
Translate this page into:
Levels, trends & predictors of infant & child mortality among Scheduled Tribes in rural India
Reprint requests: Dr Arvind Pandey, National Institute of Medical Statistics (ICMR) Ansari Nagar, New Delhi 110 029, India e-mail: arvindpandey@icmr.org.in
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
The level of infant and child mortality is high among Scheduled Tribes particularly those living in rural areas. This study examines levels, trends and socio-demographic factors associated with infant and child mortality among Scheduled Tribes in rural areas.
Methods:
Data from the three rounds of the National Family Health Survey (NFHS) of India from 1992 to 2006 were analysed to assess the levels and trends of infant and child mortality. Univariate and multivariate Cox proportional hazard model were used to understand the socio-economic and demographic factors associated with mortality during 1992–2006.
Results:
Significant change was observed in infant and child mortality over the time period from 1992-2006 among Scheduled Tribes in rural areas. After controlling for other factors, birth interval, household wealth, and region were found to be significantly associated with infant and child mortality. Hazard of infant mortality was highest among births to mothers aged 30 yr or more (HR=1.3, 95% CI=1.1-1.7) as compared with births to the mother's aged 20-29 yr. Hazard of under-five mortality was 42 per cent (95% CI=1.3-1.6) higher among four or more birth order compared with the first birth order. The risk of infant dying was higher among male children (HR = 1.2, 95% CI=1.1-1.4) than among female children while male children were at 30 per cent (HR=0.7, 95% CI=0.6-0.7) less hazard of child mortality than female children. Literate women were at 40 per cent (HR=0.6, 95% CI=0.50-0.76) less hazard of child death than illiterate women.
Interpretation & conclusions:
Mortality differentials by socio-demographic and economic factors were observed over the time period (1992-2006) among Scheduled Tribes (STs) in rural India. Findings support the need to focus on age at first birth and spacing between two births.
Keywords
Child mortality
infant mortality
NFHS
rural
Scheduled Tribe

Social and economic development of a nation is often reflected by the existing infant and child mortality rates. India has made significant strides in reducing both infant mortality (40/1000 live births) and under-five mortality (52/1000 live births) but has been unable to achieve the Millennium Development Goal (MDG) by 20151234. Six States, namely, Kerala, Tamil Nadu, West Bengal, Maharashtra, Punjab and Himachal Pradesh are likely to achieve the goal. However, it appears to be a challenge for the remaining States and Union Territories of India. Socio-economic, maternal health and environmental disparities have been associated with the variations across various States and social groups in India. Among the various social groups infant mortality has been observed to be higher among Scheduled Tribe families than the general population5.
Studies conducted globally and in India suggest associations of sex of the child, mother's exposure to mass media, use of clean cooking fuel, access to a toilet facility, improved/safe drinking water facility, mother's religion and ethnicity, income of the household, birth order, mother's age at birth, birth intervals, availability of professional antenatal and delivery care, full immunization of children, mother's education, and urban-rural residence with infant and child mortality678910. Mosley Chen Framework11 categorizes the above determinants of infant and child mortality into three categories (i) biological factors; (ii) socio-economic factors; and (iii) environmental factors.
Among the socio-economic factors, in India studies have shown that a child born to a Scheduled Tribe family has 19 per cent higher risk of dying in the neonatal period and 45 per cent risk of dying in the post-neonatal period compared with other social classes5. Though similar trends in child mortality have been observed for infant and neonates in both tribal and non tribal populations, there is a disproportionate increase in death among children aged 1-4 yr belonging to the Scheduled Tribes compared with the non-Scheduled Tribes12. These differences may be related to the increased social and health related vulnerabilities of the tribal population. Further examination of the infant mortality among the Scheduled Tribes by place of residence shows the highly disadvantaged position of the children born to mothers belonging to Scheduled Tribes in rural areas compared to urban areas12. In general, there is an increased likelihood of deaths of infants in rural as compared to urban areas, however, with regard to the Scheduled Caste/Tribes population, the risk is exacerbated13.
To improve child survival and ensure proper health, several initiatives and programmes have been undertaken among general as well as vulnerable population including Scheduled Tribes under the National Rural Health Mission (NRHM)141516. Specifically, to minimize the rural urban differentials, a life cycle approach has been adopted by the government16. In view of increased vulnerability of Scheduled Tribes in rural areas, there is a need to examine the factors that are likely to put them at risk in terms of infant and child mortality. The current study examines levels, trends and the demographic, socio-economic and to some extent, the environmental factors associated with infant and child mortality among Scheduled Tribes in rural India over three time periods using the three rounds of the National Family Health Surveys (NFHS).
