Though this appears as a good dietary composition as per global standards, the undeniable increase in the incidence of obesity, diabetes and cardiovascular diseases in India begs for an explanation. In this context, the current article is aimed at reopening the debate on fat intakes in Indian diets, with a focus on a balance between fats, carbohydrates and proteins, rather than an emphasis on individual macronutrients.
Keywords
Fat
Indian diets
linoleic acid
linolenic acid
obesity
saturated fatty acids

Introduction
Fats have been criticized for the right as well as wrong reasons. The increasing incidence of lifestyle disorders such as cardiovascular diseases (CVDs) has been mainly attributed to an increased intake of fats. However, several studies, including meta-analyses of large-scale data sets, have thrown up doubts about the validity of this ‘diet-heart’ hypothesis123. This has led to some serious deliberations in the Western world, leading to modifications in the recommendations of daily dietary fat intakes45. However, these may not be universally applicable. In contrast to Western diets, Indian diets are typically higher in carbohydrates (CHO) and lower in fats and proteins. This review aims to address the quantity and quality of fat intake in Indian diets to state that it is time to reassess the diet-heart hypothesis specifically in the Indian context.
Dietary fats and fatty acids
Fats are the main sources of energy for the body, but the type of fat and the total amount of fat consumed daily play an important role in maintaining the state of health. Dietary fat is composed predominantly of triglycerides (TGs) (98%), with small amounts of phospholipids and sterols. The fatty acids (FAs) in TGs are classified as follows: saturated FAs (SFAs), cis-monounsaturated FAs (MUFA) and cis-polyunsaturated FAs (PUFAs) of the n-6 and n-3 families. In addition, small amounts of trans FAs (TFAs) are also found in the diet. Of all the FAs, only linoleic acid (LA, 18:2 n-6) and alpha-linolenic acid (ALNA, 18:3 n-3) are considered as essential fatty acids (EFAs) since these cannot be synthesized in the body. LA and ALNA are further elongated and desaturated in the body to give rise to the metabolically important long-chain derivatives such as arachidonic acid (20:4 n-6), eicosapentaenoic acid (20:5 n-3) and docosahexaenoic acid (22:6 n-3).
Sources of dietary fats are both plant and animal based. Animal fats tend to be rich in SFA whereas plant sources such as vegetable oils are predominantly rich in MUFA and PUFA such as LA and ALNA. Long-chain (LC) n-3 FAs are obtained predominantly through marine sources such as salmon and mackerel, and TFAs are mainly formed as by-products during the industrial processing of vegetable oils to produce hydrogenated fat6.
A brief history of dietary recommendations on fats by the US Dietary Guidelines Advisory Committee (DGAC)
The interest in and importance of dietary fats were highlighted largely due to the seminal Seven Countries study conducted by Keys78, which found a significant relation between fat intake and mortality due to CVD. This led to the 1980 DGAC dietary guidelines9 to ‘reduce overall fat intake to 30%E’. The unfortunate outcome of a rigorous implementation of such a recommendation has been well documented in the USA9. Till the mid-1970s, the US diet contained about 40%E from fats. The persistent focus on reducing fats resulted in the decrease in this proportion to 37%E in 1988 and further down to 34%E by 1995910. In the meantime, the caloric intake as well as the contribution of CHO to the diet had increased significantly. By the turn of this century, it had become clear that the overwhelming focus on reducing fat intake had actually backfired on the health of the population, resulting in a dramatic increase in the incidence of overweight and obesity1112. Further studies have shown that fats, and even SFA, are not necessarily associated with risk for CVD23. Reassessments of large data sets such as the Minnesota Coronary Experiment and the Sydney Diet Heart Experiment have revealed that replacement of SFA by n-6 PUFA rich oils may have actually had deleterious outcomes on cardiac events113. Therefore, the diet-heart hypothesis is now being questioned for its validity.
