
Translate this page into:
Kimura disease: A rare case of bilateral infra-auricular masses
*For correspondence: beheravineet@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
A 35 year old male presented to the medicine outpatient department of Armed Forces Medical College, Pune, India, in April 2013, with a painless, progressive and irregular swelling below the both ears since last 10 years with no other systemic symptoms. Clinically, it was firm, non-tender, non-fluctuant swelling about 9x6 cm, located in bilateral infra-auricular areas (Fig. 1). The patient had eosinophilia and elevated IgE levels. His renal parameters and other investigations were normal. MRI showed bilateral lobulated non-homogeneous lesions with moderate contrast enhancement in bilateral parotid region as shown in Fig. 2. Fine needle aspiration cytology (FNAC) was inconclusive and biopsy was suggestive of a subcutaneous swelling with lobulated picture of lymphoid tissue separated by fibrous tissue with significant eosinophilic infiltrate.
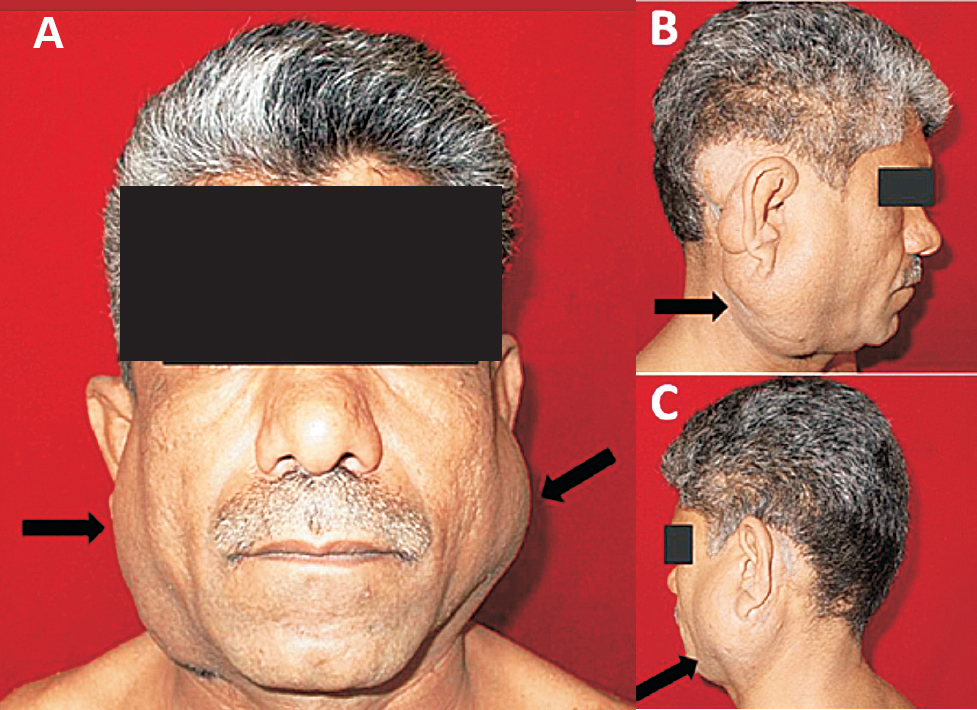
- (1A - Front view, 1B - Right lateral view, 1C - Left lateral view) shows bilateral infra-auricular swellings due to Kimura disease (arrows)
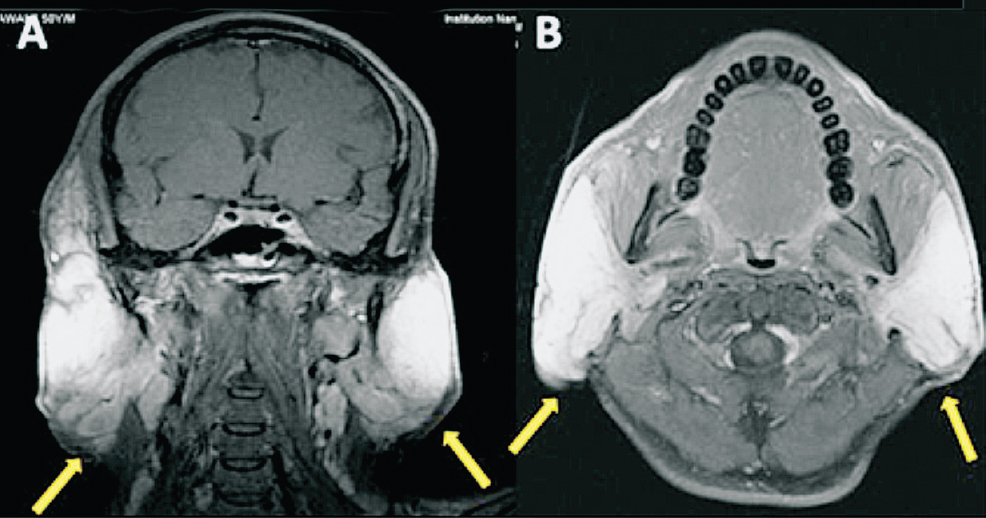
- MRI images (2A - axial section and 2B - transverse section) of the patient showing bilateral infra-auricular enhancing lesions (arrows)
Wide excision of swelling was done due to cosmetic indications. Operative findings showed subcutaneous masses which were firm, well defined, located superficial to the parotids with enlargement of intraparotid and other surrounding lymph nodes. The histopathology of the specimen confirmed Kimura's disease. He was continued on cetrizine 10 mg once daily and was closely followed up. After about six months, he had return of swelling initially in the left side followed by the right side possibly due to recurrence of disease which was confirmed by MRI. He was started on oral prednisone 40 mg/day and cyclosporine 200 mg/day which led to regression of swelling. Presently, the swelling has subsided and the patient is on maintenance of prednisone 5 mg on alternate days and cyclosporine.




