
Translate this page into:
Adherence to anti-retroviral therapy & factors associated with it: a community based cross-sectional study from West Bengal, India
Reprint requests: Dr Samiran Panda, National Institute of Cholera & Enteric Diseases (ICMR), P-33 CIT Road, Scheme-XM, Beliaghta, Kolkata 700 010, West Bengal, India e-mail: drsamiran_panda@rediffmail.com
-
Received: ,
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Failure to adhere to anti-retroviral therapy (ART) can lead to a range of unfavourable consequences impacting upon people living with HIV (PLH) and society. It is, therefore, paramount that ART adherence is measured in a reliable manner and factors associated with adherence are identified. Lack of such data from West Bengal necessitated undertaking the current study.
Methods:
Participants were included during August-October, 2011 from three Drop-In-Centres (DICs) from the three districts of West Bengal, India. ART-adherence was calculated by using formula based on pill-count and records collected from ART-card in possession of each of the 128 consenting adult PLH. Information on self-reported adherence, socio-demography, and adherence influencing issues was also collected through interviewer-administered questionnaire.
Results:
Of the 128 PLH, 99 (77%) and 93 (73%) PLH had ≥90 per cent and ≥95 per cent adherence, respectively to ART. Conversely, subjective reporting captured much higher proportion of PLH as ‘well adherent’; a finding having implications for ongoing ART programme. Factors, independently associated with poor adherence (<90%), were ‘7th to 12th month period of ART intake’ (adjusted OR=9.5; 90% CI 1.9 - 47.3; P=0.02) and ‘non-disclosure of HIV status to family members’ (adjusted OR=4; 90% CI 1.3 - 13; P=0.05. Results at 95 per cent adherence cut-off were similar.
Interpretation & conclusions:
Enabling environment, which would encourage people to disclose their HIV status and in turn seek adherence partners from families and beyond and ongoing adherence-counselling appear to be important issues in the programme. Relevance of these study findings in wider context is conceivable.
Keywords
Adherence counselling
ART
pill-count
treatment supporter
West Bengal

The National AIDS Control Programme (NACP) in India is currently in its fourth phase (2013-2017) of implementation and aims at expanding key HIV/AIDS services by integrating these with health systems of various stakeholders1. Bringing greater number of people under the provision of anti-HIV medicines distributed through government programme is an integral part of this plan. However, the challenge during such convergence and expansion would be ensuring certain level of adherence as failure to adhere to anti-retroviral therapy (ART) can have a range of unfavourable consequences for people living with HIV (PLH) as well as society at large. A study from eastern Indian State of Jharkhand has underlined this issue by identifying association of good adherence with higher chance of survival among PLH2.
Estimation revealed that till 2011 about 1,50,000 lives had been saved through provision of ART in the country1. These achievements are linked with expansion of facilities for providing free ART, which started with eight centres located in government hospitals in 2004 in six high prevalent States. The number of ART centres in the country increased to 107 in March 2007 and 380 as on December, 20121. Earlier to 2004, antiretroviral medicines were available in India in private sectors only and through some employer supported health insurance programmes from Employees’ State Insurance (ESI) scheme and railways3.
Specific concern with scaling up of ART in resource-limited setting is emergence of drug resistant viral strains due to suboptimal adherence and transmission of these resistant viral strains in the population4. Investigation by Paterson et al5, identified 95 per cent cut-off as the required adherence level for protease inhibitor (PI) containing treatment regimen for effective suppression of viral load. Further research however, revealed that viral load suppression might be achievable at lower adherence level if combination ART contains non-nucleoside reverse transcriptase inhibitor (NNRTI)67. Investigators from India in early 2000 adopted a pragmatic approach and a study conducted in Delhi and Pune used 90 per cent adherence cut-off for non-PI containing first line regimen3. Adherence studies conducted later in the country used higher (95%) cut-off value891011. A systematic review has summarized data from seven cross-sectional and one retrospective study enrolling 1666 individuals on ART (1322 male participants and 344 females). Three studies in this review were conducted in private treatment settings; two generated data from both private and public setting and the rest were from government hospitals. All these studies were published during 2005 - 2009. Pooled value of ART adherence rate was 70 per cent (95% CI 59-81%, I2=96.3%)12.
The present study was conducted in West Bengal, an eastern Indian State where currently 10 ART centres are functional and 570620 adults and 34367 children are alive with HIV and on ART1. The purpose of this study was to generate information on ART-adherence, which is lacking from West Bengal, and to identify factors associated with ART-adherence in this State.