Material & Methods
Data from three rounds of the National Family Health Surveys (NFHS) conducted during the years 1992-1993, 1998-1999, 2005-2006171819 were used. NFHS provides State and national level information on fertility, family planning, infant and child morbidity and mortality, maternal and reproductive health, nutritional status of women and children, and the quality of health services. Multistage stratified sampling methods were used to create a sample representing individuals from all 29 States of India. To make the estimates representative and comparable across the three survey rounds, appropriate sample weights were used in the analysis. In NFHS, all eligible women aged 15-49 yr were asked to provide information on complete birth history, which included sex, month and year of birth, and survival status for each live birth. The information on age at death was recorded in days for children who had died in the first month of life; in months for children who had died after the first month but before completion of their second birthday, and in years for children who had died at later ages. For children who had died after their second birthday, age at death in months was computed. Detailed information on antenatal, delivery and postnatal care for the births which occurred four years for 1992-1993, three years in 1998-1999 and five years in 2005-2006 preceding the survey to eligible women was collected. The present study was restricted to all live births that occurred three years preceding survey for analysis of infant mortality and ten years preceding survey for child mortality among rural Scheduled Tribe women.
Dependent variables are infant mortality and child mortality. Infant mortality is defined as the probability of dying before the first birthday and child mortality of the probability of dying between the first and fifth birthday.
Independent variables considered were mother's age at the time of child birth (15-19, 20-29, 30+ yr), sex of the child (female/male), birth order (1, 2-3, 4+), birth interval (≤ 24 months, > 24 months); mother's education (illiterate, literate); mother's work status (not working, working at home, working away from home); wealth (poor/rich); full antenatal care (ANC) (No/Yes); safe delivery (No/Yes); region (North, Central, East, Northeast, West, South); sanitation facility (unsafe/safe); cooking fuel (unsafe/safe); drinking water (unsafe/safe).
Wealth: NFHS did not collect information on income. The level of economic status of a woman was assessed computing a composite index of household wealth indicating possession of wealth or assets by the household to which they belonged. We computed the wealth quintile for all the three rounds of the survey separately using the methodology followed in the third round of NFHS. Using the total score, a household was categorized into categories as belonging to poor and rich.
Full ANC: Different rounds of NFHS collected information from women on specific problems they might have had during their pregnancies and whether they received any antenatal check-ups. For analyzing trends, due to availability of limited information in NFHS-1, ‘Full ANC’ was defined as ‘yes’ if the women reported of receiving at least three antenatal check-ups, at least one tetanus toxoid injection and iron and folic acid tablets or syrup.
Sanitation facility: Household having either a flush or pit latrine whether private or shared, were regarded to have ‘safe’ sanitation as opposed to those without any facility (unsafe).
Cooking fuel: The households using liquefied petroleum gas (LPG), electricity, kerosene and biogas were considered as users of low polluting fuels (safe). Those using charcoal, firewood and coal were regarded as users of high polluting fuels (unsafe).
Safe drinking water: Households with access to private or public piped or tap (hand pump) water as well as covered well water were considered to have safe water.
Region of residence: For constructing this variable, NFHS categorization according to the six major geographical locations having more or less similar cultural settings have been used: North (Jammu and Kashmir, Himachal Pradesh, Punjab, Haryana, Rajasthan, Delhi and Uttarakhand), Central (Uttar Pradesh, Madhya Pradesh and Chhattisgarh), East (Bihar, Jharkhand, West Bengal and Odisha), North-East (Arunachal Pradesh, Assam, Manipur, Meghalaya, Mizoram, Nagaland, Sikkim and Tripura), West (Gujarat, Maharashtra and Goa) and South (Andhra Pradesh, Karnataka, Kerala and Tamil Nadu).
