Translate this page into:
Mannose binding lectin (MBL) 2 gene polymorphism & its association with clinical manifestations in systemic lupus erythematosus (SLE) patients from western India
Reprint requests: Dr Anita Nadkarni, National Institute of Immunohaematology (ICMR), 13th Floor, King Edward Memorial Hospital, Parel, Mumbai 400 012, Maharashtra, India e-mail: anitahnadkarni@yahoo.com
-
Received: ,
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Background & objectives:
Systemic lupus erythematosus (SLE) is a prototypical autoimmune disease characterized by production of autoantibodies. Mannose binding lectin (MBL) is an important element of the innate defense system. The present study was undertaken to determine whether variant alleles in MBL2 gene were associated with disease severity in SLE patients.
Methods:
The MBL alleles [-550, -221, +4, Codon 52, Codon 54 and Codon 57] were studied by PCR- RFLP (restriction fragment length polymorphism) method in 100 SLE patients fulfilling ACR (American College of Rheumatology) criteria along with 100 healthy controls. SLE disease activity was evaluated using SLE Disease Activity Index (SLEDAI) score.
Results:
Homozygosity for MBL variant allele (O/O) was observed in 24 per cent of the SLE patients compared to 16 per cent of the normal controls, while no difference was found for heterozygosity (A/O) (37 vs 35%). A significant difference was reported in incidence of double heterozygosity for mutant allele B and D (B/D) among SLE patients as against control group (P = 0.015). MBL genotypes did not show any association with renal involvement.
Interpretation & conclusions:
In this study from western India, MBL gene polymorphism showed an influence as a possible risk factor for susceptibility to SLE, but had no direct effect on disease characteristics. Further studies need to be done on a larger number of SLE patients in different regions of the country.
Keywords
Allele
gene polymorphism
heterozygosity
mannose binding lectin (MBL)
systemic lupus erythematosus (SLE)

Systemic lupus erythematosus (SLE) is a complex trait characterized by the production of a range of autoantibodies and a diverse set of clinical phenotypes1. Wide-ranging clinical phenotypes include skin rash, neuropsychiatric and musculoskeletal symptoms and in some patients leading to lupus nephritis, are observed in SLE patients. Aberrant complement activation leads to inflammation resulting in tissue injury of multiple organs. Mannose binding lectin (MBL) is a calcium-dependent serum protein that plays a role in the innate immune response by binding to carbohydrates on the surface of a wide range of pathogens, where it can activate the complement system or act directly as an opsonin2. The complement system is a collection of blood and cell surface proteins that are involved in primary host defense and act as a clearance components of innate and adaptive immune responses. There are three different complement pathways, the classical complement pathway, the alternative complement pathway, and the mannose-binding lectin (MBL) pathway2. The lectin pathway is stimulated when the MBL binds to mannose residues on the pathogen surface. The MBL-associated serine proteases, MASP-1, and MASP-2, are activated and cleave C4 and C2, which then form the C3 convertase and leads to the formation of membrane attack complex (MAC) which ultimately initiates cell lysis. MBL has an oligomeric structure (400-700 kDa), built of subunits that contain three identical peptide chains of 32 kDa each. Each subunit is characterized by a lectin domain, an α-helical coiled-coil, a hydrophobic neck region, a collagenous region and a cysteine rich N-terminal region34.
MBL2 gene is present on chromosome 10 in the region 10q21-24. The normal structural MBL allele is named A, while the three variant structural alleles namely ‘B’ (codon 54), ‘C’ (codon 57) and ‘D’ (codon 52) are designated as ‘O’allele5. The MBL expression is influenced by the three promoter polymorphic variations at position –550 (H/L), –221 (X/Y) and +4 (P/Q). The promoter and coding variants are in strong linkage disequilibrium which give rise to different haplotypes. Seven such haplotypes (HYPA, LYQA, LYPA, LXPA, HYPD, LYQC and LYPB) linked to MBL2 gene have been defined6.
The aim of the present study was to investigate the role of MBL and its association with susceptibility and clinical expression of SLE through the analysis of promoter region and exonic polymorphism of MBL2 gene.