The US Department of Agriculture5 and Department of Health and Human services5 revise their Dietary Guidelines for every five years, and 25 yr after the first recommendation to reduce fat to <30%E, the National Cholesterol Education Program in 2001 recommended that the total fat intake could be increased to 25-35%E, with low-fat diets having <25%E and high-fat diets having >35%E14. Further, over the past decade, dietary recommendations have further reduced their emphasis on fats (although continuing to remain cautious about SFA and TFA) and have now focussed more on refined sugars and salt5.
A brief history of dietary recommendations in India
The history of dietary recommendations in India began at a much later date. In the Cantor Lectures in 1936, McCarrison15, the founder director of the National Institute of Nutrition, Hyderabad, India referred to the differences in the qualities of diets from various parts of India. Most nutrition-related research in India dealt with the problems of malnourishment and lack of availability of the basic nutrients. In the surveys conducted by the Director General of the Indian Medical Services in the 1930s and 1940s it was mentioned that only 39 per cent of the population were well nourished, while 41 per cent were ‘poorly nourished’ and 20 per cent were ‘very poorly nourished’1617.
After independence, several indigenous measures were taken to improve the nutritional status of the populace, and while the green revolution went a long way in reducing malnutrition, it had a number of deleterious outcomes18. The main negative feature of this programme was the focus on only two crops – rice and wheat at the expense of nutritionally important accompanying crops such as pulses and millets.
The role of fats in the diet was never a part of nutrition debates in India, until the 1980s and 1990s, when the initial dietary guidelines and Recommended Dietary Allowances (RDA) were published, for implementation on a national level19. At this point, it was clear that the dietary patterns of Indians were vastly different from a typical ‘Western’ diet, with relatively high intakes of CHO and low intakes of fat. In the first RDA report19, a minimum intake of total fat of 15%E was recommended to ensure adequate consumption of calories, essential FAs and fat-soluble vitamins. Based on the FAO/WHO (1977) recommendations20, the upper limit was set at 30%E, which was increased to 35%E in the 2010 publication of the Indian RDA21.
Recommendations for individual FAs were generally based on the minimum requirements to prevent deficiencies. Since SFA and MUFA can be synthesized in the body, no RDA was specifically mentioned for these. The requirement of LA, one of the essential FAs was based on a minimum of 3%E required to prevent deficiency. While the rationale behind setting the minimum requirement for ALNA was not clear, the AMDR for LA and ALNA was set as 2.5-9.0%E and 0.5-2%E, respectively21. In addition, the recommendations also included the daily consumption of at least 200 mg n-3 PUFA. This was based on the US Dietary Guidelines Advisory Committee (USDGAC) recommendations22, which in turn, was based on average intakes of marine fish in the USA. The upper limit for TFA intake was based on global recommendations of <1%E22.
In both the RDA reports1921, it was cautioned that in large parts of India, the major thrust ought to be to increase fat intakes since the major issue at hand was that of low intakes of total fat and n-3 PUFA23. However, this word of caution appears to have been lost in the general risk reduction clamour against the intake of fats. Therefore, the general emphasis in India, for all the population, continues to be on a relatively low-fat diet, with examples of a typical healthy diet comprising 20-25%E fat and 60-68%E from CHO.
Fats and fatty acids in Indian diets
The main sources of fat in a typical Indian diet (which is predominantly either rice or wheat based) are vegetable oils, ghee (clarified butter), milk and dairy products. With the publication of the Indian RDA19 and the general hype against the use of SFA in the diet, the dietary advice given in the 1980s and 1990s was to reduce the intake of ghee and traditional oils such as coconut and groundnut oils and to use new PUFA-rich oils such as safflower and sunflower oils.
The National Nutrition Monitoring Bureau data showed that between 1980 and 2002, there was an increase in the dietary intake of fat, both in urban and rural India24. However, it was important to note that the overall fat intake continued to be <15%E in many States of India25. Pingali and Khwaja26 have shown that although the total per capita caloric intake has increased over the past three decades, yet the contribution of animal food sources (that contain SFA) continues to be minimal. Surveys by the Indian Agricultural Research Institute27 have suggested that the trends in consumption of different edible oils have changed over the past three decades. There has been an overall increase in the consumption of refined oils, with decreased intakes of ghee/vanaspati. A significantly higher consumption of oils (such as sunflower, soybean and other unsaturated vegetable oils) reflects a greater concern for consumption of healthier edible oils, both in urban and rural areas. Thus, it appears that the hype against SFA was certainly effective.
n-6 and n-3 PUFA in Indian diets
The most abundant PUFA in most plant products is LA. Therefore a typical, balanced Indian diet would provide reasonable amounts of LA irrespective of the type of vegetable oil used. In fact, the data used to compute the minimum amount of fat in the diet required to prevent EFA deficiency were based on the assumption that the vegetable oil would contain only 20 per cent of LA19.