Statistical analysis: Univariate and multivariate Cox proportional hazard model was used to examine effects of socio-economic, demographic and environmental factors on risk of infant and under-five mortality. Pooled data of the three rounds of NFHS were used. For this model, we defined dependent variable as time (age of the child) and survival status of child (1 if event has occurred i.e. child died and 0 if child is alive) during period of infant (< 12 months) and child (1 - 4 yr), respectively. Results of the multivariate analyses are presented as hazard ratios (risk of dying). If hazard ratio is > 1 for a predictor variable, it means that the hazard is higher, i.e. increased risk of death and if hazard ratio is < 1, it implies a decreased risk of death. Cox proportional hazard analysis was based on pooled data of 12,340 births in the three years preceding date of survey for infant mortality and 43716 births in ten years preceding the date of survey for child mortality.
Results
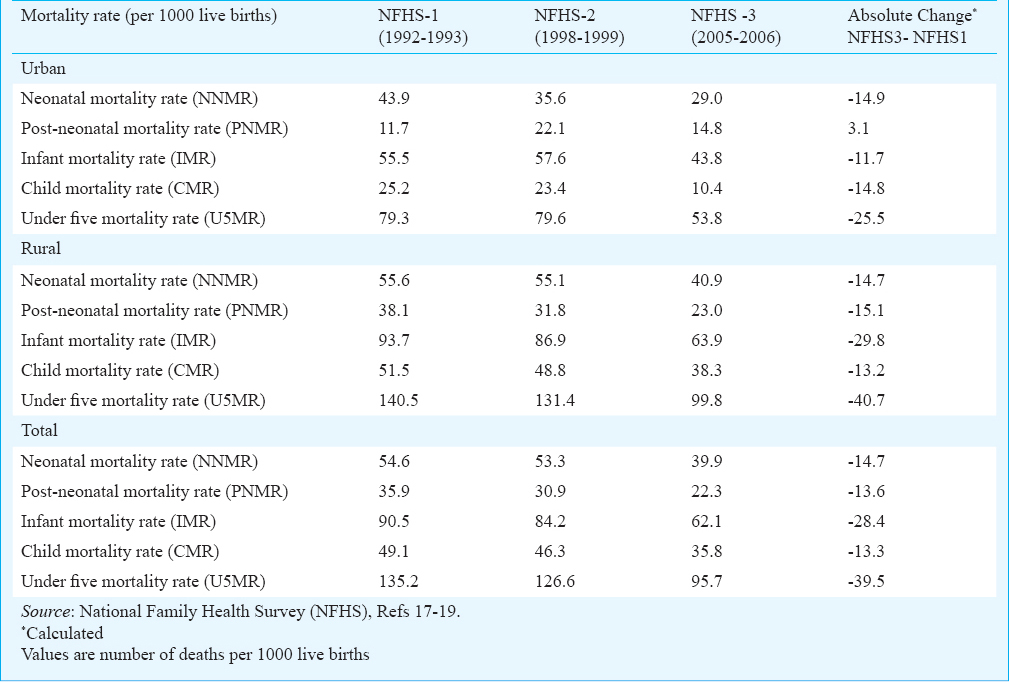
Table I shows the levels and trends of components of under-five mortality i.e. neonatal mortality rate (NNMR), post-neonatal mortality rate (PNMR), infant mortality rate (IMR), child mortality rate (CMR) and under-five mortality rate (U5MR)) according to the place of residence for the three time periods from 1992-1993, 1998-1999 and 2005-2006. Overall, the under-five mortality indicators declined steadily in the past 14 years period (1992-2006) and maximum decline was observed in rural areas. The magnitude of decline varied across components of under-five mortality by residence. During the same period, the under-five mortality rate declined from 135 deaths to 96 deaths per 1000 live births (29% decline) and infant mortality rate declined from 91 deaths to 62 deaths per 1000 live births (32% decline). All the components of under-five mortality were lower in urban areas than in rural areas. Over the past 14 years period from 1992 to 2006, maximum absolute change was observed in under-five mortality rate (41 deaths per 1000 live birth) and the lowest absolute decline for child mortality rate (13 child deaths per 1000 live births). Overall, at the national level the contribution of neonatal mortality to infant mortality increased over time from 60 to 64 per cent and contribution of infant mortality to under-five mortality decreased marginally over time from 67 to 64 per cent. Similar trend was observed in rural areas, but for urban areas, contribution of neonatal mortality to infant mortality decreased from 79 to 66 per cent and contribution of infant mortality to under-five mortality increased from 70 to 81 per cent over time.