Material & Methods
This retrospective study was conducted in 100 consecutive SLE patients from Mumbai, western India, collected over a span of three years (January 2010- December 2012). Their age ranged from 5-53 yr (mean ± SD; 28.14 ± 9.99) in females and 7-45 yr (mean ± SD; 25.75 ± 13.76) in males. These patients were referred from Rheumatology and Nephrology departments of KEM hospital, Mumbai, Maharashtra, India, to National Institute of Immunohaematology, (NIIH), Mumbai. All these patients were diagnosed according to the American College of Rheumatology (ACR) criteria7. Disease activity was assessed at the time of evaluation using Systemic Lupus Erythematosus Disease Activity Index (SLEDAI)8. Pregnant and post-menopausal women, smokers, patients with diabetes and patients with significant hyperlipidaemia were excluded. The source of normal controls (n=100) was volunteer blood bank donors and healthy women staff members of the NIIH. Blood samples (5 ml) were collected after obtaining written informed consent from all the individuals. The study protocol was approved by the Institutional Ethical Committee (IEC) of NIIH.
The patients were categorized into two groups, SLE with lupus nephritis (LN) and SLE without lupus nephritis (non LN). Renal biopsies were examined by light microscopy using hematoxylin, eosin, periodic Schiff (PAS) staining. Immunofluorescence microscopy was done using anti-IgG, anti-IgM, anti-IgA, anti-C3, anti-C4 and anti-fibrinogen fluorescein isothiocyanate conjugate (FITC). The renal histology was classified according to WHO criteria9.
Molecular analysis: Genomic DNA was extracted by using conventional phenol-chloroform extraction method10. The genotyping of six single nucleotide polymorphisms (SNPs) in the MBL2 gene was performed as previously described11. The promoter region polymorphism +4 (P/Q) and -550 (H/L) was studied using allele specific oligonucleotide amplification11. Another promoter region polymorphism at -221 (X/Y) and exonic polymorphisms R52H, G54D and G57E were studied by restriction fragment length polymorphism (RFLP) method using the restriction enzyme BsajI, HhaI, BanI, MboII respectively121314. All the PCRs were initiated by 5 min denaturation step at 94°C and completed by 7 min extension step at 72°C.
Statistical analysis: Continuous variables were expressed as mean+SD. Pairs of groups were compared using student ‘t’ test for normally distributed continuous distribution. The ‘χ2 ’ test was used for the categorical variables as needed. Statistical analysis was carried out using Graph Pad In Stat 2 software (Graph Pad Software Inc., USA). Chi-square test, with Yates's correction was used for analysis15.
Results
Among 100 SLE patients included in the study, 92 were females. At the time of evaluation antinuclear antibody (ANA) positivity was 100 per cent and anti-dsDNA (anti-double stranded DNA) positivity was 88.9 per cent. Age at onset of the disease was 4-46 yr (24.7+8.79 yr) and the age at evaluation was 5-53 yr (27.94+10.2 yr). The SLEDAI scores ranged between 6 - 53 (mean + SD; 17.53 + 9.2), the average SLEDAI score of LN patients was higher (20.60 ± 9.93) than non LN patients (12.80 ± 6.97) and overall SLE patients (16.94 ± 9.47). The disease severity of the patients was categorized into mild, moderate and severe based on their SLEDAI scores (mild<8, moderate 8-18, severe >18). Moderate disease severity was noted in 52 per cent of SLE patients, while 35 and 13 per cent patients had severe and mild disease, respectively.
Table I shows the distribution of MBL2 structural gene polymorphisms in SLE patients among LN and non LN groups as compared with healthy controls. It was observed that 39 per cent of SLE patients showed A/A genotype, 37 per cent had A/O genotype and 24 per cent had O/O genotype. Overall distribution did not differ significantly between SLE patients and controls. However, increased frequency of O/O homozygosity was observed among SLE patients when compared to controls. Similar tendency for loss of wild type allele was noted higher in LN patients as against non LN group. The total frequency of ‘O’ alleles was 0.4 in patients and 0.3 in the controls. The double heterozygosity for B/D allele was significantly higher in SLE patients (62.5%) as against control group (25%). [OR 3.973, CI (1.3-12.19), P= 0.015]. The frequency of promoter variants and position +4 is shown in Table II. There was no significant difference reported between SLE and control group. Only -550 region allele ‘L’ was found to be significantly higher among LN patients as compared to non LN group (P=0.004). MBL down-regulating promoter allele ‘X’ did not contribute to SLE susceptibility in our study.