Material & Methods
Study design, setting & participants: This cross-sectional study was carried out in 2011 by the Society for Positive Atmosphere & Related Support to HIV/AIDS (SPARSHA) in collaboration with the National Institute of Cholera & Enteric Diseases (NICED), Kolkata, India. Study participants comprised PLH attending Drop-In-Centres (DICs) of SPARSHA. DICs, recruiting study participants, were located in the three districts of West Bengal; Kolkata, West Medinipur and East Medinipur. The PLH attending these DICs had been receiving counselling, nutritional and social support services from these three DICs which did not include ART delivery. In counselling sessions, adherence was covered as a general topic and no specialized training was received by DIC based counsellors on ART-adherence. These DICs were financed by the West Bengal State AIDS Prevention and Control Society (WBSAP & CS) and managed by SPARSHA - a community based organization constituted by PLH and their friends (PLHAF). Prior to initiation of data collection, the study was approved by the institutional ethics committees of the Rabindra Bharati University and the NICED.
Participants were selected from PLH aged 18 yr or above (adult), attending monthly group meetings organized by SPARSHA. During the study period a total of 660 PLH attended meetings (375 were on ART) at the aforementioned three DICs, of whom 262 ART recipients were regular attendees. DIC-clients on ART received information about the study one month prior to recruitment and were asked to bring along their ART pill box and ART card on the day of group-meeting if they were willing to participate. One twenty eight PLH on ART providing informed consent and carrying their ART-pill box (128/262, 54%) were interviewed (Figure) during August through October, 2011. Despite working with a PLHAF-managed civil society organization, desirability bias might have influenced the validity of pill count, which otherwise serves as an objective measure of adherence.
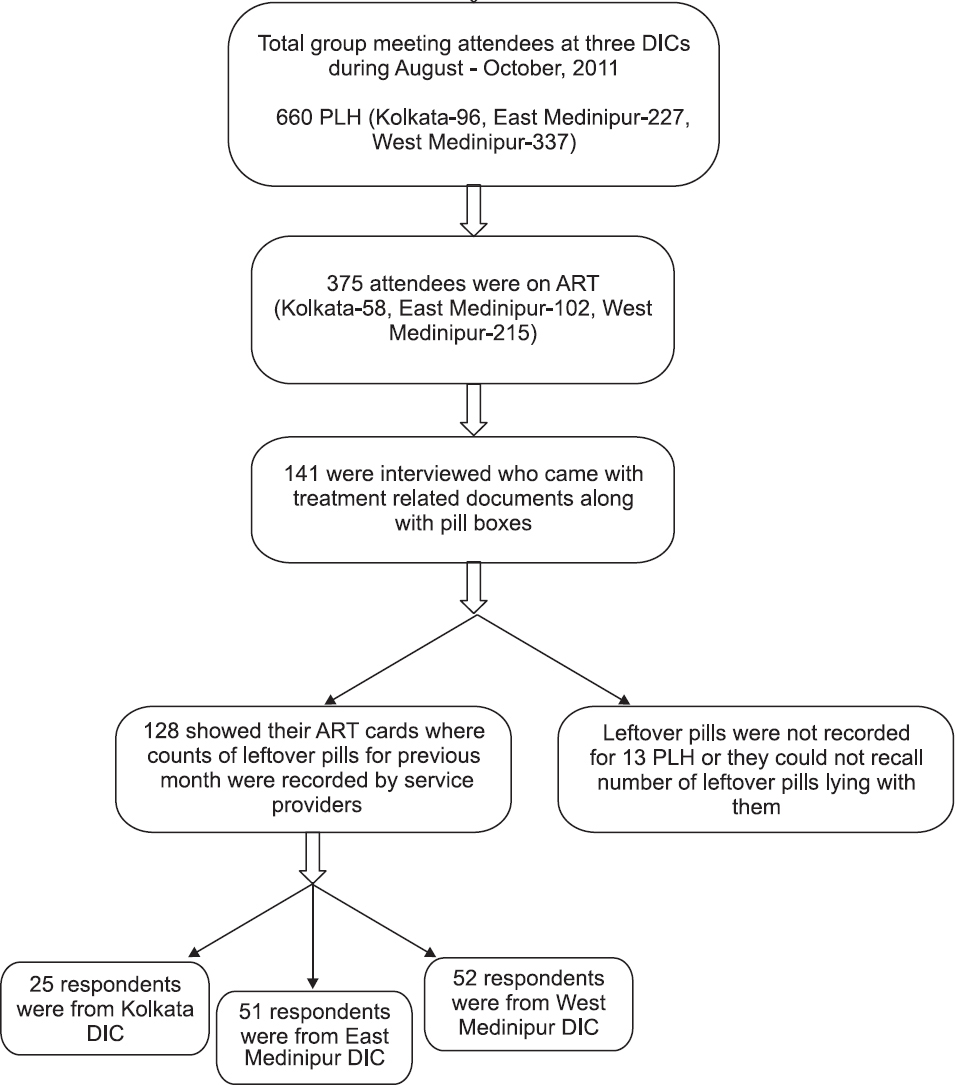
- Flow diagram showing the selection of participants. DIC, Drop-In-Centre; PLH, people living with HIV; ART, anti-retroviral therapy.