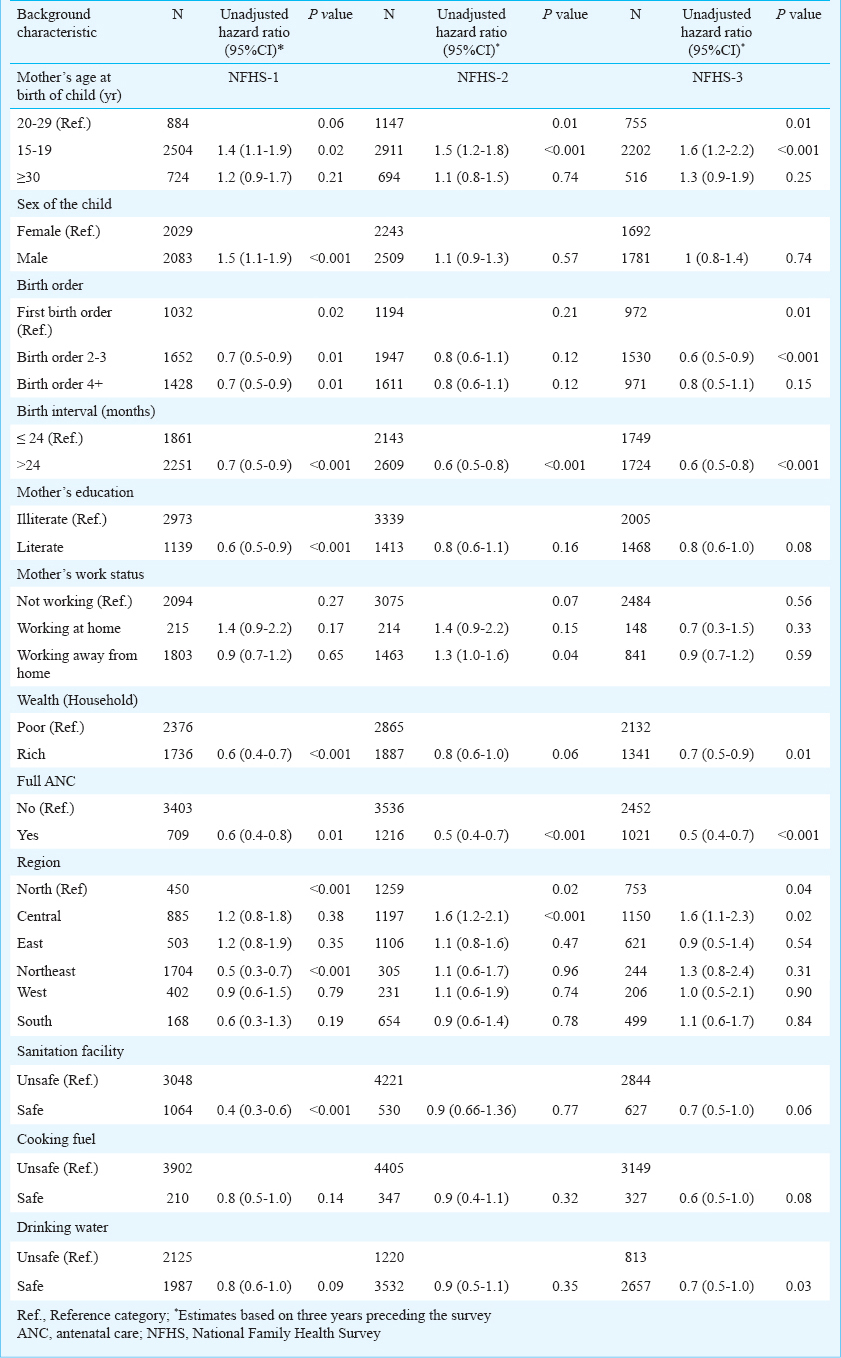
Associations between infant mortality and socio-economic and demographic factors are presented in Table II. The variables, preceding birth interval, full ANC and region were found to be significant for the three periods of NFHS. Sex of the child, birth order, mother's education, wealth status, and sanitation facility were significantly associated with infant mortality in NFHS-1. Birth order, household wealth, and households having safe drinking water facility were found to be significantly associated infant mortality in NFHS-3.
Associations between child mortality and socio-economic and demographic factors are presented in Table III. The variables namely mother's education, household wealth, region and sanitation facility were significantly associated with child mortality across the three time periods. Other significant predictors were birth interval (P<0.001) and safe drinking water facility (P<0.01) in 1992-1993; sex of the child, birth order and cooking fuel in 1998-1999; and mothers age at birth of child (P<0.001) among others in 2005-2006.