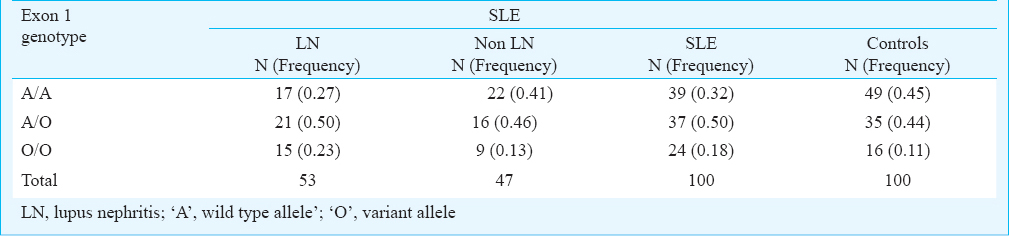
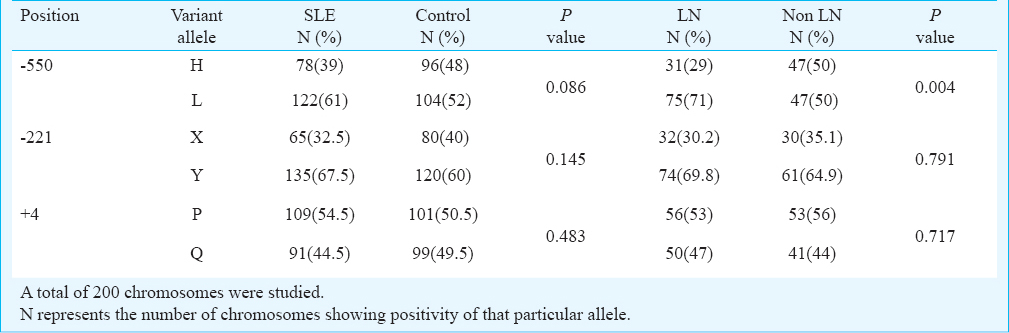
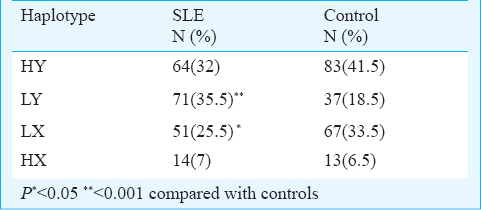
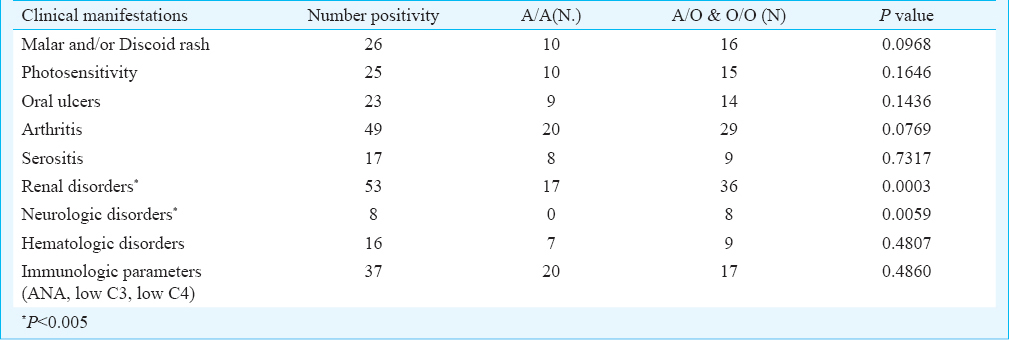
Table III shows frequency of promoter haplotypes between SLE patients and controls. Significant difference was reported in the frequency of LY haplotype between SLE patients and controls [OR – 4.1687, CI - 2.30-7.54), P=0.0001]. Similarly, LX haplotype that leads to lower MBL levels also showed significant difference between SLE patients and control group (P=0.03). Table IV summarizes details of clinical manifestations and MBL genotypes. Approximately 50 per cent of the SLE patients showed renal involvement and arthritis, followed by 37 per cent of the patients showed positivity with immunological parameters like ANA, low C3-C4 levels and 26 per cent showed the presence of malar and/or discoid rash. Significantly higher prevalence of variant allele was reported in SLE patients having renal involvement (P<0.001) and neurological disorders (P<0.05). Histological subtypes of lupus nephritis (like MPGN, FPGN, DPGN and RPGN) were studied, but they did not exhibit any notable difference and there were no significant difference found (results not shown).