Data collection: Instruments for data collection consisted of records from ART card held by each participant (bearing ART information and laboratory investigation results), pill-count in ART-pill bottle on the day of interview and field tested semi-structured one-on-one interview schedule. The interview schedule was constructed to capture different forms of self-reported lapses in ART adherence and included subjective reporting of ‘ever discontinuing HIV medicines’, ‘ever missing whole day's medication’ and ‘number of missed tablets in the last week’. Inquiry on treatment lapse in the last week helped comparing subjective adherence assessment with objective measure obtained through pill count. Information was also collected on socio-demography, reasons for discontinuing ART medication (if applicable) and exposure variables. The interview schedule was considered by us to have logical validity13 and did not include items culturally inappropriate for their administration in the State of West Bengal.
Measures: Measure of adherence to ART was the outcome variable. We used pill count1415 to categorize our study population in two outcome groups namely ‘well adherent’ and ‘poorly adherent’. Information was collected from ART card in possession of each of the study participants on ‘number of ART pills to be taken by an individual per day’, ‘date of last visit to ART centre’, ‘total number of pills provided by the centre during the last visit’ and ‘number of leftover pills from the previous month’. It was also recorded if leftover pills from the previous month were ‘returned to ART centre’ or ‘kept and used by the respective PLH’, which had implication for calculating adherence. The pills remaining in the box on the day of interview were counted to arrive at an objective measure of adherence.
Adherence for each participant was calculated as follows:
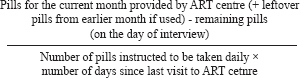
The measure thus calculated was multiplied by 100 to express adherence in percentage. Based on the above calculation, each study participant was identified as either poorly adherent (when adherence < 90%) or well adherent (when adherence ≥90%). We also applied stringent criteria of 95% cut-off to regroup our study participants as poorly adherent (adherence <95%) and well adherent (adherence ≥95%) to examine if such change had ushered different implications.
Definitions of exposure variables: Exposure variables tested for their association with the study outcome (adherence to ART), were selected a priori. Five domains namely (i) illness and treatment issues, (ii) substance use, (iii) exposure to media spreading awareness on HIV disease and treatment, (iv) supportive family environment, and (v) difficult mental status, were studied. While illness under the domain ‘illness and treatment issues’ was characterized by CD4 count during initiation of ART (reflecting immune deterioration), ‘treatment issues’ encompassed ‘duration of ART intake’ (recorded from ART card), ‘attitude of health care providers (perceived by people on ART)’, and ‘time spent to reach ART centre (as reported)’. Monthly supply of ART was collected by PLH from the respective government ART centres. Substance use was defined as self-reported current practice of alcohol intake, oral drug use, cannabis smoking and injecting synthetic pharmaceutical pain killers for non-medical purpose; no scale to assess substance dependence was used.
‘Exposure to media’ was defined as listening to radio and/or watching television. This issue was explored as HIV prevention and treatment messages constitute part of the radio and television programmes in West Bengal. Print media was not part of our investigation as the study population came from a background with low formal education. Self-reported ‘disclosure of HIV status to family member/s’ and ‘satisfaction with care received from family when ill’ were considered as markers of ‘supportive family environment’. As estimated measure of adherence was pertinent to the last one month period, questions on mental status were also framed on similar line. ‘Unwillingness to mix (socially) with others’, ‘sleep disturbance’, ‘inability to relax fully due to restlessness’ and ‘ominous thoughts that something bad would happen’ within the last one month were the issues explored in this regard.
Sample size and analyses: Sample size for the present assessment was calculated to identify 67 per cent ‘well adherent’ adults (assumption based on an earlier study conducted in India)3 with a relative precision of 10 per cent, which meant 132 PLH on ART would be required for interviews. This was derived by using the formula n= Z2 (1-α/2) (1-p)/d2p, where ‘n’ is required sample size, ‘p’ denotes prevalence of the occurrence being investigated (people well adherent to ART in the present study), ‘Z(1-α/2)’ is 1.64 for 90% confidence level and ‘d’ stands for relative precision. We fell a little short of the calculated sample size and could finally study 128 PLH on ART. A post-hoc calculation after this shortfall indicated that the power of the study remained at 80 per cent. Study participants were interviewed on the same day as recruitment and information on outcome as well as exposure variables was collected. Following completion of interviews proportion of well adherent individuals was calculated.