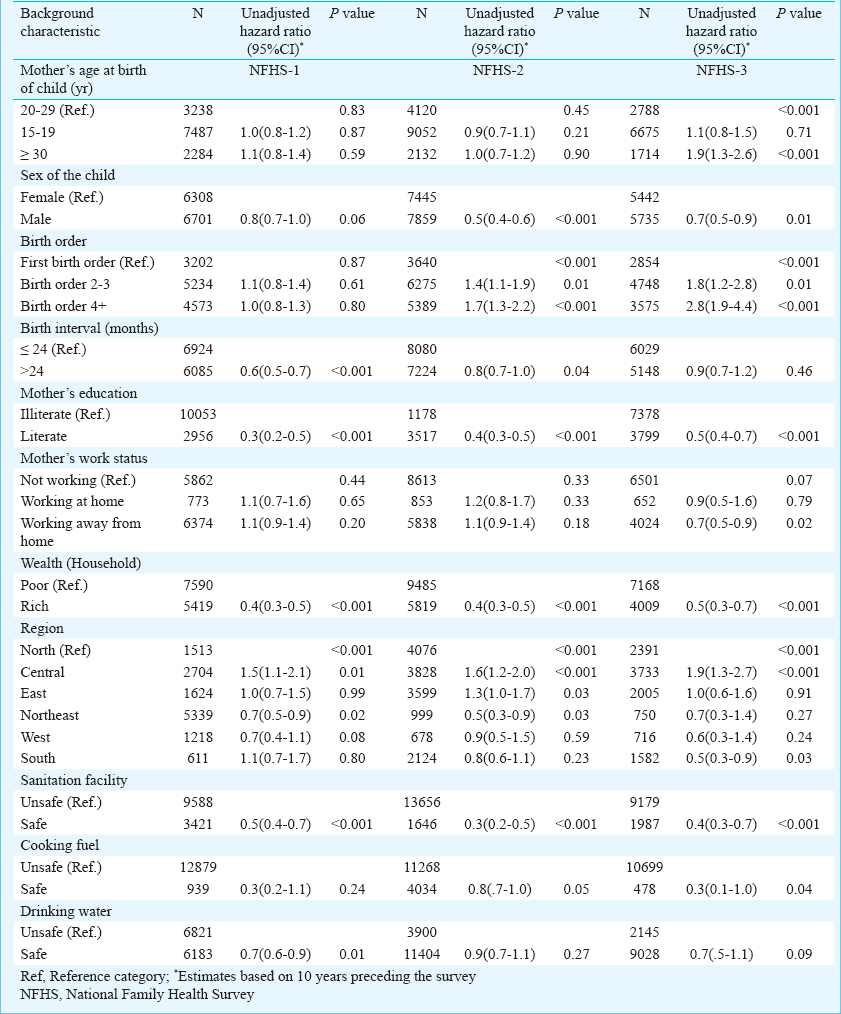
Table IV presents the hazard ratio of the occurrence of infant mortality and child mortality by selected socio-economic and demographic determinants during 1992-2006. Mother's age at child's birth, mother's education, sex of the child, birth order, birth interval, household wealth, full antenatal care (ANC), region, sanitation facility and drinking water were significantly associated with mortality among rural Scheduled Tribes (STs) population.