Dietary n-3 PUFA are of two types – the precursor, ALNA, is available in plant sources, especially green leafy vegetables and some vegetable oils, and the LC n-3 PUFA is only present in marine fish and certain types of seaweed. The intake of marine fish in Indian diets is very low except in specific coastal regions, and, therefore, the average intakes of LC n-3 PUFA are negligible2328. Thus, ALNA is the predominant source of n-3 FA. The conversion of ALNA to its LC products occurs by a series of enzymes – the desaturases and the elongases. The rate-limiting enzyme in this conversion is the Δ6-desaturase, which acts both on LA as well as on ALNA. While in vitro studies have shown that the substrate preference of this enzyme occurs in the order 18:3n-3 > 18:2n-6 > 18:1n-92930, it is also clear that high levels of LA can inhibit the conversion of ALNA31. It is, therefore, recommended that the dietary ratio of LA/ALNA should not be >10, and should preferably be in the ratio of 5:1. The increased consumption of PUFA-rich oils such as safflower (>70% LA, 0% ALNA) and sunflower (>60% LA, 0% ALNA), at the expense of more traditional oils such as coconut, groundnut and sesame, has resulted in a very skewed ratio of n-6 and n-3 FA.
The dietary recommendations by the Indian Council of Medical Research (ICMR)1921 have always stressed on increasing n-3 PUFA intake in Indian diets; however, it is not quite clear how that can be achieved. One suggestion given is to use a combination of vegetable oils. The only oils that contain reasonable amounts of the n-3 FA, ALNA, are mustard oil, soybean oil and canola oil. While mustard oil is commonly consumed in the northern and eastern Indian States, the abundance of erucic acid (22:1 n-9) in this oil (~45%) has always raised a question about its overall nutritive value. Moreover, oils such as mustard and soybean have a flavour that is not acceptable to the southern and western Indian States. Canola oil is a good option, but the main problems concerned with this oil are its cost and availability, especially since attempts to cultivate it in India have not been very successful32.
Fatty acid intakes in the context of global patterns: the current situation in India
Global data on dietary intakes show significant differences in diet composition between the high-income and low-income countries with respect to fat and CHO intakes; however, the levels of SFA are similar across economies33. Indian diets, on the other hand, contain lower fat as well as SFA, both in urban as well as rural surveys2434 (Table I).
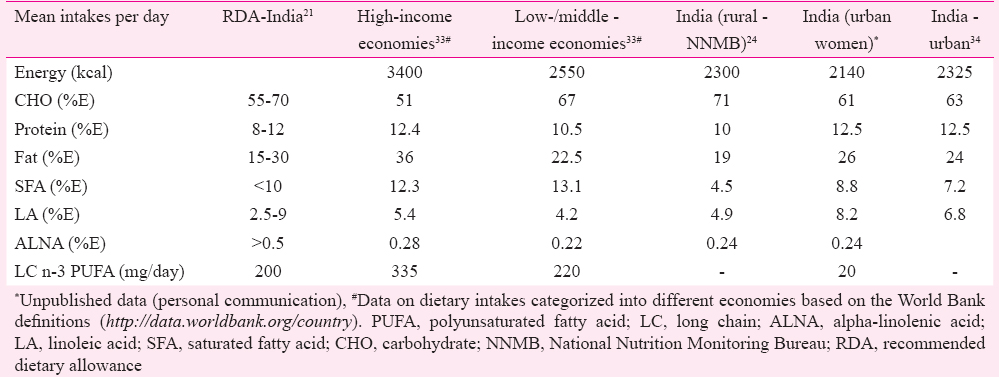
It is also clear that the intake of LA in Indian diets is relatively high compared to global intakes. This overall lower intakes of fat, SFA and higher intakes of PUFA ought to have been the ideal diet for the population, especially in terms of controlling metabolic disorders such as CVD. However, that is not the case, and therefore, this brings to the forefront a different aspect of the diet-fat-health equation – are there any repercussions of consuming a low-fat, high-n-6 PUFA, low-n-3 PUFA diet?