Subsequently, to explore the factors associated with adherence, univariate analyses were conducted comparing ‘poorly adherent’ group as cases and ‘well adherent’ group as control (binary outcome). In line with the suggestion by Katz16, we reported 90 % confidence interval for odds ratios in this study. Independent variables found associated in univariate analyses (at P=0.1) with outcome of interest (90 and 95% adherence to ART) were entered into multivariate logistic regression model. Due to smaller than required sample size theoretical considerations and measurement constraints were used to guide us in selecting variables16 for multivariate logistic regression. For example, although self reported ‘sleep disturbance’ or ‘ominous thoughts that something bad would happen’ could have been entered in multivariate model based on statistical consideration, we did not do so as these symptoms were not checked against psychological assessment for acute or chronic mental illness. Uniformity of findings at two adherence cut-offs (90 and 95%) was another consideration in this regard. All independent variables were entered simultaneously at the time of building multivariate model. SPSS version 11.0 (SPSS, Inc., USA) was used for analyses.
Results
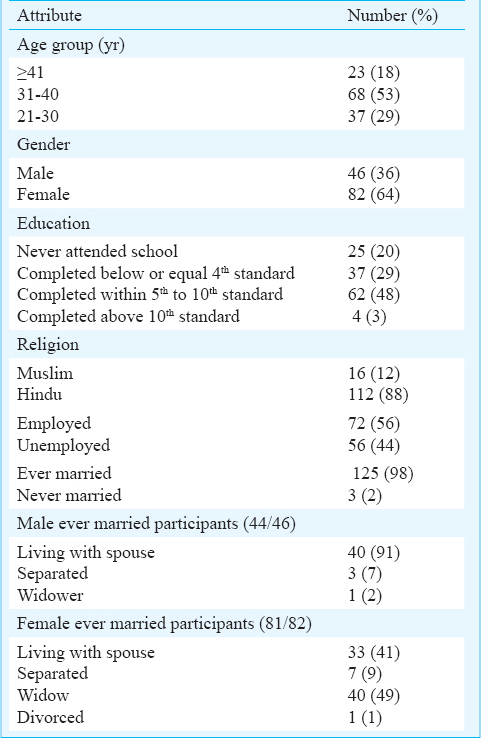
Socio-demographic characteristics: Of the 128 participants, 36 per cent (46/128) were males; mean age of males (38 ± 6 yr; range 28-53 yr) was significantly higher compared to that of females (33 ± 5 yr; range 21-46 yr; P<0.001). One fifth of the study participants (25/128) had never attended school (Table I). Compared to female participants (40/82; 49%), a significantly higher proportion of males (32/46; 70%; P<0.05) had some income generating occupation. Commonly cited occupations by males and females, respectively were daily wage labour (8/32; 25% and 15/40; 38%), petty businesses (5/32; 16% and 8/40; 20%), and agricultural work (4/32; 13% and 5/40; 13%). A tenth of males were engaged in gold or silver thread work on garments and a similar proportion of females reportedly worked as domestic help in various families. The mean monthly income of males was  2278 (minimum 300 and maximum 6500) and that of females was 1343 (minimum 100 and maximum 5000). None reported using cannabis. Injecting synthetic pharmaceutical or oral intake of drugs for non-medical purpose was also not reported. Majority of the study population (127/128; 99%) were on neucleoside reverse transcriptase inhibitors (NRTI) and non-NRTI combinations.
2278 (minimum 300 and maximum 6500) and that of females was 1343 (minimum 100 and maximum 5000). None reported using cannabis. Injecting synthetic pharmaceutical or oral intake of drugs for non-medical purpose was also not reported. Majority of the study population (127/128; 99%) were on neucleoside reverse transcriptase inhibitors (NRTI) and non-NRTI combinations.