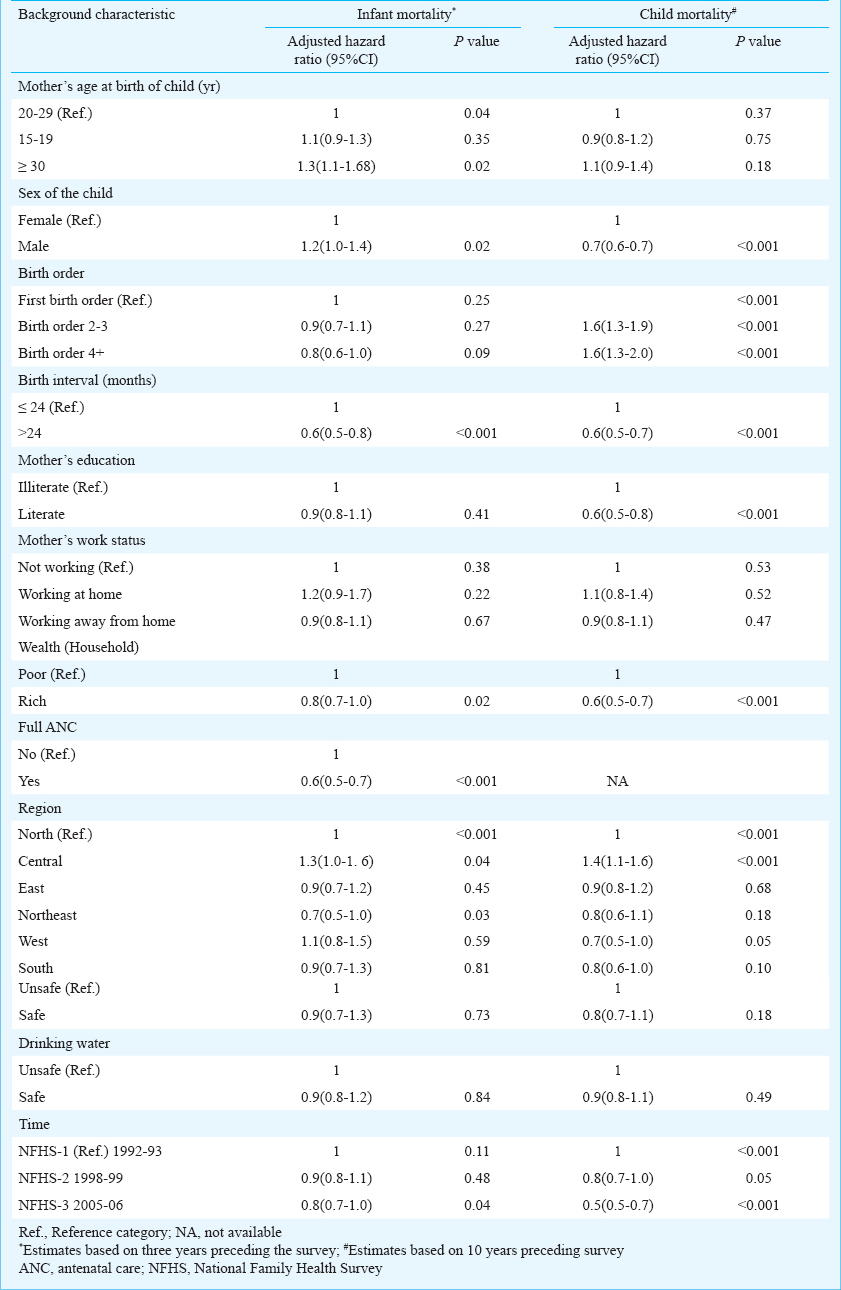
Factors associated with infant mortality (1992-2006): Hazard of infant mortality was highest among births to mothers aged 30 years or more (HR=1.3) as compared with births to the mother's age at child birth 20-29 years after controlling for other social and economic variables. The risk of infant dying was higher among male children (HR = 1.2) than among female children (Table IV). For 1992-1993, babies with birth order four or more had 40 per cent less hazard of death during the infancy period compared with first birth order baby. Results indicated that the children born to mothers with a preceding birth interval of more than 24 months were at less risk of dying than children with a preceding birth interval of 24 months or less. Hazard of infant mortality was 37 per cent less among birth interval of more than 24 months than birth interval of 24 months and less. Result showed that the risk of infant dying was 20 per cent less among rich than poor wealth quintile. The hazard of infant mortality among women who had full antenatal care was estimated at 0.6 which was substantially lower compared to those women who did not receive ANC. Children born to the household having safe cooking fuel were at 70 per cent less hazard of infant mortality than those born to the household having unsafe cooking fuel during 1992-1993. The hazard of infant mortality during 2005-2006 was 20 per cent less compared to the period 1992-1993.
Factors associated with child mortality (1992-2006): Male children had 34 per cent less hazard of child mortality than female children. Higher birth order child were at 60 per cent higher risk of mortality in age group (1-4) years than the first birth order child. Hazard of child death was 40 per cent less among child with a birth interval of more than 24 months than child with a preceding birth interval of 24 months and less. Literate women were at 38 per cent less hazard of child mortality than illiterate women.