Increasing obesity in India – role of fatty acids?
There is no doubt that India is facing a dual burden, with problems at both ends of the nutritional spectrum. The increasing incidence of non-communicable diseases (NCDs) has been well documented35 and already, 53 per cent of deaths in India are due to NCDs. A recent study shows that the number of obese men has gone up from 0.4 million in 1975 to 9.8 million in 2014 while the number of obese women has increased from 0.8 million in 1975 to 20 million in 201436. Even more worrisome is the fact that the number of severely obese women has gone up from 0.1 million to 3.7 million36. Equally troubling, the number of extremely low body mass index (BMI) adults in India is also one of the highest in the world3637; low BMI is the sine qua non of chronic energy deficiency, in which diets have low fat content.
Many factors have a role to play in the increasing overweight/obesity epidemic in India. The ‘thrifty gene’ hypothesis38, the ‘Barker’ hypothesis39, the ‘adipose tissue overflow’ hypothesis40 and ‘the mitochondrial inefficiency’ theory41 are some of the genetic/epigenetic causes that have been cited; however, it is impossible to ignore the possibility that there is also a dietary component to this epidemic. How much does fat and FA intake contribute to this? Popkin et al42 predicted a likely increase in total fat and a doubling of SFA intake in Indian diets between 1995 and 2025. However, in spite of a doubling of intake, the average SFA intake would still be well within the current recommendation of <10%E. This clearly indicates that SFA may not be the main dietary culprit in increasing the risk of obesity, and that it is important to look at other factors such as CHO, and the PUFA, as more likely candidates.
High n-6 PUFA and low n-3 PUFA intakes
Even as early as in the 1990s, researchers cautioned against the recommendations to replace SFA with PUFA without distinguishing between the n-6 and n-3 families43. While n-6 PUFAs clearly have lipid-lowering effects, these are also pro-inflammatory in nature and have been shown to have adverse effects at higher intakes44. Studies conducted in animals have shown that high LA diets, especially in combination with a low-fat diet, result in a pro-inflammatory condition resulting in an increased deposition of adipose tissue4546. Increased intake of LA during pregnancy has been found to be associated with an intergenerational cycle of obesity47. Animal studies have shown that low ALNA intake can result in increased adiposity48, thus suggesting that an increased n-6/n-3 ratio could be an emerging risk factor for obesity49.
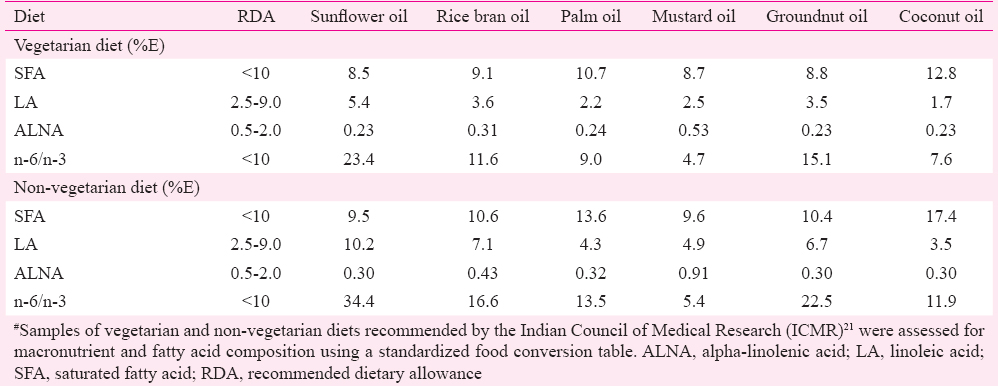
In India, where the consumption of LC n-3 PUFA is negligible, the n-6/n-3 ratio gains additional importance. Currently, a balanced vegetarian diet (for a normal human performing moderate amount of work) as recommended by the ICMR21, if cooked using different vegetable oils, would provide the amounts of FAs as shown in Table II. It is clear that using unsaturated oils such as sunflower oil has resulted in the skewing of Indian dietary PUFA intake towards a predominantly n-6 variety. This raises the important question - How far has this contributed to the bludgeoning obesity problem in India?