Univariate & multivariate analyses: Based on pill count and 90 per cent adherence cut-off, 77 per cent (99/128) of the study participants belonged to well adherent category and the remaining 29 (23%) were poorly adherent. Poor adherence was significantly associated with four factors in univariate analyses (Table II); ‘being in 7th to 12th month of ART intake’ (OR 10.5; 90% CI 2.2 – 49.2; P=0.01), ‘exposure to media (does not listen to radio/nor watches TV)’ (OR 2.5; 90% CI 1.2 – 5; P=0.03), ‘non-disclosure of HIV status to family members’ (OR 4.9; 90% CI 1.7 – 14.2; P=0.01) and ‘incessant thinking during the last one month that something bad would happen (ominous thoughts)’ (OR 2.6; 90% CI 1.3 – 5.2; P=0.02). When 95 per cent cut-off criteria for adherence was applied, 73 per cent (93/128) of the study participants were in ‘well adherent’ category and the remaining 35 (27%) were grouped as ‘poorly adherent’. Univariate analyses following such categorization revealed almost similar association with independent variables as with 90 per cent cut-off (Table II).
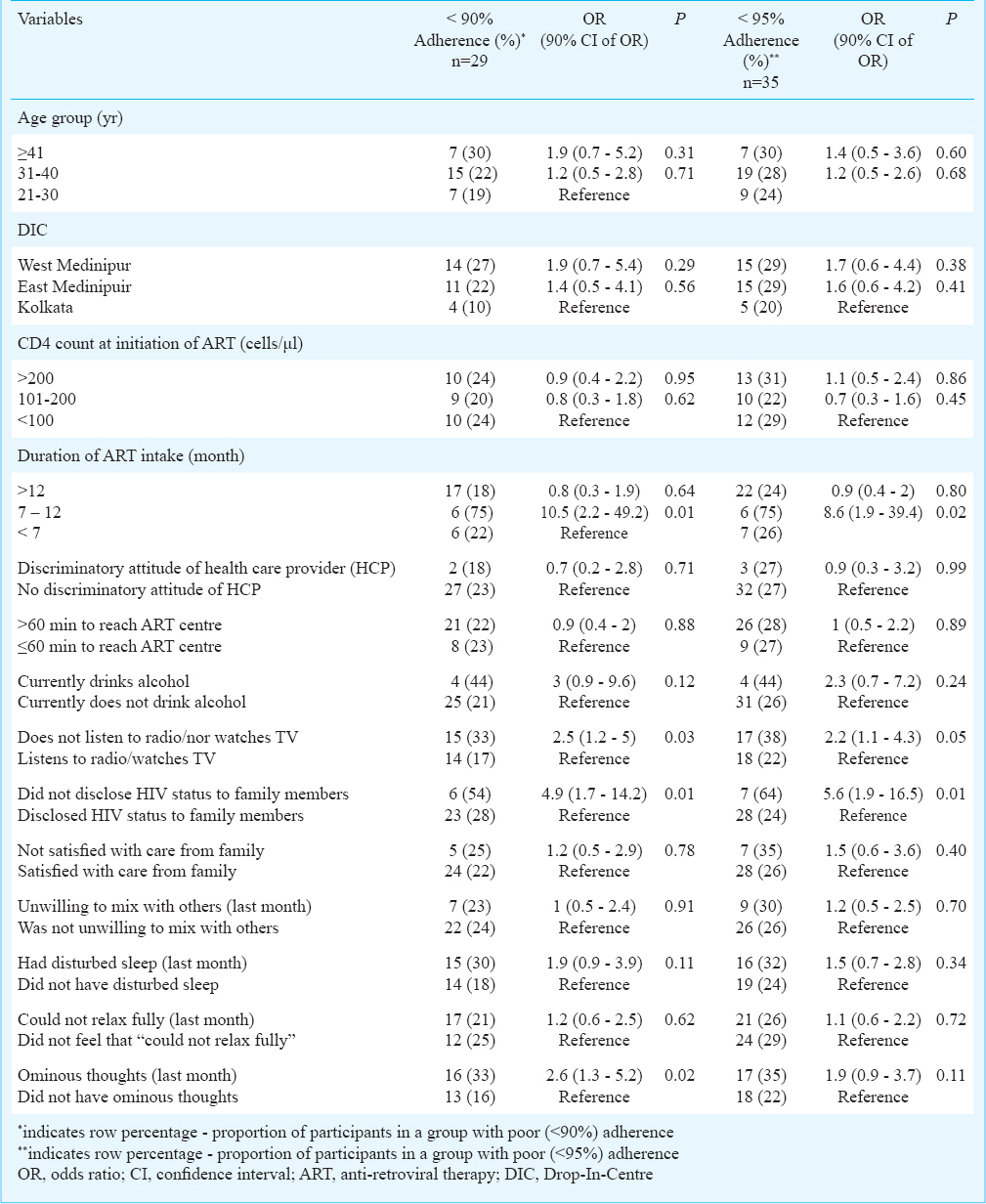
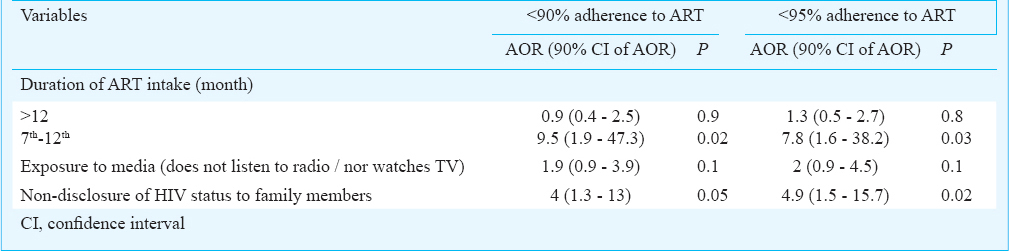
In multivariate model, after adjusting for ‘duration of ART intake’, ‘exposure to media’ and ‘disclosure of HIV status to family members’ (Table III), ‘being in 7th to 12th month period on ART’ had nine times the odds (adjusted OR=9.5; 90% CI 1.9 – 47.3; P=0.02) and ‘non-disclosure of HIV status to family members’ had four times the odds (adjusted OR=4; 90% CI 1.3 – 13; P=0.05) of being associated with poor adherence (<90%). Factors, independently associated in multivariate analyses with <95 per cent adherence to ART were similar (Table III) to what was found when a lower cut-off was used.
Subjective measure of adherence & difficulties faced: As per self-report, 71 per cent (91/128) of the study participants never missed HIV medication since initiation of ART and only 3 per cent (4/128) ever missed whole day's medication.
Self-reported adherence within the recent past (pertaining to last week) revealed a contrasting picture compared to adherence measure estimated through pill count. Among all the participants, 110 were on ‘two tablets a day’ (two tablets of stavudine, lamivudine, nevirapine combination), 17 on ‘3 tablets a day’ (two tablets of stavudine, lamivudine combination and one tablet of efavirenz) and one on ‘7 tablets a day’ (two tablets of zidovudine, 4 tablets of ritonavir, lopinavir combination and single tablet of tenofovir, lamivudine