
Translate this page into:
Disseminated nocardiosis in a patient with sarcoidosis
* For correspondence: visitsrinivasan@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 64 year old male with well-controlled diabetes mellitus and fibrocystic sarcoidosis on steroids presented to the department of Pulmonology, Manipal Hospitals, Bengaluru, India, in October 2013 with a one week history of discharging ulcer and skin rash, and one day history of seizures with altered sensorium. His medications included oxygen at 1l/min, insulin, aspirin, 15 mg prednisolone, pantoprazole and calcium. Clinical examination showed a 2x2.5 cm ulcer with clean base and serous discharge over the left thigh. Multiple 2 x 3 cm reddish non-pruritic papules were present over both lower limbs and abdomen (Fig. 1). Repeat computed tomography of the chest did not show any new consolidation or cavitation (Fig. 2), but confirmed stage IV sarcoidosis. CT-head showed multiple space occupying lesions (Fig. 3A); magnetic resonance imaging of the head revealed multiple enhancing intracranial ring lesions (Fig. 3B). Cerebrospinal fluid examination showed 400 polymorphs/μl, elevated protein (105 mg/dl) and depressed sugar values (45 mg/dl, corresponding blood glucose 145 mg/dl) with normal adenosine deaminase levels (3 U/l, normal <8 U/l). Biopsy from nodules showed necrosis with lympho-mononuclear dermal infiltration and Grocott's stain revealed filamentous branching structures. Discharge from the ulcer showed long thin filamentous forms suggesting Nocardia that was confirmed on modified acid-fast staining (Fig. 4A); cultures were confirmed to be Nocardia asteroides (Fig. 4B). The patient was treated with phenytoin, ceftriaxone, amikacin and oral trimethoprim-sulphamethaxazole. Insulin and oxygen were continued and prednisolone tapered. Neurological abnormalities normalized by one week. At 12 months follow up, the patient was well.
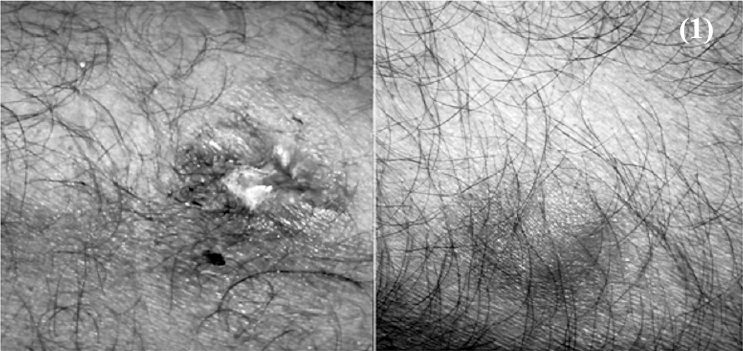
- Photomicrographs of the skin lesions showing a 2 × 2.5 cm ulcer with clean base and serous discharge over the left thigh. Multiple 2 × 3 cm reddish non-pruritic papules were present over both lower limbs and abdomen.
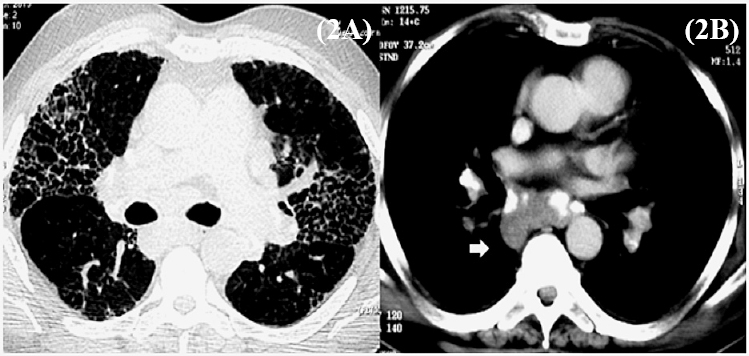
- Computed tomography (CT) of chest confirmed upper lobe predominant honey-combing and septal thickening (A) and large calcified right paratracheal, sub-carinal, bilateral hilar and paraaortic lymphadenopathy (B) consistent with prior diagnosed stage IV sarcoidosis. No cavitation, consolidation or evidence of pulmonary nocardiosis was seen.
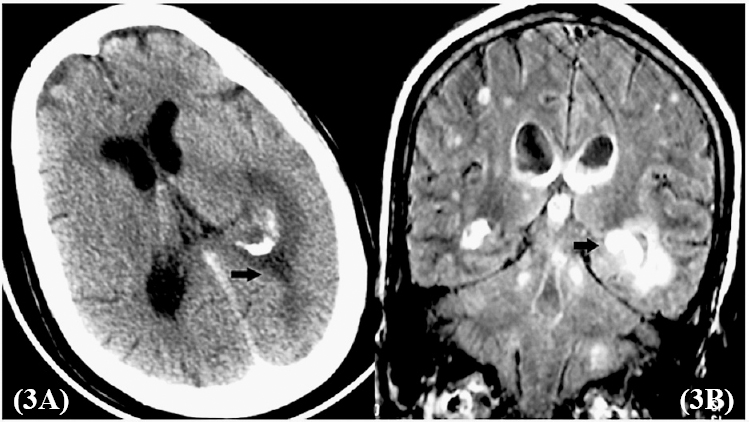
- Contrast enhanced computed tomography (CECT) of the head shows an enhancing hypoattenuated lesion over the left parietal lobe (a black arrow in Fig. 3A). Magnetic resonance imaging (MRI) of the head showing multiple enhancing ring lesions (arrow) in the cerebrum, cerebellum and brain stem (B) which were hyperintense on T1 and T2-weighted images with extension into the lateral ventricles.
-
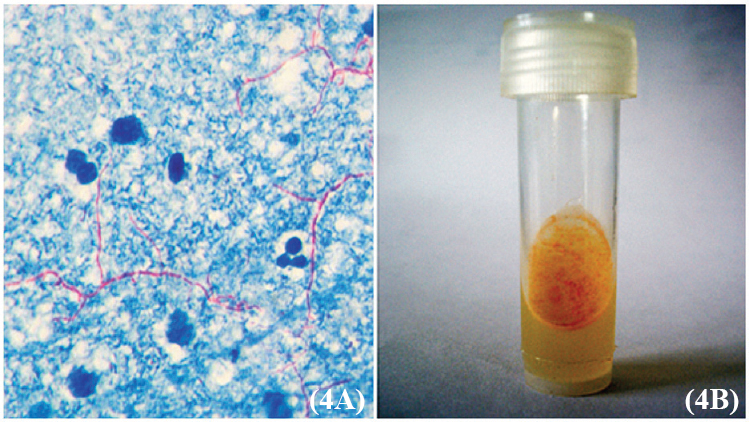
(A). Modified acid-fast staining (× 40) of the aspirate from the discharging ulcer showing presence of long thin filamentous forms suggesting Nocardia. Cultures grew buffy colonies (B) that were typed biochemically as Nocardia asteroides.
Acknowledgment
The authors thank Dr Vikas, department of Radiology, Manipal Hospitals, Benguluru for help in reporting the neuroradiology of this index patient and Dr Srivatsav Lokeswaran, department of Pulmonary Medicine, for help in patient management.
Conflicts of Interest: None.




