Translate this page into:
Mesenchymal stromal cells as regulators of anti-tumour immune response
This editorial is brought out on the occasion of World Cancer Day - February 4, 2015.
*For correspondence: alessandro.poggi@hsanmartino.it
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
In India, breast and cervix uteri cancers are two of the leading causes of neoplasia for women, while neoplasia of lung and gastroenteric tract are a cause of mortality in men. It appears that lifestyle, exposition to carcinogenic substances and diet can greatly influence the incidence of cancer123. Data reported from several agencies should be carefully analyzed as several confounding elements can be present. India is a vast country with diverse cultures, habits, and living conditions and the Population Based Cancer Registries cover a small percentage of the total population leaving several States uncovered123. Besides the conventional therapy targeted molecular therapies are becoming popular for treatment of neoplasia. These therapies hit neoplasia focusing on an essential biochemical pathway blocking mainly phosphokinases with specific inhibitors or targeting tumour cells with humanized monoclonal antibodies. Usually, monoclonal antibodies interfere with soluble growth factors or trigger complement and cellular dependent tumour cytotoxicity45. In addition, it is becoming more prominent to use antibodies which favour autoimmune reactivity by relieving the brake of host immune system678. Further, it is also relevant to point out that the infiltration of neoplasia as breast and gastrointestinal tract cancer with lymphocytes could identify patients with a better outcome910. Thus, a therapy which favours the anti-tumour immune response could be an additional weapon against cancer. The carcinoma microenvironment is composed of different subsets of inflammatory leukocytes, fibrocytes, tumour infiltrating lymphocytes (TIL), blood and lymphatic vessels and several types of mesenchymal stromal cells (MSCs) as fibroblasts which produce and secrete extracellular matrix components (EMC)11. The MSCs can influence their surroundings producing EMC and soluble factors playing a role in survival, proliferation, epithelial mesenchymal transition (EMT) and metastasis of carcinoma stem cells1112. Furthermore, MSC can regulate both innate and adaptive immune cell response1314. It is becoming evident that MSCs play a key role in the development of the carcinoma11. The focus here will be on the use of drugs to regulate MSC-mediated activities together with the analysis of the more recent findings regarding the immunosuppressive role of MSCs.
MSCs as carcinoma associated fibroblasts (CAF): MSCs are fibroblast-like cells with a fuse shaped morphology which can produce and secrete several EMC such as collagen, fibronectin, laminin, heparin sulphate, proteoglycans, and can differentiate in specialized stromal cells which produce mainly a few kinds of EMC11. Fibroblasts-like cells located at the carcinoma site are usually named carcinoma associated fibroblasts (CAF)12. Their phenotypic characterization is based on the expression of a combination of markers, such as CD105, CD73, CD90 and CD146 rather than the presence of a peculiar surface11. Within the tumour, some epithelial cells can undergo epithelial-mesenchymal transition (EMT) and MSC can assume some epithelial characteristics11. A key role in the interaction between CAF and tumour cells is played by transforming growth factor (TGF)β15. It has been shown that TGFβ can have opposite effects on tumour cells, depending on the stage of the tumour and can act as either a tumour promoter or a tumour suppressor15. TGFβ has also important effects on the immune cells present and/or recruited within the tumour site16. It inhibits the cytotoxic programme in natural killer (NK) cells and T lymphocytes through transcriptional repression of genes encoding perforins, granzymes and cytotoxic factors16. It is of note that MSCs can produce and secrete TGFβ and thus these cells can play a role both in EMT transition and in regulation of anti-tumour immune response.