combination). While the PLH on seven tablets a day reported missing whole day's medication once in the last week, 12 of those who were on ‘3 tablets a day regimen’ reported no missed tablet; two individuals in this group reported missing two tablets each and three reported missing one tablet each. Of those 110, who were on two tablets a day regimen, only 2 per cent had reported <90 per cent adherence (2/110 - each missing two pills) and 7 per cent had <95 per cent adherence in the last one week (2/110 - each missing two pills and 6/110 - each missing one pill) – which was low compared to pill count based measure of adherence for the last one month (23 and 27%, respectively).
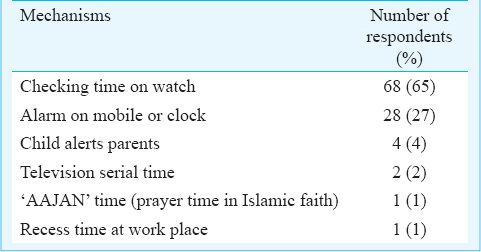
On further inquiring if the participants had ever discontinued taking anti-HIV medicines, 15 per cent (19/128) reported doing so. Some of the reasons cited for discontinuation were ‘financial problem’ (6/19), ‘experimenting with pill holiday’ (1/19), ‘physical problems such as skin rash, vomiting, anaemia or abdominal pain’ (6/19), ‘not attaching importance to regular intake of ART’ (1/19) and ‘forgetfulness’ (5/19). One hundred and four study participants took resort to some form of reminder mechanism for timely intake of anti-retroviral (ARV) medicines (Table IV). In response to queries on difficulties faced, some of the participants reported ‘occasional bad behaviour from health care workers’, ‘ART medicine stock-out’, ‘lack of free bed when needed for admission in hospital’ and ‘non-availability of medicines at hospital for treating opportunistic infections’.
Discussion
The present assessment measured ART adherence among adults in three districts of West Bengal. Till recently no such data were available from this eastern Indian State. Pill count revealed that 73 and 77 per cent PLH, respectively had ≥95 and ≥90 per cent adherence to ART. Conversely, subjective reporting on adherence pertaining to last one week recorded higher proportion of PLH as well adherent. Factors, independently associated with poor adherence were ‘duration of ART intake’ and ‘non-disclosure of HIV status to family members’. These study findings provide direction for future intervention development. Although challenges involved in scaling up ART facilities in India have been acknowledged by programme authorities, yet discussions have been restricted to operational constraints, with little considerations for how local health system responses to HIV/AIDS influence the delivery of ART17.