The regulatory and coding variants are in strong linkage disequilibrium; with seven most common haplotypes described HYPA, LYPA, LYQA, LXPA, HYPD, LYPB and LYQC. The distribution of seven common haplotypes was studied among SLE patients and control group. All seven haplotypes were equally distributed among patients and control group. There was no linkage association of any haplotype noted with disease severity. The haplotype LYPA (48%), LYQA (46%) and HYPA (41%) showed the highest prevalence among study population.
Discussion
It has been shown that MBL2 gene polymorphisms influence susceptibility to SLE and could be associated with some clinical and laboratory features, disease progression, cardiovascular disease and increased risk of infection16. Many groups have previously investigated the possibility of interaction among SLE candidate genes. Multiple genes are known to be involved in susceptibility of SLE17. Several studies have shown MBL gene variation at exon 1 as being additive risk factor for susceptibility in different populations18192021. In our study, slightly increased frequency of exonic variant allele was observed among SLE patients when compared to controls. The overall frequency for MBL structural mutant alleles in exon 1 region did not differ significantly between SLE and control groups but there was a decreased tendency of wild type allele ‘A’ in SLE patients. Similar findings have been reported by Asgharzadeh et al11 in their study on MBL2 gene polymorphism, susceptibility to renal dysfunction among SLE patients. Another study on white Danish population has demonstrated that complicating infections in SLE patients are strongly associated with homozygosity (O/O) for MBL variant allele5. In our study also, the variant allele ‘O’ contributed significantly in infections.
A recent study carried out in the eastern India showed higher frequency of B/B genotype in SLE patients as compared to healthy controls22. In our study from western India higher frequency of B/D genotype was observed in SLE patients. A meta-analysis involving studies with three ethnic populations namely European derived, African derived and Asian derived concluded that allele ‘B’ and the allelic variant at promoter region of MBL2 gene, specifically those found at position -550 and -221 were risk factors for SLE development23. In our study the promoter variant analysis did not show any difference among SLE patients and control group except that -550 region allele ‘L’ was found to be significantly higher among LN patients as compared to non LN group. Another meta-analysis by Xu et al24 of five European and three American studies indicated a significant association between the polymorphism and SLE in allelic contrast. While stratified by ethnicity in European population, no significant association was found, therefore, they concluded that the MBL2 A/O polymorphism might be associated with SLE24. In our study, non significant association of MBL2 A/O polymorphism with susceptibility to SLE was observed.
Glesse et al26 observed a significant difference among the frequency of both promoter haplotype and haplotypic combination in African derived patients, with a higher incidence of HY haplotype and LY/HY combinations in SLE patients when compared with controls. The studies among Americans, Caucasians and Chinese have shown complete absence of HX haplotype showing complete linkage disequilibrium between alleles H/L and X/Y27. We observed equal frequency of HX haplotype among our SLE patients and control group. Similar results have been reported by Navarra et al28 among Filipinos population showing higher frequency of HX alleles (SLE - 22.41%, control - 25.4%) suggesting genetic diversity. The regulatory and coding variants are in strong linkage disequilibrium; only seven haplotypes have been so far reported in human population and, therefore, thought to be resulted due to founder mutational events. The haplotype HYPA was reported to be associated with wild type allele ‘A’ showing higher MBL levels, whereas haplotype LXPA was associated with most severe defects29. In our study, we did not find such associations as both the haplotype HYPA and LXPA showed nearly equal distribution among SLE patients and controls.
In conclusion, our study indicated that frequency of double heterozygosity for B/D allele was increased in SLE patients as compared to normal healthy individuals. Similarly, allele ‘L’ of the -550 region in the promoter site showed susceptibility for renal involvement suggesting that these alleles could be an important risk factor for SLE development in our population. LX haplotype that leads to lower MBL levels might have contributed to disease susceptibility in our SLE patients from western India. Thus, the overall effect and role of associated risk factors may vary according to the ethnic and genetic background of the study population.
Acknowledgment
Authors acknowledge the Department of Biotechnology (DBT), Government of India, New Delhi, for the financial support.
References
- Autoantibodies in systemic lupus erythematosus: comparison of historical and current assessment of seropositivity. Lupus. 2011;20:250-5.
- [Google Scholar]
- The role of complement in the development of systemic lupus erythematosus. Annu Rev Immunol. 2004;22:431-56.
- [Google Scholar]
- Mannose binding lectin (MBL) in autoimmunity and its role in systemic lupus erythematosus (SLE) J Assoc Physicians India. 2010;58:688-90.