MSC-dependent regulation of immune response in solid tumours and relevance of tumour infiltrating lymphocytes: MSCs present within a carcinoma can regulate immune response in several ways. Many inhibiting factors responsible for the MSC-mediated downregulation of effect or lymphocyte activation (Figure) have been identified including TGFβ, IL10 and prostaglandin E2, indoleamine 2,3 dioxigenase, heme oxigenase, arginase 1 and 2, nitric oxidase synthase 2, hepatocyte growth factor and peculiar histocompatibility antigens such as HLAG51314. Thus, it is conceivable that targeting of CAF-derived immunosuppressive factors can be a tool to favour anti-tumour immune response. Recently, it has been claimed for both breast cancer and colon-rectal cancer that TIL can be an important prognostic factor to identify patients with a better outcome independent of the tumour stage910. The in situ evaluation of the immune cell infiltrate, termed as “immunoscore”, has revealed significant prognostic value. Both proteomics and transcriptomics have confirmed the involvement of the immune system, both the innate and the adaptive arm, in solid tumours. As for the immune infiltrate, among T lymphocytes, the two major populations of αβ and γδ T cells, should be considered as well as T helper (Th) 1 lymphocytes mainly producing tumour necrosis factor (TNF)α and interferon (IFN)γ, Th2 or Th17 (IL4 or IL17) and eventually regulatory T cells (Tregs) secreting TGFβ and/or IL1017. In particular, γδ T cells are good mediators of a stress-related response: the exposure of “stress signals”, can occur due to cell damage, including tumour transformation17. Among the stress molecules involved in this type of immune response, there are the major histocompatibility complex (MHC)-class-I related molecules MIC-A and MIC-B and the UL16 binding proteins (ULBPs) also called NKG2D ligands (NKG2D-L)1718 (Figure). Both αβ cytolytic T and γδ T lymphocytes can interact with NKG2D-L through the NKG2D receptor: this interaction leads to an activating signal that makes T lymphocytes promptly able to exert their effect or function, i.e. proliferation, production of anti-tumour cytokines (such as IFNγ, or TNFα), or release of lytic enzymes to destroy tumour cells1718. On the other hand, NKG2D-L can be released by tumour cells and, in their soluble form, bind to NKG2D receptor without delivering the activating signal, but rather blocking the ability to recognize membrane NKG2D-L expressed by cancer cells. We have reported that MSC derived from the bone marrow or from the lymph nodes of lymphoma patients inhibit the generation of anti-tumour effector-memory CD8+αβT and γδT cells, the Th1 lymphocyte-associated cytokine pattern and the NKG2D-mediated killing of lymphoma cells18. At the tumour site, this is due to the secretion of TGFβ by MSC, counteracting IL15 and leading to the impairment of NKG2D-mediated recognition of tumour cells19. Preliminary results indicate that MSC from colon-rectal cancer can inhibit αβ andγδ T cell proliferation and the CD3-T cell antigen receptor-mediated cytotoxicity19.
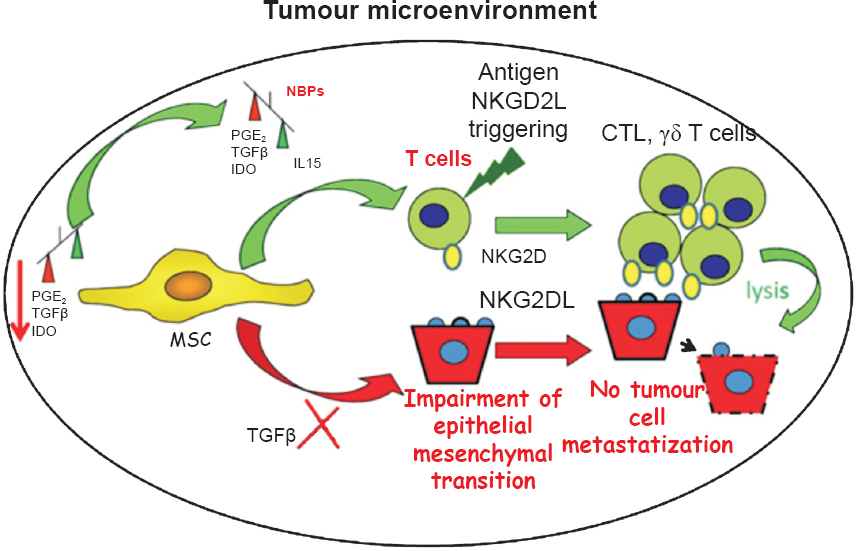
- Role of mesenchymal stromal cells (MSC) in tumour microenvironment: priming with aminobisphosphonates can trigger anti-tumour immunity. MSC through different soluble factors as prostaglandin E2 (PGE2), indoleaminedioxigenase (IDO) and transforming growth factor (TGF)β can downregulate anti-tumour immune response triggered through NKG2D-NKG2DL interaction. In addition, TGFβ can stimulate epithelial mesenchymal transition (EMT) and further metastasization of tumour cells. The priming of MSC with aminobishosphonates (NBPs) induces an imbalance between the production of TGFβ and interleukin (IL)15. TGFβ is an immune regulating factor compared with the immunostimulation elicited with IL15. This leads to the triggering, rather than inhibition, of anti-tumour immune response with the consequent tumour cell killing. Cytolytic T lymphocytes (CTL) and γδ T cells are the main effector mediators of tumour cell elimination. Further, the reduction in TGFβ production can impair the EMT and the consequent metastasization of tumour cells.