An introspection
It appears that two serious considerations need to be made that there are many people in India who do not get enough fats in their diet, and second, that the composition of a typical Indian diet unfortunately has all the components that lead to a deleterious plasma lipid profile – high CHO, low fat in diets of the poor, low SFA, high LA and low n-3 PUFA. The situation that India is facing now is somewhat similar to that faced by the USA in the 1980s and 1990s – a rapid increase in the incidence of obesity in spite of a lower fat and SFA intake50. The US Dietary Guideline Advisory Committee has actively responded to the situation, and the most recent revision of their dietary reference intake has removed the upper limit for fat intake4. It is time for India to take cognizance of the issues at hand and initiate steps to correct the potentially dangerous composition of the existing diets, to make informed decisions on what should be eaten and to educate the population appropriately. This does not mean a swing of the pendulum to the other side such that dietary recommendations are reversed to make unnecessary villains out of n-6 PUFA or CHO. It means that diets, especially with respect to macronutrients, cannot be dealt with in isolation, and restoring a balance between these nutrients should be the focus of future advice.
Given the rapid changes that have occurred in terms of advice, the subject of how much, and what fats to eat is now very confusing, not just to the consumer, but also to doctors as well as nutrition practitioners. A number of issues need to be considered. For example, do we need to reconsider the present guidelines separately through the prisms of requirements and chronic disease risk reduction? Perhaps there is no ‘one size fits all’ solution. How can the dichotomy of poor and middle class diets be addressed through guidelines – is this even possible?
Specifically, the daily requirement of n-3 PUFA as it has been enunciated needs to be re-examined. A large majority of Indians do not consume LC n-3 PUFA, and even non-vegetarians consume negligible amounts of marine fish. Available dietary information suggests that Indians consume, at most, about 20-50 mg n-3 PUFA per day28. In such a situation, the feasibility as well as the necessity of consuming at least 200 mg n-3 PUFA (as per the RDA) needs to be questioned. Recent data suggested that even low intakes of LC n-3 PUFA (20-40 mg/d) during pregnancy resulted in increased birth weight of infants and a reduced incidence of small for gestational age infants51. To generate evidence on the requirement of n-3 PUFA or LC n-3 PUFA, well-conducted epidemiological studies as well as randomized controlled trials need to be carried out to better understand the role of not only n-3 PUFA, but also the n-6/n-3 PUFA ratio in Indian diets. Finally, given the unambiguous evidence of the adverse effects of TFA, it is very important to find ways to reduce TFA in the diet, and also to clearly define natural sources of TFA to avoid confusion.
In addition to these introspective questions, clear and carefully crafted nutrition education programmes need to be created to clarify many of the confusing messages about fats. The following points are worth emphasizing: SFA intake has been actively discouraged in the past few decades. Instead, the message should stress on the balance between the types of FAs, rather than a distracting focus on individual FA types. The importance of the n-6/n-3 PUFA ratio has always been highlighted in education messages. While the benefit of a low ratio has been extolled, the actual harm that could be incurred due to a high ratio has never really been emphasized. India is at the developmental crossroads, where diets are increasing and becoming more accessible and diversified; it is critical that a well-informed policy should be laid out before lessons that have painfully been learnt in the West are forgotten.
Conflicts of Interest: None.
References
- Re-evaluation of the traditional diet-heart hypothesis: analysis of recovered data from Minnesota Coronary Experiment (1968-1973) BMJ. 2016;353:i1246.
