
Translate this page into:
Turner like dysmorphia as presenting feature of Type-II Mayer-Rokitansky-Kuster-Hauser syndrome
* For correspondence: deepdutta2000@yahoo.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
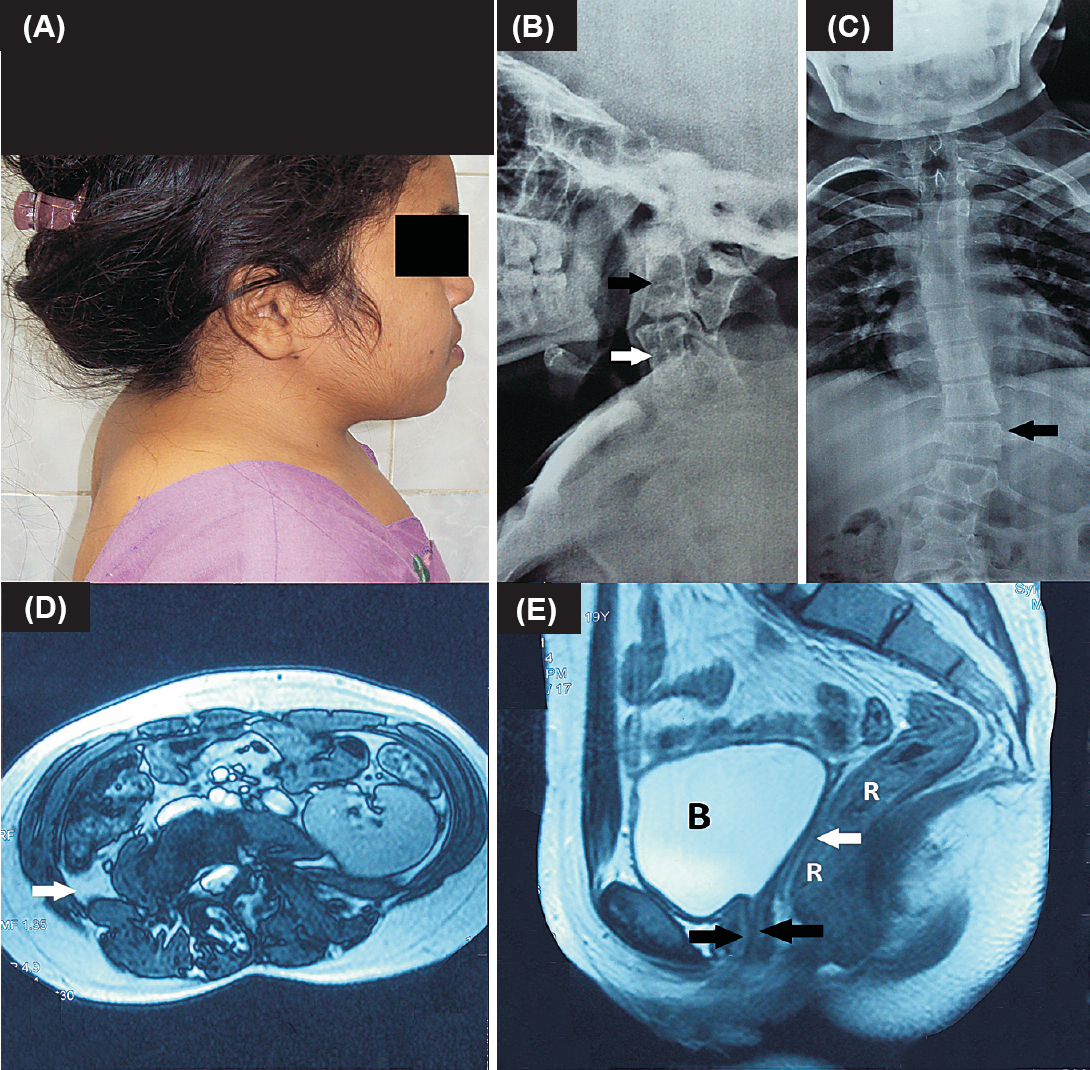
A 19 yr old girl with Turner-like dysmorphia (Figure A) (height: 131 cm; standard deviation: - 5.2 cm) presented to the Endocrinology clinic, Dr Ram Manohar Lohia Hospital, New Delhi, India, in November 2014 with complaints of primary amenorrhoea. Examination was significant for short neck, restriction of neck movements, scoliosis (Figure B, C), well developed breasts (B4), pubic hair (P3), axillary hair, normal estrogenized vulva, labia, clitoris with a blind vagina measuring 6 cm. Karyotype was normal (46XX) with normal hormones (luteinizing hormone: 2.44 mIU/ml; follicle stimulating hormone: 3 mIU/ml; estradiol: 68 pg/ml), ruling out Turner syndrome (TS). Short neck was due to type-II Klippel Feil (KF) anomaly (Figure B). Echocardiography showed small ostium secundum atrial septal defect (ASD). Presence of vertebral, cardiac and renal anomalies (right renal agenesis and malrotation of left kidney) (Figure D) along with Mullerian agenesis (Figure E) led to diagnosis of Type-II Mayer-Rokitansky-Kuster-Hauser syndrome (MRKH2). Mullerian agenesis (type I and II), which includes MRKH2 is the second most common cause of primary amenorrhoea (after TS). She was currently sexually inactive. Potential need for vaginal dilatational procedures/vaginoplasty in case of dyspareunia later in life was discussed. Scope for in vitro fertilization and surrogate pregnancy were considered as long-term fertility options due to absence of inner genital tract. In view of lack of neurodeficits or neck instability, surgical interventions for KF anomaly were deferred.
-
(A). Patient profile showing Turner like dysmorphia as evidenced by short neck and multiple facial nevi; (B). X-ray neck showing type-II Klippel Feil anomaly characterized by fusion of C2-C4 vertebrae (black arrow) and C5-C7 vertebrae (white arrow); (C). X-ray dorsolumbar spine showing scoliosis (black arrow) (D). Magnetic resonance imaging (MRI) abdomen showing right renal agenesis as evidenced by absence of kidney in right renal fossa (white arrow). Left kidney was malrotated; (E). MRI pelvis showing anterior and posterior lips of lower one third of vagina (black arrows), with absence of upper two-third of vagina, cervix and uterus (Mullerian agenesis) between bladder (B) and rectum (R) (white arrow).