One of the limitations of the present study was recruitment of participants from client-base of single community based organization (CBO). Engaging other CBOs might have presented a different picture. Secondly, only 54 per cent of eligible clients on ART took part in the study that might have contributed in self-selection bias. Bias due to social desirability and its effect on pill count has already been mentioned. Despite these limitations, we have been able to identify factors associated with adherence having implication for ongoing ART programme.
The current study, through pill count procedure, estimated 23 per cent study participants to be <90 per cent adherent. Weakness of self-report as a method of measuring adherence is underlined by this finding, as only two per cent individuals reported to have <90 per cent adherence through self-reports. Similar was the finding at higher adherence cut-off. In a summary of literature on concordance of self-report with other measures of medication adherence 37 of the 86 comparisons (43%) were categorized as highly concordant18. However, the authors noted that concordance varied substantially by type of self-report measure and non-self report measure18. Self-report measures, in general, were highly concordant with electronic measures in only 17 per cent of comparisons, whereas these were highly concordant with other types of non-self-report measures in 58 per cent comparisons18. As electronic ‘medication event monitoring system’ (MEMS) might not be available in many resource limited settings, adherence assessment studies should be conducted at regular intervals in line with our approach of engaging community organizations so that ongoing ART programmes could be better informed.
Since all participants received anti-HIV medicines from government-operated ART centres, it was not surprising that the proportion of well adherent PLH in our study was higher compared to the study conducted in 20043 when provision of ART in India was mostly dependent on private financing. A systematic review of Indian studies12 also highlighted that in 50 per cent of the studies, cost of medication was cited as commonest impediment for ART adherence. On the contrary, only five per cent of our study participants reported ever discontinuing ART for financial constraint. The other reasons encountered for discontinuation of anti-HIV medicines were ‘experimenting with pill holiday’, ‘physical problems such as skin rash, vomiting, anaemia, abdominal pain’ and ‘forgetfulness’, which were similar to studies undertaken in other parts of the country891011. It is important to take cognisance of a review article that has critically examined barriers to ART adherence in India19, and proposed a framework comprising ‘predisposing factors’, ‘enabling factors’, and ‘need factors’. This framework could serve as a useful tool to identify problem areas and suggest specific health system strategies for improving adherence.
In the present study different reminder mechanisms used by PLH to remember the time of intake of ARV medicines were also recorded. Health care workers may find these handy during provider-patient consultation. The role of treatment supporters cannot be overemphasized in this context. Those in our study, who did not disclose their HIV status to family members, had almost four times the odds of being poorly-adherent to ART. Evidence from Thailand20 has underscored the need to incorporate close family members, including parents more explicitly in programmes to augment adherence. Suggestions have been made to facilitate their effectiveness as long-term adherence partners by providing them with adequate information, training and resources20. A study from south India has identified older age (≥40 yr), female sex, absence of alcoholism, good family bonding, personal ability to follow treatment needs, having hope in life and absence of past history of psychiatric illness to be independently associated with good adherence21. On the other hand, negative impact of stress, low general health perception, anxiety and depression on adherence to ART have been highlighted by studies from India and other countries2223. We could not specifically explore psychological issues as clinical assessment of psychiatric morbidity was not part of our study. It is important to recognize the deleterious effect of inability of disclosure of one's own HIV status on health24. As stigma reinforces such inabilities25 and environment of discrimination may even discourage individuals to undergo HIV test, it would be beneficial if the community based stigma reduction initiatives constitute an integral part of HIV care agenda. Innovative communication approaches can go a long way in such efforts26.
Finally, poor adherence to ART in our study was associated with ‘being in 7th to 12th month of ART therapy’. A study from south India23 identified increased odds of non-adherence with relatively longer duration of ART intake (more than 24 months). Adherence-counselling should not, therefore, be considered as one-off activity at the beginning of ART-initiation and should be reinforced during latter phases as well at regular intervals. In conclusion, our study may have generalization limited to West Bengal, particularly in southern part of the StateState from where study participants were recruited. The study was also limited by smaller sample size and variations between and within DICs. However, creating an environment where people will be able to disclose their HIV status and in turn seek adherence partners from families and beyond and ongoing adherence-counselling-support appear to be programme issues having relevance in wider context.