- [Google Scholar]
- Saturated fat and cardiometabolic risk factors, coronary heart disease, stroke, and diabetes: a fresh look at the evidence. Lipids. 2010;45:893-905.
- [Google Scholar]
- Saturated fat and cardiovascular disease: a review of current evidence. Curr Cardiovasc Risk Rep. 2013;7:154-62.
- [Google Scholar]
- The 2015 US Dietary Guidelines: lifting the ban on total dietary fat. JAMA. 2015;313:2421-2.
- [Google Scholar]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015. 2015-2020 dietary guidelines for Americans. (8th ed). Available from: http://www.health.gov/dietaryguidelines/2015/guidelines/
- [Google Scholar]
- Atherosclerosis: a problem in newer public health. J Mt Sinai Hosp N Y. 1953;20:118-39.
- [Google Scholar]
- Dietary fats, eating guides, and public policy: history, critique, and recommendations. Am J Med. 2002;113(Suppl 9B):89S-106S.
- [Google Scholar]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services, Dietary Guidelines for Americans (7th ed). Washington, DC: U.S. Government Printing Office; 2010. January 2011. Adv Nutr 2011; 2: 293-94
- Overweight and obesity in the United States: prevalence and trends, 1960-1994. Int J Obes Relat Metab Disord. 1998;22:39-47.
- [Google Scholar]
- Prevalence and trends in obesity among US adults, 1999-2000. JAMA. 2002;288:1723-7.
- [Google Scholar]
- Use of dietary linoleic acid for secondary prevention of coronary heart disease and death: evaluation of recovered data from the Sydney Diet Heart Study and updated meta-analysis. BMJ. 2013;346:e8707.
- [Google Scholar]
- National Cholesterol Education Program. Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III), NHLBI, National Institutes of Health Publication 01-3670:11. Bethesda, MD: NIH; 2001.
- The “discovery” of malnutrition and diet in Colonial India. Indian Econ Soc Hist Rev. 1994;31:1-26.
- [Google Scholar]
- Indian Council of Medical Research. Nutrient requirements and recommended dietary allowances for Indians. Report of the Expert Group of the Indian Council of Medical Research. Hyderabad: National Institute of Nutrition; 1990.
- [Google Scholar]
- FAO Report of a Joint FAO/WHO Expert Consultation on Dietary. In: Fats and oils in human nutrition FAO technical papers 3. Rome: FAO; 1977.
- [Google Scholar]
- Indian Council of Medical Research. Nutrient requirements and recommended dietary allowances for Indians. Report of the Expert Group of the Indian Council of Medical Research. Hyderabad: National Institute of Nutrition; 2010.
- Institute of Medicine; Food and Nutrition Board. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids (macronutrients). Washington, DC: The National Academies Press; 2005.
- Fats in Indian diets and their nutritional and health implications. Lipids. 1996;31:S287-91.
- [Google Scholar]
- 2002. National Nutrition Monitoring Bureau (NNMB) Technical Report 21: Diet and Nutritional status of rural population, Annexure 7.2, National Institute of Nutrition, Hyderabad. Available from: http://wcd.nic.in/Schemes/research/nti1947/72%20dietary%20intakes%20pr%2042.pdf
- Correlation of regional cardiovascular disease mortality in India with lifestyle and nutritional factors. Int J Cardiol. 2006;108:291-300.
- [Google Scholar]
- 2004. Globalisation of Indian diets and the transformation of food supply systems. ESA Working Paper No. 04-05. Available from: http://www.fao.org/es/esa
- Edible oilseeds supply and demand scenario in India: implications for policy. New Delhi: Indian Agricultural Research Institute; 2012.
- Polyunsaturated fatty acid consumption and concentration among South Indian women during pregnancy. Asia Pac J Clin Nutr. 2009;18:389-94.
- [Google Scholar]
- The oxidative desaturation of unsaturated fatty acids in animals. Mol Cell Biochem. 1974;3:41-52.
- [Google Scholar]
- Specificity of delta 6 desaturase – Effect of chain length and number of double bonds. Adv Exp Med Biol. 1977;83:127-34.