Children born to the rich household were at 45 per cent less hazard of child mortality than those born to the poor household. Result showed that the women belonging to west region had 30 per cent less hazard of child mortality than those women belonging to north India. Child from the household having safe sanitation facility had 16 per cent less hazard of child death compared with child from the household having unsafe sanitation facility. During 2005-2006 the hazard of child mortality was 46 per cent less compared to period 1992-1993 followed by 15 per cent during the period 1998-1999 after controlling all predictor variables in the model.
Discussion
Overall, it was observed that all components of under-five mortality viz. neonatal mortality rate, post-neonatal mortality rate, infant mortality rate (IMR) and child mortality rates declined, maximum decline was observed in rural areas than in urban area during the 14-year period (1992-2006) among Scheduled Tribes. The study also indicated at factors that were significantly associated with infant and child mortality among Scheduled Tribes in rural India during 1992-2006. These included mother's age at child birth, sex of the child, birth order, birth interval, household wealth status, and region of residence. The results depicted a U-shaped relationship between infant, and child mortality with mother's age at birth. Similar findings have been observed in general population61020. Increasing impact of low age of mother at birth on mortality could be due to wide gap in utilization of the mother and child health (MCH) care services between younger and older mothers. There is a need for programmes to focus on delaying the age at first birth for younger women in tribal populations in rural areas. Such efforts would not only reduce the infant and child mortality but also help in reducing the morbidity conditions in children under five62122.
Birth order and preceding birth interval of the child are known to be significantly associated with mortality23. Increasing birth order was found to be positively associated with child mortality6. Mortality tends to increase with the birth order. The steady increase in child mortality with the birth order may reflect competition in economically disadvantaged population8. The risk of infant mortality was higher in first order births. However, a study on utilization of maternal health services suggested that higher mortality risk among first order birth could be linked with the early childbearing trends and lower utilization of maternity services in developing countries like India24.
This study showed a higher risk of infant mortality among boys compared with girls in rural India. However, the pattern was reversed with respect to children in the age group of 1-4 yr. The mortality of female child was more compared to male child. Similar findings have been observed in general population and are consistent with other studies2526. Biologically a male child is at higher risk of mortality as reflected by the infant mortality rates, however, the socio-behavioral causes such as gender based discrimination may in part attribute for the higher mortality of a female child. However, since literature suggests gender equitable relationships in tribal population12, further research is required to establish these gender differentials in mortality among tribal population. Our findings showed a positive association of education with child survival. The children of educated mothers have a greater chance of survival, in part because educated women seek out higher quality services and have a greater ability to use healthcare inputs2728.
A considerable poor-rich gap in mortality (during 1992-2006) has emerged from this study. Several studies have reiterated the case of economic inequality and health care access leading threat to the newborns at early age29. Further, the study reconfirmed the regional differences in mortality indicators highlighted by several studies30. Poor health indicators and high mortality in Empowered Action Group (EAG) States have been established as the outcome of poor socio-economic status, demographic stages, low female autonomy, besides the poor health system performance and lower utilization of maternal and child health services30.
The findings of this study should be considered in light of a few data limitations. In order to maintain consistency in the variables across the three rounds of NFHS surveys, data on a few important predictors of infant and child mortality such as anaemia in women or presence of accredited social health activist (ASHA) which were collected in the third round, could not be used in the multivariate analysis.
In conclusion, analysis of under-five mortality over three points of time showed a decline in mortality among rural Scheduled Tribes during 1992-2006 period. The factors associated with mortality remained more or less same over this period. The ongoing national programmes on decreasing infant and child mortality have been focusing on educating women on increasing age at marriage, age at first birth, and increasing the birth interval between two births. In addition to these, our study findings highlight the need for addressing socio-cultural norms towards eliminating gender based discrimination among Scheduled Tribes.
References
- Progress and prospects of millennium development goals in India. Mumbai: International Institute for Population Sciences; 2009.
- [Google Scholar]
- Reducing child mortality in India in the new millennium. Bull World Health Organ. 2000;78:1192-9.
- [Google Scholar]
- National Institute of Medical Statistics (NIMS), Indian Council of Medical Research (ICMR) and United Nations Children's Fund (UNICEF). Infant and child mortality in India: levels, trends and determinants. New Delhi: NIMS (ICMR) and UNICEF India Country Office; 2012.
- [Google Scholar]
- Are too early, too quickly and too many births the high risk births: an analysis of infant mortality in India using National Family Health Survey. Demogr India. 2004;33:127-56.