- [Google Scholar]
- The role of mannose-binding lectin in systemic lupus erythematosus. Clin Rheumatol. 2008;27:413-9.
- [Google Scholar]
- Mannose-binding lectin polymorphisms and susceptibility to infection in systemic lupus erythematosus. Arthritis Rheum. 1999;42:2145-52.
- [Google Scholar]
- Human mannose-bonding lectin in immunity: friend, foe or both? J Exp Med. 2004;199:1295-9.
- [Google Scholar]
- Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997;40:1725.
- [Google Scholar]
- Derivation of SLEDAI: a disease activity index for lupus patients. The Committee on Prognosis Studies in SLE. Arthritis Rheum. 1992;35:630-40.
- [Google Scholar]
- The classification of glomerulonephritis in systemic lupus erythematosus revisited. J Am Soc Nephrol. 2004;15:241-50.
- [Google Scholar]
- Protocol adapted from short protocols in molecular biology. (3rd ed). New York: John Wiley; 1995. p. :2-3. Unit 2.1
- [Google Scholar]
- Mannose-binding lectin gene and promoter polymorphism and susceptibility to renal dysfunction in systemic lupus erythematosus. J Biol Sci. 2007;7:801-5.
- [Google Scholar]
- PCR-restriction fragment length polymorphism method to detect the X/Y polymorphism in the promoter site of the mannose binding lectin gene. Clin Chem. 2003;49:1557-8.
- [Google Scholar]
- Association of mannose-binding lectin gene polymorphism but not of mannose serine protease 2 with chronic severe aortic regurgitation of rheumatic etiology. Clin Vaccine Immunol. 2008;15:932-6.
- [Google Scholar]
- Might there be a link between mannose binding lectin and vitiligo. Eur J Dermatol. 2007;17:146-8.
- [Google Scholar]
- On estimating the relation between blood group and disease. Ann Hum Genet. 1955;19:251-3.
- [Google Scholar]
- The role of mannose-binding lectin in systemic lupus erythematosus. Clin Rheumatol. 2008;27:413-9.
- [Google Scholar]
- Analysis of polymorphisms affecting immune complex handling in systemic lupus erythematosus. Rheumatology (Oxford). 2003;42:446-52.
- [Google Scholar]
- Association of functional mutant homozygotes of the mannose binding protein gene with susceptibility to pulmonary tuberculosis in India. Tuber Lung Dis. 1999;79:221-7.
- [Google Scholar]
- Role of mannose binding lectin gene variants on its protein levels and macrophages phagocytosis with live mycobacterium tuberculosis in pulmonary tuberculosis. FEMS Immunol Med Microbiol. 2006;46:433-7.
- [Google Scholar]
- Association of mannose-binding lectin gene polymorphism with tuberculosis susceptibility and sputum conversion time. Int J Immunogenet. 2012;39:10-4.
- [Google Scholar]
- Association of SP-D, MBL, I-NOS genetic variants with pulmonary tuberculosis. Indian J Hum Genet. 2006;12:105-10.
- [Google Scholar]
- Low producer MBL genotypes are associated with susceptibility to systemic lupus erythematosus in Odisha, India. Hum Immunol. 2013;74:114-9.
- [Google Scholar]
- The mannose-binding lectin gene polymorphisms and systemic lupus erythematosus; two case-control studies and a meta-analysis. Arthritis Rheum. 2005;52:3966-74.
- [Google Scholar]
- Association of RANTES and MBL gene polymorphisms with systemic lupus erythematosus: a meta analysis. Mol Biol Rep. 2013;40:941-8.
- [Google Scholar]
- Association of systemic lupus erythematosus with promoter polymorphisms of the mamose-binding lectin gene. Arthritis Rheum. 1998;41:1663-8.
- [Google Scholar]
- Association of mannose-binding lectin 2 gene polymorphic variants with susceptibility and clinical progression in systemic lupus erythematosus. Clin Exp Rheumatol. 2011;29:983-90.
- [Google Scholar]
- On the haplotypic frequencies of the MBL2 gene among human populations. Lupus. 2007;16:838.
- [Google Scholar]
- Increased frequency of mannose-binding lectin promoter LX haplotype among Filipinos with systemic lupus erythematosus. Lupus. 2007;16:147-8.
- [Google Scholar]
- Interplay between promoter and structural gene variants control based serum level of mannan-binding protein. J Immunol. 1995;155:3013-20.
- [Google Scholar]