Aminobisphosphonates as drugs able to render MSC immunostimulating rather than immunosuppressive: In principle, two different approaches can be employed to target MSC: the first one is to eliminate MSC using cytotoxic drug; the second one is to render MSC immunostimulating rather than immunosuppressive. The use of cytotoxic drugs is greatly impaired because tumour MSCs do not show peculiar difference from healthy MSCs. It has been recently shown20 that lymph node MSC derived from non-Hodgkin's lymphoma patients pulsed with aminobisphosphonates as zoledronic acid can trigger, rather than inhibit, host γδT cell proliferation. In addition, these MSCs reduce the expression and secretion of TGFβ production but enhance the IL15 expression. This imbalance between TGFβ and IL15 leads to the generation of effector γδT cells able to lyse more efficiently tumour lymphoma cells20. EMT is partly induced by TGFβ1520 suggesting that the lower degree of TGFβ production displayed by zoledronate-pulsed MSC can influence also tumour EMT limiting tumour cell expansion and metastasization. It is to remark that zoledronate is commonly used for osteoporosis in post-menopausal women, thus its use to trigger immune response in breast cancer influencing MSC behaviour would be a suitable therapeutic tool. This idea is in line with what is found using thalidomide and its derivative immunomodulatory drugs (IMIDs)21. These drugs are efficient in impairing the growth and expansion of multiple myeloma cells eliciting an anti-myeloma immune response influencing stromal cell behaviour of bone marrow21.
Conclusions
MSCs localized in tumour microenvironment can promote through TGFβ the EMT that facilitate the generation of metastasis and can downregulate innate and adaptive immune responses. Thus, MSC can be a suitable target for tumour therapy both using drugs which impair the MSC-mediated inhibitions by eliminating MSC or try to switch the MSC-mediated immune suppression into an activation. Whether targeting of MSC is useful in cancer treatment and is safe for the patient are still to be defined. However, the identification of surface molecules expressed selectively by tumour associated MSCs and the selection of drugs that can revert MSC behaviour, can aid in planning the treatment of several cancers, affecting the fate of tumour cells and relieving the immunosuppressive microenvironment of the tumour.
References
- Population-based incidence and patterns of cancer in Kamrup Urban Cancer Registry, India. Natl Med J India. 2013;26:133-41.
- [Google Scholar]
- Rural urban differences in breast cancer in India. Indian J Cancer. 2014;51:277-81.
- [Google Scholar]
- Indian Council of Medical Research consensus document for the management of colorectal cancer. Indian J Med Paediatr Oncol. 2014;35:192-6.
- [Google Scholar]
- Combining immunotherapy and targeted the rapies in cancer treatment. Nat Rev Cancer. 2012;12:237-51.
- [Google Scholar]
- Diverse mechanisms regulate the surface expression of immunotherapeutic target ctla-4. Front Immunol. 2014;5:619.
- [Google Scholar]
- Therapeutic uses of anti-PD-1 and anti-PD-L1 antibodies. Int Immunol. 2015;27:39-46.
- [Google Scholar]
- Clinical blockade of PD1 and LAG3 - potential mechanisms of action. Nat Rev Immunol. 2015;15:45-56.
- [Google Scholar]
- The continuum of cancer immuno surveillance: prognostic, predictive, and mechanistic signatures. Immunity. 2013;39:11-26.
- [Google Scholar]
- CD3+, CD4+& CD8+tumour infiltrating lymphocytes (TILs) are predictors of favourable survival outcome in infiltrating ductal carcinoma of breast. Indian J Med Res. 2014;140:361-9.
- [Google Scholar]
- Mechanisms of tumour escape from immune system: role of mesenchymal stromal cells. Immunol Lett. 2014;159:55-72.
- [Google Scholar]
- Role of epigenetic mechanisms in epithelial-to mesenchymal transition of breast cancer cells. Transl Res. 2015;165:126-42.
- [Google Scholar]
- Immunomodulatory properties of mesenchymal stromal cells. Blood. 2007;110:3499-506.
- [Google Scholar]
- Mesenchymal stromal cell “licensing”: a multistep process. Leukemia. 2011;25:1408-14.
- [Google Scholar]
- TGFβ in T cell biology and tumour immunity: Angel or devil? Cytokine Growth Factor Rev. 2014;25:423-35.
- [Google Scholar]
- Stress immunity in lymphomas: mesenchymal cells as a target of therapy. Front Biosci. 2014;19:281-90.
- [Google Scholar]
- How to exploit stress-related immunity against Hodgkin's lymphoma: targeting ERp5 and ADAM sheddases. Oncoimmunology. 2013;2:e27089.
- [Google Scholar]
- High ERp5/ADAM10 expression in lymph node microenvironment and impaired NKG2D ligands recognition in Hodgkin's lymphomas. Blood. 2012;119:1479-89.
- [Google Scholar]
- Aminobisphosphonates prevent the inhibitory effects exerted by lymph node stromal cells on anti-tumour Vδ 2 T lymphocytes in non-Hodgkin lymphomas. Haematologica. 2014;99:131-9.
- [Google Scholar]
- Pomalidomide: the new immunomodulatory agent for the treatment of multiple myeloma. Blood Cancer J. 2013;3:e143.
- [Google Scholar]