- [Google Scholar]
- Dietary linoleic acid influences desaturation and acylation of deuterium-labeled linoleic and linolenic acids in young adult males. Biochim Biophys Acta. 1994;1213:277-88.
- [Google Scholar]
- Canola cultivation in India: scenario and future strategy. 2009. Proceedings of the 16th Australian Research Assembly on Brassicas. Ballarat Victoria. Available from: http://www.australianoilseeds.com/__data/assets/pdf_file/0009/6849/31_Canola_cultivation_in_India_scenario_and_future_strategy.pdf
- [Google Scholar]
- Global Burden of Diseases Nutrition and Chronic Diseases Expert Group NutriCoDE. Global, regional, and national consumption levels of dietary fats and oils in 1990 and 2010: a systematic analysis including 266 country-specific nutrition surveys. BMJ. 2014;348:g2272.
- [Google Scholar]
- Reproducibility and validity of an interviewer-administered semi-quantitative food frequency questionnaire to assess dietary intake of urban adults in Southern India. Int J Food Sci Nutr. 2006;57:481-93.
- [Google Scholar]
- Burden of non communicable diseases in India: setting priority for action. Int J Med Sci Public Health. 2013;2:7-11.
- [Google Scholar]
- NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19·2 million participants. Lancet. 2016;387:1377-96.
- [Google Scholar]
- Prevalence of body mass index lower than 16 among women in low- and middle-income countries. JAMA. 2015;314:2164-71.
- [Google Scholar]
- Insights from the developing world: thrifty genotypes and thrifty phenotypes. Proc Nutr Soc. 2005;64:153-61.
- [Google Scholar]
- Type 2 (non-insulin-dependent) diabetes mellitus, hypertension and hyperlipidaemia (syndrome X): relation to reduced fetal growth. Diabetologia. 1993;36:62-7.
- [Google Scholar]
- Why might South Asians be so susceptible to central obesity and its atherogenic consequences? The adipose tissue overflow hypothesis. Int J Epidemiol. 2007;36:220-5.
- [Google Scholar]
- Could mitochondrial efficiency explain the susceptibility to adiposity, metabolic syndrome, diabetes and cardiovascular diseases in South Asian populations? Int J Epidemiol. 2009;38:1072-81.
- [Google Scholar]
- Trends in diet, nutritional status, and diet-related noncommunicable diseases in China and India: the economic costs of the nutrition transition. Nutr Rev. 2001;59:379-90.
- [Google Scholar]
- What is the desirable ratio of saturated, polyunsaturated, and monounsaturated fatty acids in the diet? Am J Clin Nutr. 1997;66(4 Suppl):988S-90S.
- [Google Scholar]
- Health implications of high dietary omega-6 polyunsaturated fatty acids. J Nutr Metab 2012 2012:539426.
- [Google Scholar]
- Dietary linoleic acid elevates endogenous 2-AG and anandamide and induces obesity. Obesity (Silver Spring). 2012;20:1984-94.
- [Google Scholar]
- Temporal changes in dietary fats: role of n-6 polyunsaturated fatty acids in excessive adipose tissue development and relationship to obesity. Prog Lipid Res. 2006;45:203-36.
- [Google Scholar]
- Omega-6 polyunsaturated fatty acids and the early origins of obesity. Curr Opin Endocrinol Diabetes Obes. 2013;20:56-61.
- [Google Scholar]
- A low alpha-linolenic intake during early life increases adiposity in the adult guinea pig. Nutr Metab (Lond). 2010;7:8.
- [Google Scholar]
- An emerging risk factor for obesity: does disequilibrium of polyunsaturated fatty acid metabolism contribute to excessive adipose tissue development? Br J Nutr. 2008;100:461-70.
- [Google Scholar]
- 2000. Dietary Guidelines Advisory Committee. Dietary guidelines for Americans. Available from: https://health.gov/dietaryguidelines/dgac/pdf/dgac_ration.pdf
- Maternal fat and fatty acid intake and birth outcomes in a South Indian population. Int J Epidemiol. 2016;45:523-31.
- [Google Scholar]