Acknowledgment
Authors acknowledge Drs Jayanta Acharya and Anup Ghati of the Rabindra Bharati University for support during conceptualization and implementation of the study, Shri Sambhu Seth, Secretary of SPARSHA for allowing us to execute this study through SPARSHA's community based network of People Living with HIV (PLH) and Ms Saheli Samanta of Library & Information Science Division of NICED for her critical inputs. Funding support provided by SPARSHA for undertaking field work is also acknowledged.
Conflicts of Interest: None.
References
- National AIDS Control Organization (NACO), Department of AIDS Control, Ministry of Health and Family Welfare, Government of India. In: Annual Report 2012-13. New Delhi: NACO; 2013.
- [Google Scholar]
- Adherence to antiretroviral therapy and its effect on survival of HIV-infected individuals in Jharkhand, India. PLoS One. 2013;8:e66860.
- [Google Scholar]
- Adherence to antiretroviral therapy & its determinants among HIV patients in India. Indian J Med Res. 2008;127:28-36.
- [Google Scholar]
- Predicting the impact of antiretroviral in resource-poor settings: preventing HIV infections whilst controlling drug resistance. Curr Drug Targets Infect Disord. 2003;3:345-53.
- [Google Scholar]
- Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133:21-30.
- [Google Scholar]
- Higher rates of viral suppression with nonnucleoside reverse transcriptase inhibitors compared to single protease inhibitors are not explained by better adherence. HIV Clin Trials. 2004;5:278-87.
- [Google Scholar]
- Similar adherence rates favor different virologic outcomes for patients treated with non-nucleoside analogues or protease inhibitors. Clin Infect Dis. 2005;40:158-63.
- [Google Scholar]
- Reasons for non-adherence to anti-retroviral therapy among adult patients receiving free treatment at a tertiary care hospital in Delhi. Indian J Community Med. 2010;35:172-3.
- [Google Scholar]
- Barriers to ART adherence & follow ups among patients attending ART centers in Maharashtra, India. Indian J Med Res. 2011;134:954-9.
- [Google Scholar]
- Adherence to anti-retroviral therapy among HIV patients in Bangalore, India. AIDS Res Ther. 2009;6:7-14.
- [Google Scholar]
- Physician estimate of antiretroviral adherence in India: poor correlation with patient self-report and viral load. AIDS Patient Care STDS. 2010;24:189-95.
- [Google Scholar]
- Adherence to antiretroviral therapy in India: a systematic review and meta-analysis. Indian J Community Med. 2013;38:74-82.
- [Google Scholar]
- Research methods in community medicine: surveys, epidemiological research, programme evaluation, clinical trials. (6th ed). England: John Wiley; 2008.
- [Google Scholar]
- Managing HIV-infected children in a low-resource, public clinic: a comparison of nurse vs. clinical officer practices in ART refill, calculation of adherence and subsequent appointments. J Int AIDS Soc. 2012;15:17432-9.
- [Google Scholar]
- Research Coordinator Orientation, University of Pittsburgh, 2002. Available from: https://www.clinicalresearch.pitt.edu/Content/docs/adherence_calculator.pdf
- [Google Scholar]
- Multivariable analysis: a practical guide for clinicians and public health researchers. (3rd ed). New York: Cambridge University Press; 2011.
- [Google Scholar]
- Health systems’ responses to the roll-out of antiretroviral therapy (ART) in India: a comparison of two HIV high-prevalence settings. AIDS Care. 2010;22(Suppl 1):85-92.
- [Google Scholar]
- The concordance of self-report with other measures of medication adherence: a summary of the literature. Med Care. 2004;42:649-52.
- [Google Scholar]
- The role of parents and family members in ART treatment adherence: evidence from Thailand. Res Aging. 2010;32:19-39.
- [Google Scholar]
- Relationship between social factors and treatment adherence: a study from south India. East J Med. 2011;16:147-52.
- [Google Scholar]
- Anxiety and depression symptoms as risk factors for non-adherence to antiretroviral therapy in Brazil. AIDS Behav. 2010;14:289-99.
- [Google Scholar]
- Predictors of nonadherence to highly active antiretroviral therapy among HIV-infected South Indians in clinical care: implications for developing adherence interventions in resource-limited settings. AIDS Patient Care STDs. 2010;24:795-803.
- [Google Scholar]
- Disclosure of HIV status and sexual orientation independently predicts increased absolute CD4 cell counts over time for psychiatric patients. Psychosom Med. 2007;69:74-80.
- [Google Scholar]
- HIV-related stigma: adapting a theoretical framework for use in India. Soc Sci Med. 2008;67:1225-35.
- [Google Scholar]
- Entertainment-education: a communication strategy for social change. New York: Routledge; 1999.
- [Google Scholar]