- [Google Scholar]
- Maternal health care services: observations from Chhattisgarh, Jharkhand and Uttranchal. Econ Pol Wkly. 2004;39:713-20.
- [Google Scholar]
- Further evidence of the effects of preceding birth intervals on neonatal, infant, and under-five-years mortality and nutritional status in developing countries: evidence from the demographic and health surveys. DHS Working Paper No. 41. Calverton, Maryland, USA: Demographic and Health Research Division, Macro International Inc; 2008.
- [Google Scholar]
- Childhood mortality in Rwanda: levels, trends, and differentials; Further analysis of the Rwanda demographic and health surveys, 1992-2007/08. DHS Further Analysis Reports No. 66. Calverton, Maryland, USA: ICF Macro; 2009.
- [Google Scholar]
- Cause-specific neonatal deaths in rural Bangladesh, 1987-2005: levels, trends, and determinants. Popul Stud (Camb). 2014;68:247-63.
- [Google Scholar]
- An analytical framework for the study of child survival in developing countries. Bull World Health Organ. 2003;81:140-5.
- [Google Scholar]
- A closer look at child mortality among Adivasis in India. Policy Research Working Paper 5231. Washington DC: The World Bank, South Asia Region, Human Development Department; 2010.
- [Google Scholar]
- Determinants of infant mortality in rural India: a three-level model. Health. 2013;5:1742-9.
- [Google Scholar]
- Ministry of Health and Family Welfare, Government of India. National Health Mission. Available from: http://nrhm.gov.in
- [Google Scholar]
- UNICEF. India's call to action for child survival and development: a bold step to reaffirm our commitment. 2013. Available from: http://www.unicef.org/india/Resources.pdf
- [Google Scholar]
- Ministry of Health and Family Welfare. Government of India. Components of National Health Mission Schemes. Available from: http://nrhm.gov.in/nrhm-components/rmnch-a/childhealth-immunization/child-health/schemes.html
- [Google Scholar]
- International Institute for Population Sciences (IIPS). National Family Health Survey (NFHS-1), 1992-93. India. Mumbai: IIPS; 1995.
- [Google Scholar]
- nternational Institute for Population Sciences (IIPS), and ORC Macro. 2000. National Family Health Survey (NFHS-2), 1998-99. India. Mumbai: IIPS; 2000.
- [Google Scholar]
- International Institute for Population Sciences (IIPS) and Macro International. 2007. National Family Health Survey (NFHS-3), 2005-2006. India. Mumbai: IIPS; 2007.
- [Google Scholar]
- Reproductive health, and child health and nutrition in India: meeting the challenge. Lancet. 2011;377:332-49.
- [Google Scholar]
- Early marriage and sexual and reproductive health risks: experiences of young women and men in Andhra Pradesh and Madhya Pradesh, India. New Delhi: Population Council; 2008.
- [Google Scholar]
- The effect of maternal child marriage on morbidity and mortality of children under 5 in India: cross sectional study of a nationally representative sample. BMJ. 2010;340:b4258.
- [Google Scholar]
- Birth-spacing, fertility and neonatal mortality in India: dynamics, frailty, and fecundity. J Econom. 2008;143:274-90.
- [Google Scholar]
- Determinants of maternity care services utilization among married adolescents in rural India. PLoS One. 2012;7:e31666.
- [Google Scholar]
- Child mortality estimation: estimating sex differences in childhood mortality since the 1970s. PLoS Med. 2012;9:e1001287.
- [Google Scholar]
- Gender differentials in child mortality in Andhra Pradesh: evidence from National Family Health Survey. Fam Welf. 2001;47:1-11.
- [Google Scholar]
- Effect of WHO newborn care training on neonatal mortality by education. Ambul Pediatr. 2008;8:300-4.
- [Google Scholar]
- Community-based interventions for improving perinatal and neonatal health outcomes in developing countries: a review of the evidence. Pediatrics. 2005;115(Suppl 2):519-617.
- [Google Scholar]
- An integrated scientific framework for child survival and early childhood development. Pediatrics. 2012;129:e460-72.
- [Google Scholar]
- The Million Death Study Collaborators. Causes of neonatal and child mortality in India: a nationally representative mortality survey. Lancet. 2010;376:1853-60.
- [Google Scholar]




